-
STLS: Basics of TB and NTEP
Fullscreen-
STS: TB & TB Epidemiology
FullscreenTuberculosis
Content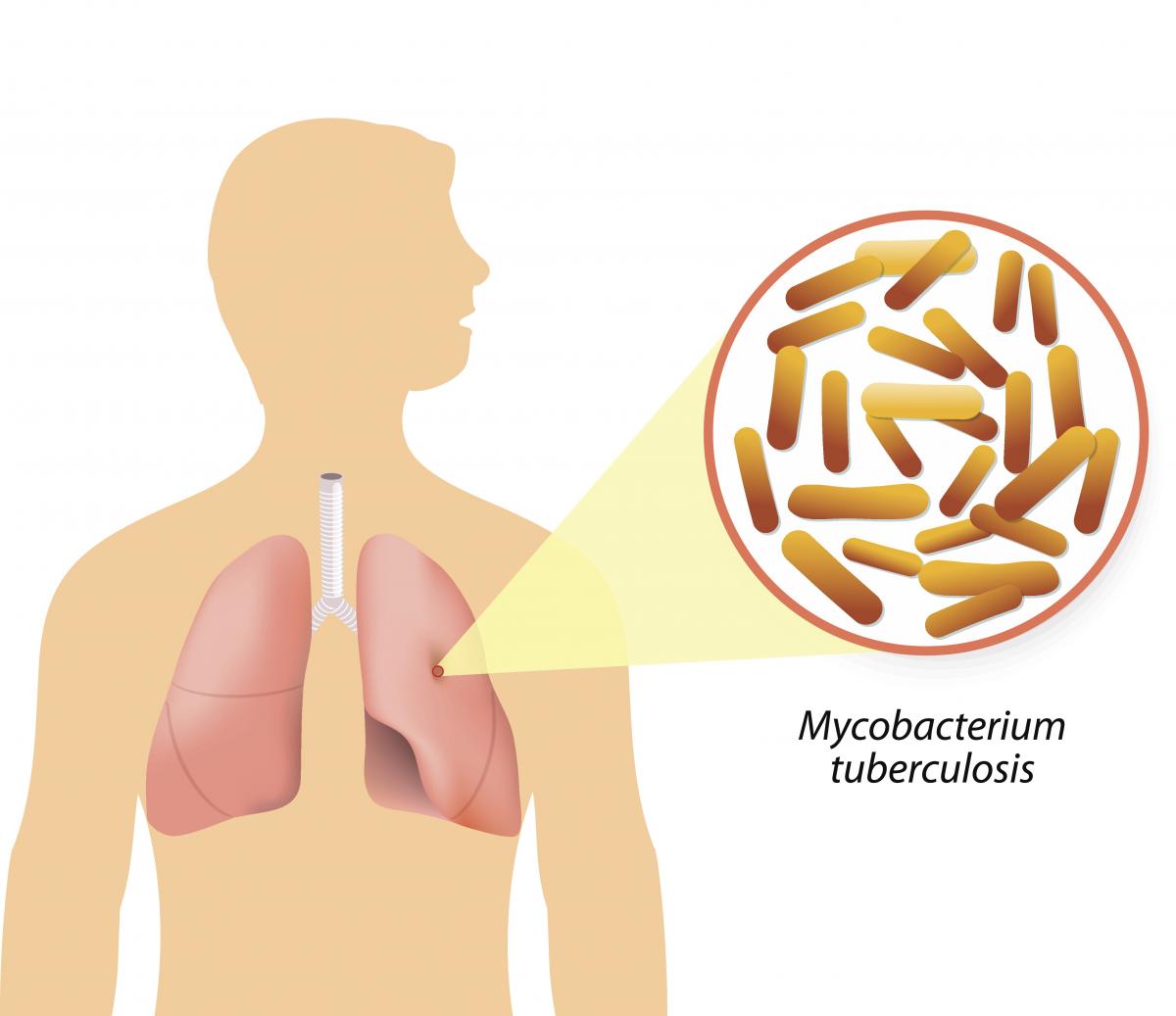
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB-HIV BURDEN
ContentThe interaction between HIV and TB in co-infected persons is bidirectional and synergistic; on the one hand, HIV infection predisposes the development of active TB, and, on the other, the course of HIV-related immunodeficiency is worsened by active TB infection.
Globally and in India, TB is the most common opportunistic infection seen in HIV patients and a leading cause of death in these patients. The lifetime risk of TB in immune-competent persons is 5-10%, whereas, in an HIV-infected person, the annual risk of TB is 5-15%. Thus, people living with HIV are 18 (15-21) times more likely to develop active TB disease than people without HIV.
TB and HIV Burden Trends in India
India is one of the WHO’s 30 high TB/HIV burden countries; of the 3 million TB incident cases, close to 54000 occurred in HIV-infected persons (See Table 1 for more details). TB and HIV are major public health challenges in India and are leading causes of mortality and morbidity among all other infectious diseases.
Table 1: Comparison between global and Indian TB/HIV burden estimates, Source: WHO Global TB Report 2022 INDICATORS GLOBAL ESTIMATES INDIA ESTIMATES Total TB Incidence 11 million 3 000 000 HIV-positive TB Incidence 703 000 54 000 HIV-positive TB Mortality 187 000 11 000 Resources
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Epidemiological Triad of TB
ContentThe Epidemiologic Triad is a model used in the field of epidemiology to study diseases and how they are spread. It consists of a triangle with three vertices or corners.
The three vertices for infectious diseases consist of:
1. Agent, or microbe that is the factor causing the disease.
2. Host, or organism harbouring the disease.
3. Environment, or those external factors that cause or allow disease transmission.
In the Epidemiological Triad of TB (Figure), the agent is the TB causing bacteria Mycobacterium tuberculosis; the host refers to humans that are susceptible to TB. Susceptibility or the risk factors for acquiring TB can be:
- Close contact with a person having TB disease
- Nutritional status of the host
- Existing co-morbidities
- Low immunity.
Susceptibility of the host can also vary due to age, gender, genetic composition, race, ethnicity, etc.
As TB is an airborne disease, environmental factors come into play for the transmission of TB. These include crowding, poor ventilation, bad sanitation, indoor air pollution, etc.
The understanding between the interplay of agent, host and environment is essential to understanding the epidemiology of TB and taking measures to control it. The risk of TB due to environmental factors can be reduced by practising airborne infection prevention measures like good ventilation, hand hygiene and cough etiquette.

Figure: Epidemiological Triad of TB
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The three vertices of the Epidemiological Triad are agent, host and environment.
TRUE FALSE 1 The three vertices of the Epidemiological Triad are agent, host and environment.
Yes Yes Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
Chemotherapy and its implication in TB control
ContentChemotherapy for TB is the use of an anti-TB drugs to kill, or prevent the replication of, TB mycobacteria in the patient’s body. Effective anti-TB chemotherapy renders the patient non-contagious and cures the patient, thereby interrupting the chain of transmission. Mortality rates of TB range from 50-80% in untreated smear-positive individuals and drop to lower than 5% under chemotherapy.
Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment. TB disease must be treated for at least 6 months and in some cases even longer. The use of multi-drug therapy reduces the incidence of drug-resistant cases and increases the overall effectiveness of treatment.
If treatment is interrupted, any surviving bacteria may cause the patient to later become ill and infectious again, potentially with drug-resistant disease.
How infectious are tuberculosis patients under chemotherapy?
Under effective chemotherapy, there is a substantial decline in infectiousness in two weeks time, and may not be a major source of risk to any contacts. This decline is indicated by the rapid fall in the number of viable organisms in the sputum, and reduced frequency of coughing.
Types of Chemotherapy in TB
- Preventive Chemotherapy: Regimen for healthy but TB infected persons with a high risk of developing TB, in order to prevent them from developing TB.
- Standard Chemotherapy: Two-phased chemotherapy for an average of 6-8 months based on the combination of at least four major drugs (HRZE) given for 2 months during the initial intensive phase of treatment and followed by a combination of at least 2 drugs given for at least 4 months during the continuation phase of treatment.
- Chemotherapy for Drug-resistant TB: Two-phased chemotherapy varying from 9 - 24 months in patients having demonstrated resistance to drugs used in standard chemotherapy. The regimen varies with the drug to which the resistance is present, however, each regimen contains a mix of second-line anti-TB drugs including injectables.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Infectiousness and Host Susceptibility, The Journal of Infectious Diseases, Vol. 216, suppl_6, 2017.
- Tuberculosis chemotherapy: Current Drug Delivery Approaches, Respiratory Research 7, Article no. 118, 2006.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which type of chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB? First-line anti-TB drugs Preventive Chemotherapy Standard Chemotherapy Chemotherapy for Drug Resistant-TB 2 Preventive chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB. Yes Yes Incidence of TB Disease
ContentIncidence is an epidemiological measure of the occurrence of new cases of a disease in a population over a specified period of time. Tuberculosis (TB) incidence is the number of new cases of active TB disease during a certain time period (usually a year), and is better expressed as a rate, as shown in the figure below.


Figure: Deriving the Incidence of TB Disease for a Given Population
Tuberculosis incidence varies considerably in different populations and population segments.
In 2021, the Global TB incidence was 134 (125-143) per 100,000. The TB Incidence rate of India is - 210 (178-244) per 100,000 in 2021 according to WHO Global TB Report 2022.
Resources
- India TB Report, 2022.
- Epidemiologic Basis of Tuberculosis Control, Hans L. Rieder, 1999.
- Morbidity Frequency Measures, Centers for Disease Control and Prevention.
- Global Tuberculosis Report 2022.
Prevalence of TB Disease
ContentPrevalence is an epidemiological measure of the proportion of a population with a disease or a particular health condition at a specific point in time (point prevalence) or over a specified period of time (period prevalence).
Tuberculosis (TB) prevalence refers to the number of people with TB that are present in a particular population at a given time. Calculation of the TB prevalence rate is shown in the figure below.

Figure: Deriving the Prevalence of TB Disease for a Given Population
TB prevalence rate is derived by adding the number of persons that develop new TB disease (i.e., incident cases) and those who already have the disease (i.e., existing cases), and dividing the sum by the total population from which the cases arose.
TB prevalence varies widely and is affected by a number of factors such as age, gender, population density, rural/urban settings, as well as socioeconomic factors.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
TB Notification rate
ContentTB notification rate is the number of TB cases notified over a specified time period for a specified population, usually per lakh. It indicates how many cases have been diagnosed and informed to the National TB Elimination Program.
It is mostly calculated annually, and the calculation formula is as follows:

Figure: Deriving the Annualized TB Case Notification Rate
The National TB Elimination Program calculates TB notification rates based on TB cases notified using the digital surveillance system called Nikshay. Each state/district is provided with an annual target for TB case notification, the progress of which is measured periodically to understand efforts taken for the detection of TB cases.
Example
If the number of TB patients diagnosed in District X one year is 1000, and the mid-year population of District X is 10,00,000, then the annualized TB case notification rate is calculated as follows:
100 cases/100 000/year
Resources
-
STLS: NTEP
FullscreenEnd TB strategy
ContentThe World Health Organisation End TB Strategy, adopted by the World Health Assembly in 2014, aims to end the global TB epidemic. The strategy draws on the opportunities presented by the Sustainable Development Goals (SDGs), especially those goals aimed at achieving universal health coverage and social protection from disease.
The table given below provides information on the vision, goal, milestones and targets for the End TB Strategy.
Table: Details on the End TB Strategy; Source: The End TB Strategy, World Health Organisation, 2015, p2. Vision of the End TB Strategy A world free of TB:
- Zero TB deaths
- Zero TB disease cases
- Zero suffering due to TB
Goal of the End TB Strategy To end the global TB epidemic by 2035 End TB Milestones for 2025 - 75% reduction in tuberculosis deaths (compared with 2015)
- 50% reduction in tuberculosis incidence rate (less than 55 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
End TB Targets for 2035 - 95% reduction in tuberculosis deaths (compared with 2015)
- 90% reduction in tuberculosis incidence rate (less than 10 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
The National Strategic Plan (2017-2025) proposes bold strategies with commensurate resources to rapidly decline TB in the country by 2030 in line with the global End TB targets to attain the vision of a TB-free India.
Resources
- National Strategic Plan for Tuberculosis Elimination 2017–2025.
- The End TB Strategy, World Health Organisation, 2015.
Sustainable Development Goals [SDGs] related to TB
Content
Figure: Summary of the Sustainable Development Goals
- Goal 3 is related to Good Health and Well-being. It mentions that 'Each nation needs to ensure healthy lives and promote the well-being of all ages'.
- The United Nations Sustainable Development Goals (SDGs) include ending the TB epidemic by 2030 under Goal 3.
- Goal 3.3: By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.
India is a signatory of the United Nations Sustainable Development Goals and has targeted TB elimination by 2025, five years ahead of the SDG timeline.
Resources
Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Training and Demonstration Centre [STDC]
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
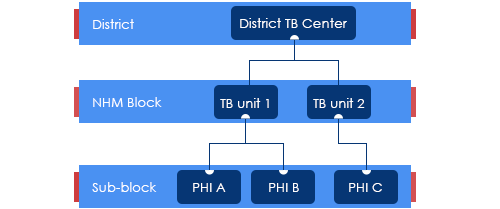
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Drugs Stores in NTEP
ContentImage
DRUG STORE
Central TB Division, MoHFW, has
Under NTEP, there is a large network of drug stores across the country to ensure a regular and uninterrupted supply of drugs and consumables. The Drugs and consumables are procured at the Central level and supplied at Central warehouses (GMSDs & CMSS); further drugs and consumables are supplied to the State Drug Stores and further dissemination to district and sub-district levels following the stocking norms to ensure uninterrupted supply of drugs and consumables to the patient.
To provide overall policy guidance and coordination, the Procurement and Supply Chain Management (PSM) Unit has been established at Central TB Division (CTD), MoHFW, for procurement and Supply Chain Management of all types of anti-TB drugs, diagnostics and consumables.
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Interaction of STLS with TB Patient Care Ecosystem
ContentThe Senior Tuberculosis Laboratory Supervisor (STLS) interacts with the TB patient care ecosystem from the time a presumptive TB case is identified, examined, diagnosed, notified, and put on anti-tuberculosis treatment till the completion of treatment.
The key interactions include:
- Coordination with the Medical Officer (MO) of various dispensaries and other health establishments to ensure referral of the presumptive TB cases to the Designated Microscopy Centers (DMCs) and Nucleic acid amplification test (NAAT) laboratories for diagnosis of TB and DR-TB.
- Coordination with laboratory technicians of the DMCs and NAAT laboratories for results of TB diagnosis, follow-up, and sending samples for further testing to the designated Intermediate Reference laboratories (IRLs).
- STLS is also responsible for providing monthly supply of staining regents, consumables, NAAT cartridges and chips to the LTs of the DMC and NAAT Laboratories.
- STLS is the key person for ensuring quality assured TB diagnosis in the district. This is done by performing activities like On-site evaluation (OSE) visits, Random Blinded Rechecking (RBRC) of smears and providing quality assured staining reagents to the DMCs.
- STLS is also responsible for providing monthly supply of staining regents, consumables, NAAT cartridges and chips to the LTs of the DMC and NAAT Laboratories.
- Coordination with Senior Treatment Supervisor (STS) to ensure that all TB patient diagnosed are initiated on treatment.
- Coordination with STS and PMDT Coordinator in updation of relevant NTEP records, line-list of presumptive DR-TB patients and preparation of Quarterly Reports
- The STLS interacts with the health care staff to facilitate change management with respect to use of Information and Communications Technology (ICT) and Ni-kshay tools for concerned data entry, validation & its use for public health action.
- STLS ensures that the laboratory results related to diagnosis and subsequent follow-ups are updated by the LTs in a timely manner.
- STLS ensures that the laboratory results related to diagnosis and subsequent follow-ups are updated by the LTs in a timely manner.
- STLS constantly Interacts with the District Drug Store (DDS), pharmacist and District TB Centre (DTC) to ensure adequate supply of CBNAAT cartridges and Truenat Chips to the NAAT laboratories and also keeps a track of transaction related to receipt and dispatch of these Cartridges and Chips.
- This process is undertaken by the use of Ni-kshay Aushadhi. SLTS uses Ni-kshay Aushadhi for request generation, inventory management, and issue of cartridges and Chips to NAAT laboratories.
- This process is undertaken by the use of Ni-kshay Aushadhi. SLTS uses Ni-kshay Aushadhi for request generation, inventory management, and issue of cartridges and Chips to NAAT laboratories.
- The STLS supports assigning treatment support centers and treatment supporters for the patient. The treatment supporters may be community volunteers accessible, willing, and acceptable to the patient and who can be accountable to the health system. These include Anganwadi workers, dais, teachers, panchayat leaders, religious leaders, and others.
- The STLS coordinates with District TB Officer (DTO) and DTC to conduct monthly and quarterly review meetings.
- The STLS is crucial in undertaking active case finding activities and organizing community-based Information, Education and Communication (IEC) activities like patient-provider group interaction meetings and community meetings in coordination with the support of field staff, which includes the ASHA workers, Community Health Officer (CHO), Multipurpose Health Worker (MPHW), and Auxiliary Nursing Midwife (ANM).
- The STLS coordinates with the private health care settings including the standalone laboratories in the districts to ensure that the patients diagnosed in these facilities are notified to the programme and appropriate public health action is taken when required.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test STLS helps the DTO in organising review meetings. True False True The STLS coordinates with District TB Officer (DTO) and DTC to conduct monthly and quarterly review meetings. - Coordination with the Medical Officer (MO) of various dispensaries and other health establishments to ensure referral of the presumptive TB cases to the Designated Microscopy Centers (DMCs) and Nucleic acid amplification test (NAAT) laboratories for diagnosis of TB and DR-TB.
-
STLS: Integration of NTEP with Health System
FullscreenNational Health Mission [NHM]
ContentThe National Health Mission (NHM) was launched by the Government of India in 2013, subsuming the National Rural Health Mission (NRHM) and National Urban Health Mission (NUHM). Figure 1 shows the history of the NHM.
The vision of NHM is “Attainment of Universal Access to Equitable, Affordable and Quality health care services, accountable and responsive to people's needs, with effective intersectoral convergent action to address the wider social determinants of health.”
Image
Figure 1: History and Make-up of the NHM; Source: Annual Report 2015-16, Ministry of Health and Family Welfare (MoHFW)
NHM further aims to support the existing national programmes of health and family welfare (Figure 2) including reproductive and child health, malaria, blindness control, iodine deficiency, filariasis, kala-azar, tuberculosis (TB), leprosy, and integrated disease surveillance.
Image
Figure 2: Health Programs Supported by NHM NHM and the National Tuberculosis Elimination Program (NTEP)
Integrating the NTEP with the health system increases the effectiveness and efficiency of TB care and control. India's TB control programme has been mainstreamed efficiently with the NHM.
The overall responsibility for the financial management of the NTEP is with the MoHFW, Director General of Health Services (DGHS) through the NHM.
At the state level, the State Health Society or its equivalent under the NHM of the state manages the financing of the TB Control Programme.
At the sub-district level, the TB Unit (TU) is the nodal point for TB control activities. TUs are based mainly in NHM health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
Resources
Medical Colleges
ContentMedical colleges in the country are integrated with the National TB Elimination Programme (NTEP) to widen access and improve the quality of TB services. Medical colleges provide specialized services for seriously ill TB patients.
The integration of medical colleges in the program is in a structured task force mechanism at different levels:
- National
- Zonal
- State
One national and six zonal task forces have been formed under the programme along with task forces for all states. A core committee is also formed in each medical college. These task forces are created with defined roles and responsibilities for the effective involvement of medical colleges in the programme.

Core Committee
Every medical college will have core committees representing various hospital departments and NTEP nodal officers. These committees meet quarterly and review the implementation of the program in the medical college.
Functions of the core committee:
- They organise sensitisation workshops and training for faculty members, postgraduates, undergraduates, interns, paramedical staff, etc.
- Ensure that teachings on TB/ NTEP form part of the curriculum for all medical colleges.
- Coordinate between various departments so that patients get the services under one roof.
- Coordinate with the district TB programme.
Role of Medical College in NTEP
- Medical colleges coordinate with the district TB programme for participation in quality assurance, supervision, monitoring, review and evaluation.
- Operational research is one of the important activities of medical colleges.
- Every medical college should have TB detection facility and treatment support centres. These centres are equipped with trained additional human resources such as medical officers, laboratory technicians and TB health visitors.
- The National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients.
- Medical colleges undertake advocacy for the programme.
- Medical colleges also functions as peripheral health institutes (PHI), maintain TB notification registers and submit monthly PHI reports: They have Nikshay user access and need to enter TB-related data on a real-time basis.
Resources
RNTCP Technical and Operational Guidelines for Tuberculosis Control in India, 2016.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Every medical college should have a DR-TB facility? True False 1 National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients. Need for integration of NTEP with Health System
Content-
The public health system in India through the National Health Mission (NHM) visualises the attainment of Universal Health Coverage (UHC) for all its citizens, which provides access to equitable, affordable and quality health care services, which is also accountable and responsive to the needs of the people.
-
Under the umbrella of NHM, the National TB Elimination Programme (NTEP) ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI).
-
Furthermore, the NHM, under the Ayushman Bharat initiative has taken measures to strengthen the primary care facilities including Primary Health Centres (PHCs) and Sub Health Centres (SHCs) in the Ayushman Bharat Health & Wellness Centres (AB-HWCs).
Need for integration of NTEP with the Health System at Different Levels
- Closer to community TB Services: The integration of TB services with the health system provides an opportunity for the TB programme to leverage the resources under the Ayushman Bharat initiative to take TB interventions closer to the community which were otherwise provided at the primary care level.
- Improved population coverage: Active empanelment and HWC database will help to monitor and identify the left-out population and contribute significantly to the NTEPs case finding activity coverage.
- Improved population health outcomes: Improved availability, access and utilisation of advanced TB treatment services under the ambit of UHC is essential in reducing morbidity and mortality from TB which may in turn also contribute to overall equitable health outcomes.
- Reduced out-of-pocket expenditure: The integration will improve the access to TB services, assure within-reach TB medicines and diagnostic services, provide linkages for care coordination with Medical Officers/ specialists across various levels of care, etc., all of which will reduce the catastrophic expenditures faced by the patients and their families.
- Decreased crowding at the secondary and tertiary health facilities: A strong network of peripheral level TB care services would facilitate in reduction of the overcrowding and the case burden at the secondary and tertiary facilities, which could be utilised for cases with follow-up referral to higher level facilities.
- Increased responsiveness and addressal of social determinants of TB: Provision of TB treatment at the nearest point of care for the communities and engaging the most peripheral workers from the health system like the Accredited Social Health Activists (ASHA) in the TB programme may lead to comfort in accessing the care by the patients and also enable addressing psycho-social determinants of TB.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, CTD, MoHFW, India, 2020.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). True False 1 Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). Yes Yes -
-
-
STLS: TB Diagnosis and Case finding
Fullscreen-
STLS: Diagnostic Technologies
FullscreenTesting for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
Cartridge Based Nucleic Acid Amplification Test [CBNAAT]
ContentCartridge Based Nucleic Acid Amplification Test (CBNAAT) is a rapid molecular diagnostic test. It is used for diagnosis of Tuberculosis (TB) and Rif-resistant Tuberculosis (RR-TB) in NTEP. Results are obtained from unprocessed sputum samples in about 2hours which helps in early detection and treatment of TB patients.
India has vast number of CBNAAT laboratories which are utilized for TB/RR-TB detection and Universal Drug Susceptibility Testing (UDST) under the National TB Elimination Program (NTEP).

Figure: CBNAAT Cartridge and Machine in Use (Image courtesy: USAID supported Challenge TB Project)
The CB-NAAT system detects DNA sequences specific for Mycobacterium tuberculosis complex and rifampicin resistance by Polymerase Chain Reaction (PCR). It concentrates Mycobacterium tuberculosis bacilli from sputum samples, isolates genomic material from the captured bacteria by sonication and subsequently amplifies the genomic DNA by PCR. The process identifies clinically relevant rifampicin resistance-inducing mutations in the RNA polymerase beta (rpoB) gene in the Mycobacterium tuberculosis genome in a real-time format using fluorescent probes called molecular beacons.
Video fileVideo: Cartridge-Based Nucleic Acid Amplification Test [CBNAAT] - GeneXpert Technology
Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- India TB Report 2021, National TB Elimination Program (NTEP), MoHFW, 2021.
Assessment Questions
Question
Answer 1
Answer 2
Answer3
Answer 4
Correct Answer
Correct explanation
Part of pre-test
Part of post-test
Under NTEP, CBNAAT is offered upfront for which of these categories?
PLHIV
Paediatric presumptive TB
Presumptive DR-TB
All of the above
4
Under NTEP, CBNAAT is recommended upfront for People living with HIV, Paediatric Presumptive TB patients, Presumptive DR-TB patients and patients notified from the Private sector.
Yes
Yes
CBNAAT requires the processing of sputum samples before testing
True
False
2
Results are obtained from unprocessed sputum samples in about 2hours from a CBNAAT machine
Yes
Yes
Line Probe Assay [LPA]
ContentLine Probe Assay (LPA) is a rapid molecular test available at centralised laboratories.
The assay is based on Polymerase Chain Reaction (PCR) that can simultaneously detect Mycobacterium tuberculosis complex as well as drug sensitivity to anti-TB drugs.

Figure 1: The GenoType MTBDRplus Molecular LPA Procedure; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Advantages of LPA
- Rapid molecular test. (Turnaround time: 3-5 days)
- Highly sensitive and specific.
- Performed directly from sputum smear-positive specimens and on isolates of M. tuberculosis complex grown from smear-negative and smear-positive specimens.
- Detects multiple gene mutations in anti-TB drugs.
- First-line LPA detects mutations to rifampicin and isoniazid
- Second-line LPA detects mutations to fluoroquinolones and aminoglycosides.
- Suitable for low and high-throughput labs.
Disadvantages of LPA
- Cannot be used as a point-of-care test.
- Requires appropriate laboratory infrastructure, equipment and biosafety precautions.
- Different rooms (DNA extraction, pre-amplification, amplification, post-amplification/ hybridization) are required to perform different steps (Figure 2).
- Requires trained manpower to perform tests and interpret test results.
- Stringent internal quality control is required to prevent contamination.

Figure 2: Amplification (A) and Post-amplification Laboratory (B) for LPA; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Resources
- Guidelines for PMDT in India, 2021.
- Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test LPA can be used as a point-of-care test. True False 2 LPA cannot be used as a point-of-care test. Yes Yes Solid and Liquid Culture in TB
ContentCulturing TB Bacilli is well known and historic method for detection/ confirmation of Tuberculosis. It is a highly sensitive and specific phenotypic test; it can detect even a few viable bacilli in the sample (Upto 10 Colony Forming Units- CFUs). TB bacilli multiply in the culture and form colonies of TB bacilli which can are easily be identified.
Based on the growth media used Culture is divided in to two types, Solid and Liquid Culture methods. Types Culture:
- Solid Culture on Lowenstein Jensen media : Historic gold standard culture test. Results take usually upto 2 months (60 days).
- Modern Liquid culture systems: (e.g. BACTEC MGIT 960, BacT Alert or Versatrek etc.) Results take usually up to 42 days.
Uses
- Solid culture is the gold standard diagnostic test for TB. But it is not used for the purpose of TB diagnosis due to the long turn around time of 2 months. It is largely used for research purposes where it is used as the baseline test on which the sensitivity and specificity of other tests are calculated.
- Liquid Culture is being used for follow-up monitoring of patients on drug resistant TB treatment to detect treatment failure. Liquid culture is also used for long term follow up patients who have successfully completed treatment to detect recurrence.
- Liquid culture is used as a previous step to grow bacilli and obtain isolates prior to Drug Susceptibility Testing.
- Liquid cultures are also used in TB prevalence surveys for its high sensitivity and specificity
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Culture Drug Susceptibility Testing [CDST]
ContentCulture Drug Susceptibility Testing (CDST) is a growth-based phenotypic method used to check the susceptibility of Mycobacterium tuberculosis strains to various first and second line anti-TB drugs. Mycobacterial resistance to a particular drug is identified if there is growth observed in culture in presence of that drug.

In NTEP CDST is the standard method to detect resistance in samples of patients who have tested positive on followup. While CDST is possible on both Solid and Liquid culture, currently, the NTEP utilizes only liquid culture as a method for DST, due to faster Turn around times.
CDST testing services are available under NTEP in designated, specialized laboratories called CDST Labs both in public and private sector. Currently there are 80 such laboratories (60 certified for First Line and 49 for Second line drugs). Such designated laboratories are subject to regular external quality assessment, often by the National Reference Laboratory at that region.
Quality assured DST to R, H, Z, Mfx, Lfx, Lzd, Am, Km and Cm are available across the country.
Resources
-
STLS: Diagnostic Network and Hierarchy
FullscreenLaboratory Hierarchy and Network
ContentNTEP laboratory network is comprising of National Reference Laboratories (NRLs), state level Intermediate reference laboratories (IRLs), Culture & Drug Susceptibility Testing (C & DST) laboratories and peripheral level laboratories. Peripheral level laboratories consist of designated microscopy centres (DMCs) and NAAT labs.
NTEP has a quality assured laboratory network for bacteriological examination of sputum in a 3-tiered system.
Figure: Laboratory network of NTEP
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Roles of NRLs
Content- National Reference Laboratories (NRLs) conducts annual on-site evaluation/supervisory visits to laboratories for assessing the quality of microscopy, culture and drug susceptibility test (C&DST), and for improvement of the overall laboratory quality.
- NRLs also assist Central TB Division (CTD), in developing laboratory guidelines, standard operating procedures (SOPs), and conduct training to state-level Intermediate reference laboratories (IRLs) and other technical issues.
- NRLs conduct C&DST training to the IRLs, and develop SOPs for the technical procedures, equipment maintenance, infection control and recording and reporting.
- NRLs are also responsible for offering second-line drug susceptibility tests (DST) for multi-drug resistant TB (MDR-TB) treatment failures.
- NRLs are responsible for the accreditation of the mycobacteriology laboratory for culture and drug sensitivity testing under the National Tuberculosis Elimination Program (NTEP).
- In addition, NRLs are also responsible for the conduct of research for the programme and evaluation of newer tools for the diagnosis of TB.
- The National Institute for Research in Tuberculosis (NIRT) Chennai, the Supranational Reference Laboratory (SRL) of the region is responsible for the external quality assurance of the other 5 NRLs. NIRT is in turn quality-assured through the SRL coordinating laboratory at Antwerp, Belgium.
Assessment Questions
Question
Answer 1
Answer 2
Answer3
Answer 4
Correct Answer
Correct explanation
Part of pre-test
Part of post-test
What are the functions of National Reference Laboratories?
Providing Culture and DST training to the IRLs
Developing SOPs for the technical procedures
Offering second-line DST
All of the above
4
All the functions stated are performed by the National Reference Laboratories.
Yes
Yes
Which institute is responsible for the external quality assurance of NRLs?
SRL
CTD
National Institute for Research in Tuberculosis, Chennai
National Tuberculosis Institute, Bangalore
3
The National Institute for Research in Tuberculosis (NIRT) Chennai, the Supranational Reference Laboratory (SRL) of the region is responsible for the external quality assurance of the other 5 NRLs. NIRT is in turn quality-assured through the SRL coordinating laboratory at Antwerp, Belgium.
Yes
Yes
Roles of IRLs
ContentThe Intermediate Reference Laboratories (IRLs) function as a culture and drug susceptibility testing (C&DST) facility for the state level.
In addition to performing CDST, IRL is also responsible for:
- Undertaking training on laboratory technologies for district and field level staffs
- Conducting on-site evaluation visits to districts for sputum microscopy at least once a year
- Undertaking panel testing of Senior TB Laboratory Supervisors (STLS) at each district linked to it
- Ensuring the proficiency of staff performing National Tuberculosis Elimination Programme (NTEP) smear microscopy activities by providing training to laboratory technicians and STLS
Resources
- Guidelines for Programmatic Management of Drug-resistant TB in India, 2021.
- NTEP Laboratory Network.
Kindly provide your valuable feedback on the page to the link provided HERE
CDST labs and their role
ContentUnder the National Tuberculosis Elimination Programme (NTEP), many labs are established at the regional level within states for providing Culture and Drug Susceptibility Testing (C&DST) facilities for presumptive TB/DRTB and for TB/DRTB patients.
- C&DST laboratories are mostly located in intermediate reference laboratories (IRLs) or medical colleges.
- There are 42 C&DST laboratories established under the programme in different geographies.
- Dedicated human resources are provided for the laboratories under the programme.
- Districts are linked with laboratories for providing facilities for Culture and DST using:
- Phenotypic Methods (Solid – Lowenstein Jensen (LJ), and Liquid Culture – Mycobacteria Growth Indicator Tube (MGIT))
- Genotypic technology (Line Probe Assay (LPA) and Cartridge Based Nucleic Acid Amplification Test (CBNAAT))

Figure: Culture and Drug Susceptibility Testing (C&DST) facility,
Source: The Foundation For Innovative New Diagnostics (FIND)Resources
- Guidelines for Programmatic Management of Drug Resistant TB in India, 2021
- Training Modules (1-4) for Programme Managers and Medical Officers; New Delhi, India: Central TB Division, July 2020
Kindly provide your valuable feedback on the page to the link provided HERE
NAAT Labs and their role
ContentThe National Tuberculosis (TB) Elimination Program (NTEP) has a network of Nucleic Acid Amplification Tests (NAAT) laboratories coupled with Designated Microscopy Centers (DMCs) to form the backbone of the diagnostic component of TB services.
Nucleic Acid Amplification Tests (NAAT) laboratories includes Cartridge-based NAAT (CBNAAT) and TrueNat tests. These tests detect tuberculosis as well as rifampicin resistance and are more sensitive than smear microscopy.
Functions of Nucleic Acid Amplification Test (NAAT) Laboratories:
- Acting as a hub for collection of samples from public and private health facilities (spokes)
- Universal Drug Susceptibility Testing (UDST) to rule out rifampicin resistance among confirmed TB patients
- Timely provision of NAAT test result to the TB patient, medical officer of the concerned health facility and NTEP staff for related actions
- Acting as a sample dispatch center for the Culture DST laboratory for subsequent processing of samples for first-line line probe assay (LPA) and second-line drug resistance testing utilizing second line LPA and liquid culture DST
- Recording and reporting including digitization of diagnostic process from collection to test result in NTEP Nikshay portal and Laboratory Information Management System
- Management of supplies and logistic associated with laboratory logistic (CBNAAT cartridges and TrueNAT chips) and reporting any additional requirement thereof
- Supporting the quality assurance activities undertaken by District or Intermediate Reference Laboratory under NTEP
- Support health system in carrying out special drives for vulnerable and at-risk population and their testing directly by CBNAAT (slum population, diabetic population, smoker, malnourished people, patients of silicosis and kidney dialysis etc.)
Resources
- RNTCP Technical and Operational Guidelines for TB Control in India, 2016.
- Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Functions of a Designated Microscopy Centres [DMC]
ContentFunctions and Integrated Services of the DMC
- Testing of Sputum samples by Microscopy.
- Request/ referral for microscopy or Nucleic Acid Amplification Test (NAAT) or Culture and Drug Susceptibility Test (C&DST) or Chest X-ray (CXR) or Tuberculin Skin Test (TST) is generated at the PHI-DMC, as well as follow-up tests.
- Maintain consumables and logistics required for testing/ packaging and transport.
- Maintain TB laboratory registers for recording and reporting.
- Notify every TB patient in Nikshay at the earliest and update information of patients on comorbidity, treatment adherence, treatment outcome, contact investigation and TB Preventive Treatment (TPT).
- Biomedical waste management for the waste generated at DMCs.
- A DMC is required to participate in the External Quality Assurance system(EQA) of NTEP to ensure standardized quality diagnostic testing.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Sputum Collection centres
ContentTo increase access to diagnostic services, NTEP has a provision for sputum collection centres in areas where the health facility is not equipped with key requirements to conduct sputum microscopy, molecular tests, drug susceptibility testing or follow up examinations.
Sputum collection centres are dedicated locations where sputum samples are collected, packaged and then transported to nearby TB diagnostic centres. It could be attached to any near-by health-facility as well.
Requirements of a Sputum Collection Centre
To function as sputum collection centres, the following is essential:
- Linkage/ mapping (time and distance) to testing laboratory
- Availability of adequate number of sputum cups and falcon tubes, logistics for sample packaging and transport
- Identification of open areas for sputum collection
- Staff trained in NTEP guidelines on sputum collection, sample packaging and transport, complete and correct documentation of laboratory request form, and infection control practices
- Feasibility and financial measures required for sample transport
- Inclusion of local volunteers, courier services, sample transportation under National Health Mission Free Diagnostic Services or other mechanisms as decided by the state/district
- Availability of Information, Education and Communication (IEC) material, training modules, and job-aids
Sputum collection centres are established in:
- Ayushman Bharat Health and Wellness Centres/Sub-centres
- Urban primary health centres
- Tribal, hilly, desert and difficult-to-reach areas of the country
Resources
- Training Modules for Programme Managers and Medical Officers
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres
- Mycobacteriology Laboratory Manual, GLI Initiative, 2014
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under NTEP, where are sputum collection centres established to increase access to diagnostic services? Tribal areas Ayushman Bharat health and wellness centres Difficult-to-reach areas All of the above 4 To increase access to diagnostic services, sputum collection centres are established in Ayushman Bharat health and wellness centres, Urban health centres, tribal, hilly, desert and difficult-to-reach areas of the country. Yes Yes
-
STLS: Approaches to TB Case Finding
FullscreenScreening For Tuberculosis Disease
ContentScreening for active tuberculosis (TB) a process to filter out people who are less likely to have TB, from a group. Screened positive people are likely to have TB and are confirmed subsequently using a TB diagnostic test. This will allow finite diagnostic testing resources to be used on the remaining.
Screening in TB may be performed using simple field tools (4 Symptom complex) and tests such as Chest X-ray, or a combination of both. Combination of both is the most effective, but is often not applied due to the practical difficulties in making a chest X-ray conveniently available.
Screening is an integral part of any general case finding effort. It is also applied systematically in specific situations.
- At health care facilities (intensified case finding): Here those visiting are screened using the 4 symptom complex, often at the point of entry to the facility. Those screened positive may be fast-tracked to TB Diagnostic testing.
- In vulnerable populations in active case finding efforts: Here the entire population identified for active case finding are screened using the pre-decided protocols by going door to door.
Resources
Approaches to TB Case Finding
ContentPeople who have been exposed to patients with infectious TB are known as TB contacts; they constitute a high-risk group for TB. Case finding investigation contributes to the early detection of TB cases, and results in identifying a significant number of additional patients.
Figure: Approaches to Tuberculosis Case Finding
Active case-finding requires systematic screening and clinical evaluation of populations who are at high risk of developing TB, such as people living in slums, tribal areas, congregate settings, persons who are household contacts of TB cases
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Active Case Finding
ContentSystematic screening of all individuals of a defined population is known as active case finding. It is applied outside of health facilities at the community level by the health system.
Objective of ACF is to:
- identify cases early, initiate prompt treatment, reduce risk of poor treatment outcomes and reduce risk of further transmission of TB
- to provide access to diagnosis services to populations that would have been otherwise unreached
It is effort intensive and is recommended only in population groups where there is estimated high case load. In NTEP, ACF is recommended only to be performed in Key / vulnerable population.
ACF can also be clubbed with suitable ACSM campaigns to create awareness about the signs and symptoms and about TB in the target population/ community. It can also be combined with other health activities/ campaigns (such as Pulse Polio/ Leprosy screening/ population based screening for NCDs) for increased efficiency.
Resources
- Training Modules for Programme Managers and Medical Officers.
- Active TB Case Finding, Guidance Document.
- WHO recommendations for Systematic Screening for Active Tuberculosis
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is not a primary objective of ACF? Increase TB notification Early identification of cases. Reduce the risk of transmission of TB. Reduce the risk of poor treatment outcomes. 1 Notification is not a primary objective of ACF. Yes Yes Passive Case Finding
ContentPassive case finding is essentially where the patient self reports to the health care provider with symptoms. This requires that affected individuals are aware of their symptoms, have access to health facilities, and are evaluated by health workers or volunteers who recognise the symptoms of TB and link those individuals for TB testing services.
This approach to case finding has the least effort and cost and is a minimum expectation. In a Peripheral Health Institution (PHI), it is estimated that about 2-3% of new adult outpatients are symptomatic that require referral for TB diagnosis (presumptive TB cases).
Passive case finding may miss TB patients if :
- The disease is mild/ transient.
- Access to healthcare is poor.
- Health providers do not have an adequate index of suspicion and are unable to reliably link respiratory symptoms to TB.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following can be considered a passive case finding? TB case finding for all patients attending an HIV clinic. TB case finding in all inmates of an elderly home. Patients attending a PHC with symptoms are referred for testing by the doctor. TB case finding among household contacts of a TB case. 3 All other examples except those attending PHC referred for TB testing are cases of active or intensified case finding effort. Yes Yes What may cause a passive case finding to miss cases? Healthcare providers fail to notify the case. Healthcare providers do not refer cases for TB testing. There are no health facilities in the area. Both 2 and 3 4 Healthcare providers failing to notify cases is missing notification and not related to passive case finding. Yes Yes Intensified Case Finding
ContentIntensified Case Finding (ICF) is a case finding approach between Active and Passive approaches. Here individuals coming in contact with the health system through any activity are screened actively for symptoms of TB and referred for testing.
This approach brings the benefit of active case finding approach by active screening for TB symptoms, but does limit the extensive effort required by restricting to only those people who has some or the other healthcare problem. This approach is considered for people attending a healthcare facility.
Some examples of ICF are screening for TB symptoms and referral for testing in:
- all cases attending an HIV clinic.
- among children with malnourishment who attend a nutrition clinic.
- all mothers attending the antenatal clinics
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is an example of an intensified case finding?
Systematic screening for TB of all contacts of TB cases. Screening all cases attending an OPD with respiratory symptoms for TB testing. Referring cases that report more than 2 weeks of cough from an OPD for TB testing. Screening all people belonging to a slum for TB symptoms. 2 Systematic screening of TB contacts and those belonging to a slum population are examples of active case finding.
Referring to cases that report TB symptoms is a passive case finding.
Yes Yes Bidirectional Screening
ContentBidirectional screening is a method to identify cases in diseases which have predisposition to each other or has a significant influence on each other. For example TB and HIV, where having HIV increases risk of developing TB and cases with TB would have poor outcomes if co-infected with HIV.
Screening for TB is done through four-symptoms complex based screening or through Chest X-ray. Screening for the linked disease is carried out as per the policies of the corresponding health program.
Bi-directional screening policies are implemented by various disease control programs. For example, with NTEP the following disease control efforts implement a bidirectional screening policy:
- HIV through NACO
- COVID19
- Diabetes Mellitus (DM) through NPCDCS
- Tobacco through National Tobacco Control Program
Both programs monitor bidirectional screening, referral and testing as per their own policies.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Bidirectional screening for TB is not done in which of the following conditions? Diabetes Tobacco abuse/ addiction Pregnancy COVID-19 3 Although pregnant mothers may be screened for TB as a part of intensified case finding, all TB cases are not actively/ routinely screened for pregnancy. Yes Yes TB-HIV Bidirectional Screening
TB-Diabetes Bidirectional Screening
TB-Tobacco Bidirectional Screening
ContentWhy important, how is it done,
TB-COVID Bidirectional Screening
-
STLS: TB Case Finding in NTEP
FullscreenDiagnostic Algorithm for EPTB
ContentIt is crucial to make an effort for microbiological confirmation in presumptive Extrapulmonary Tuberculosis (EPTB) cases. Appropriate specimens from the Extrapulmonary (EP) site are collected and, depending on the specimen type and availability of facilities, the specimens are sent for:
- Cartridge-based Nucleic Acid Amplification Testing (CBNAAT)
- Culture and Drug Susceptibility Testing (C&DST) for M. tuberculosis
- Histopathological examination
The diagnostic algorithm (see the figure below) to be followed for EPTB cases depends on 2 main factors:
- Availability of appropriate specimens from the EP site
- Availability of CBNAAT (preferred test)

Figure: Diagnostic Algorithm of EPTB
- If an appropriate specimen from the EP site is available, specimens from the presumed sites of involvement must be tested with CBNAAT.
- CBNAAT detects MTB and RIF status and helps to identify microbiologically confirmed EPTB cases.
- If CBNAAT is not available, the specimen is sent for Liquid Culture (LC) at the C&DST lab. If the LC is positive, it is identified as a microbiologically confirmed EPTB case.
- If there is high clinical suspicion of TB even after a negative culture result, other diagnostic tools are used to clinically diagnose EPTB (usually with a specialist). If these tests indicate TB, they may be treated as clinically diagnosed EPTB or else arrive at an alternate diagnosis.
Clinical Diagnosis of EP-TB
If an appropriate specimen from the EP site is not available, in the presence of high clinical suspicion of TB, other modalities of diagnosis are used in consultation with a specialist. If with other diagnostic modalities, TB diagnosis still cannot be established, the specialist may explore an alternate diagnosis.
A clinical diagnosis of EPTB is made if a consultative decision is made to treat with a full course of anti-TB drugs in spite of the situations listed above. Chest X-ray (CXR), ultrasonography, Computerised Tomography (CT) scan, Magnetic Resonance Imaging (MRI) and biochemical examinations are supporting tests that can be used to help arrive at a diagnosis.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Technical Operational Guidelines, Chapter 3: Case Finding and Diagnosis Strategy, NTEP.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements are correct?
We must try our utmost best to get a microbiological confirmation in presumptive extrapulmonary tuberculosis cases.
If the extrapulmonary specimen is not available, then consult with a clinician if there is a high suspicion of TB to diagnose the case.
Wherever possible, all extrapulmonary specimens must be subjected to CBNAAT.
All of the above
4
Microbiological confirmation is crucial for EPTB cases, and CBNAAT is the preferred test. If specimens are not available, but TB is highly suspected, then a clinical diagnosis can be sought in consultation with a specialist.
Yes Yes Screening and diagnosis for DRTB
ContentDrug-resistant TB (DR-TB) diagnosis is predominantly based on laboratory diagnosis. Presumptive-TB/ DR-TB is identified by the health facility doctor during passive screening or by health staff/ community volunteers during Active Case Finding (ACF).
The vision of National TB Elimination Programme (NTEP) is to provide early diagnosis to all persons with any form of DR-TB through Universal Drug Susceptibility Testing (UDST).
All diagnosed TB patients are eligible for a NAAT test to know their Rifampicin sensitivity status. The integrated diagnostic algorithm for diagnosis of TB offers upfront Nucliec Acid Amplification Test (NAAT) for diagnosis of TB to vulnerable population. Among other eligible groups for NAAT are: non-responders to treatment and contacts of DR-TB patients are also offered upfront NAAT.
Rapid identification of DR-TB is achieved by using a combination of NAAT (CBNAAT/ Truenat) followed by sequential testing by first- and second-line Line Probe Assay (LPA) and Liquid Culture (LC) and Drug Susceptibility Testing (DST) for specific drugs as described below:
- When Rifampicin resistance is not detected by NAAT, the patient is offered First-line (FL) LPA.FL-LPA provides information on Isoniazid resistance.
- For Rif resistance/Inh resistance cases, SL-LPA is done and it provides information on resistance to Levofloxacin, Moxifloxacin and Amikacin.
- For all Rif resistance cases, LC and DST is done for Pyrazinamid, Moxifloxacin (if resistance detected by LPA), Linezolid, Clofazimine*, Bedaquiline* and Delamanid*.
(* when available)
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Liquid Culture and DST is done before NAAT. True False 2 Rapid identification of DR-TB is achieved by using a combination of NAAT (CBNAAT/ Truenat) followed by sequential testing by first- and second-line LPA and then liquid culture and DST. Yes Yes Integrated DR-TB Algorithm
ContentCheck
Diagnostic Algorithm for Paediatric DR-TB
ContentAll childhood TB patients’ sputum and other relevant samples (e.g. gastric aspirate, induced sputum, bronchoscopic lavage, lymph node aspiration, CSF, tissue biopsies etc.) should be subjected to genotypic or the phenotypic Drug Susceptibility Tests (DSTs). Based on the bacteriological confirmation, the child should be treated for DS/DR TB as required.
But in cases where the child’s DST is unknown, the source patient’s DST should be considered.
If the source is a known DS TB, treat the child for DS TB. If the child responds poorly to the DS TB treatment consult the pediatrician and re attempt the necessary investigations.
If the source patient is a known DR TB patient, consult with the pediatrician and re-attempt DST on an appropriate specimen from the child and treat as per the child’s DST (if the report is conclusive), if not then treat the child as DR TB after the source patient.
If the source patient’s DST status is not known perform DST on the child’s and the source patient’s specimen and treat the child as per the DST of the child or the source patient, whichever report is conclusive.
Pediatric TB patients should be presented to and discussed with a DR-TBC Committee (including the pediatrician) to decide the treatment.
Image
Figure: Diagnostic Algorithm for Paediatric DR-TB; Source: Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India,2021, CTD, MoHFW, India, p39.
Abbr: DR-TB: Drug-resistant TB; DS-TB: Drug-sensitive TB; NAAT: Nucleic Acid Amplification Test; MGIT: Mycobacterium Growth Indicator Tube; DST: Drug Susceptibility Testing; DRT: Drug Resistance Testing; BAL: Bronchoalveolar Lavage.
Resources
- Guidelines on Programmatic Management of Drug Resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Whose DST report should be considered if the child's DST is not known? Source Patient's DST Any other patient's DST No other patient's DST None of the Above 1 If the child's DST is not known, source patient's DST should be considered. Yes Yes Classification of TB on the basis of Site of disease
ContentBased on the site of disease, Tuberculosis can be classified as-
- Pulmonary tuberculosis (PTB) refers to any microbiologically confirmed or clinically diagnosed TB involving the lung parenchyma or the tracheo-bronchial tree.
- Extra Pulmonary tuberculosis (EPTB) refers to any microbiologically confirmed or clinically diagnosed TB involving organs other than the lungs such as pleura, lymph nodes, intestine, genitourinary tract, joint and bones, meninges of the brain etc.
Note: Miliary TB is classified as PTB because there are lesions in the lungs. A patient with both pulmonary and extra-pulmonary TB should be classied as a case of Pulmonary TB.
Classification of TB cases based on history of Previous TB treatment
Content- New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
- Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated(cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
- Transferred In: A TB patient who is received for treatment in a Tuberculosis Unit, after registered for treatment in another TB unit is considered as a case of transfer in.
- Transferred Out : A patient who has been transferred to another recording and reporting unit and whose treatment outcome is unknown.
Classification of TB on the basis of Drug Resistance
ContentResistant Sensitive Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistant to Isoniazid (H) Rifampicin (R) Fluroquinolones (FQ) =
Ofloxacin, Levofloxacin,
MoxifloxacinGroup A Drugs =
Bedaquiline/ LinezolidH Mono / Poly Drug Resistance Resistant Sensitive Unknown/ Sensitive Unknown/ Sensitive Rifampicin Resistance (RR) Unknown/ Sensitive Resistant Unknown/ Sensitive Unknown/ Sensitive Multi Drug Resistance TB (MDR TB Resistant Resistant Unknown/ Sensitive Unknown/ Sensitive Pre-Extensive Drug Resistance (Pre -XDR) Resistant Resistant Resistant Unknown/ Sensitive Extensive Drug Resistance (XDR) Resistant
Resistant Resistant Resistant Resources:
Classification of TB on the basis of diagnosis
ContentOn the basis of diagnosis, Tuberculosis (TB) can be classified into 2 main types:
- Microbiologically confirmed TB
- Clinically diagnosed TB
Microbiologically Confirmed TB
- Microbiologically confirmed TB refers to a presumptive TB case from which a biological specimen is positive for acid-fast bacilli/ Mycobacterium tuberculosis on smear microscopy, culture, or on a rapid diagnostic molecular test (such as Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ Truenat).
- All such diagnosed cases should be notified at the source, regardless of whether TB treatment has started.
Clinically Diagnosed TB
- Clinically diagnosed TB refers to a presumptive TB case that is not microbiologically confirmed but has been diagnosed with active TB by a clinician who has decided to give the patient a full course of anti-TB treatment.
- This definition includes cases diagnosed on the basis of X-ray abnormalities or suggestive histology or extrapulmonary cases without laboratory confirmation.
- Clinically diagnosed cases subsequently found to be microbiologically positive (before or after starting treatment) should be reclassified as microbiologically confirmed.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Definitions and Reporting Framework for Tuberculosis, WHO, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TB is classified on the basis of diagnosis into which of the following? Microbiologically confirmed TB and clinically diagnosed TB Mono-resistant TB and poly-resistant TB Recurrent cases and previously treated cases None of the above 1 TB can be classified on the basis of diagnosis into 2 main types: Microbiologically confirmed TB and Clinically diagnosed TB. ACF campaign activities
ContentActive Case Finding (ACF) is a provider-initiated activity with the primary objective of detecting TB cases early by active case finding in targeted groups and to initiate treatment promptly.
- It can target people who anyway would have sought health care with or without symptoms or signs of TB and also people who do not seek care.
- Increased coverage can be achieved by focusing on clinically, socially and occupationally vulnerable populations.
- ACF activities in a campaign mode will create mass awareness about the signs and symptoms in general population
Objective of ACF campaign activities- Reaching the unreached in a campaign mode to enhance TB case finding

Figure 1: Objectives of active case finding
Beyond TB disease, screening can also identify individuals who are eligible for and would benefit from TB preventive treatment (TPT) once TB disease is ruled out, thus further averting future incident TB.
General process is as below:

Figure 2: ACF campaign general process
Resources
- WHO consolidated guidelines on tuberculosis: Module 2: Screening, Systematic screening for TB disease;WHO 2021
- India TB Report 2022, Central TB Division, MoHFW 2022
- Active TB Case Finding- Guidance document, Central TB Division & DGHS, MoHFW 2017
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF will help in reducing spread of tuberculosis True False 1 ACF helps in early case detection & treatment initiation, thus reducing community level prevalence of TB disease & limit spread
Mapping the population for ACF
ContentMapping of vulnerable population is a pre-requisite for conducting an efficient ACF campaign. It involves understanding the population characteristics, identifying and enumerating and mapping the target population.
Guidelines for mapping
- Identify & map high risk/ vulnerable populations in the local area with the following guidance. If additional information is available locally, it can be used for the prioritisation of target groups.
Priority Urban area Rural area Tribal area
1 Slum Difficult to reach villages Difficult to reach villages & hamlets 2 Prisons inmates Mineworkers Villages with a known higher caseload 3 Old Age homes Stone crusher workers Tribal school hostels 4 Construction site workers Populations groups with known high malnutrition Areas with known high malnutrition 5 Refugee camps Populations known to drink raw milk Villages seeking care from traditional healers 6 Night shelters Populations known to eat uncooked meat Populations known to drink raw milk 7 NACO/SACS identified HRG for HIV NACO/ SACS identified HRG for HIV Populations known to eat uncooked meat 8 Homeless Weaving & Glass industrial workers Tribal areas with little ventilated huts 9 Street children Cotton mill workers 10 Orphanages Unorganised labour 11 Homes for destitute Tea garden workers 12 Asylums Villages largely seeking care from traditional healers 
Figure 1: Schematic map for house to house survey of identified vulnerable population
- Without proper mapping, there is a high chance of missing cases. The success of the active TB case finding campaign relies on how good the mapping is.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF campaign activities are done in all individuals of a defined area. True False 2 Symptom screening as part of the ACF campaign will be done in the identified and mapped target groups only (not in the general population).
Yes Yes Planning for ACF
ContentActive case-finding (ACF) approaches bring essential TB services closer to the community. It has high potential for improving TB case detection and reach people with TB currently missed by the health system. To maximize gains from ACF, it is important that the interventions are planned in advance.
Planning for ACF includes identifying the right target population/area, designing the intervention, finding the right implementing partners, training of workforce, microplanning for daily activities, logistics, ensuring that the complete pathway of care is followed, reporting and recording.
Steps involved in planning for ACF
1. Identification of population based on:
a. increased risk for TB eg: prisoners, miners, urban slums, co-morbidities like HIV, diabetes etc.
b. those with limited access to health services eg: migrants, homeless, tribal, live in hard to reach areas etc.
2. Identification of stakeholders including district and sub-district TB program staff, non-government organizations, community based organizations, community health workers to support with ACF activities
3. Strengthening the health system e.g. training of staff, ensuring sufficient lab supply and lab technicians. Staff trainings should be done to eliminate gaps in knowledge about TB, cough hygiene, infection control measures, conducting screening, collecting quality sputum, transporting sputum or referring people with presumptive TB to the health facility/laboratory, TB testing, data collection, data entry
4. Microplanning for ACF includes:
a. when and where to conduct ACF-day, time, duration, methodology-camp, door-to-door, community gatherings, home visits, place of work etc
b. availability of trained manpower, team composition, logistics and consumables
c. screening and diagnostic algorithm to be used
d. number of screenings and tests done per day
e. accessibility and linkage with TB testing laboratories, use of mobile van with CXR, CBNAAT/Truenat
f. laboratory workload to accommodate additional testing due to ACF
g. laboratory turn around time, availability of test reports for clinical management
h. advocacy on ACF activities with the target population, pre-sensitization meetings, addressing perceived risks of TB screening and diagnosis (e.g. job loss, loss of income)
i. data collection tools (paper based, smartphones, tablets etc.), TB notification, recording and reporting
Resources
1. Systematic screening for active tuberculosis: an operational guide (http://www.who.int/tb/publications/ systematic_screening/en/)
2. Experience of active tuberculosis case finding in nearly 5 million households in India (Prasad BM, Satyanarayana S, Chadha SS, Das A, Thapa B, Mohanty S, et al. Public Health Action. 2016;6(1):15–8. doi:10.5588/pha/15/0035)
3. Community-wide screening for tuberculosis in a high-prevalence setting (Marks GB, Nguyen NV, Nguyen PTB, et al. N Engl J Med 2019; 381: 1347-57)
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
True or False: Active case screening required planning for manpower, resources and microplanning for ACF activities
True
False
1
Active case screening required planning for manpower, resources and microplanning for ACF activities
Training the workforce for ACF campaign
ContentA state-level meeting by the Principal Secretary of Health & Family Welfare with all members must be held to communicate the days of the Active Case Finding (ACF) campaign and take all the necessary actions needed to conduct a successful campaign in the state.
Training for ACF is given in a top to bottom manner as follows:
I. State-level training workshop
- One-day training workshop for District and Sub-district level officers will be conducted.
- Trainers - State TB Officers (STOs), State TB Training and Demontration Centre (STDC) in charge, National TB Elimination Programme (NETP) Consultants, Central representatives
- Trainees - District TB Officers (DTOs), Block/ Municipal Medical Officers, Senior Treatment Supervisor (STS), Senior Treatment Laboratory Supervisor (STLS), Non-government Organisation (NGO) partners, etc.
- The objective of the workshop should be to sensitise the district & block level planners on the strategy to be followed, the need for preparing micro-plans for their areas, and sort out issues of coordination between the implementing partners.
- Training to suspect the TB cases in the community, collection/ transport of sputum samples and recording/ reporting of daily activities should also be given.
II. District micro-planning meeting/ Urban area planning meeting
- The Chief Medical Officers (CMO) / DTOs/ National TB Elimination Programme (NTEP) consultants and the NTEP field staff, should facilitate these meetings.
- The meetings have to be attended by all block/ municipal medical officers, and other organisations involved in social mobilisation, along with personnel involved in planning at the block level.
- The objective of these meetings should be to sensitise the Block Medical Officers (BMOs) on how to micro-plan for their areas for the upcoming ACF campaign. Special attention should be paid to developing area-specific Information, Education and Communication (IEC) strategies for difficult areas.
III. Orientation trainings at block/ ward level for Accredited Social Health Activists (ASHAs)/ Field Level Workers (FLWs)/ NGO staff
- Trainers - DTOs, block/ municipal medical officers and NTEP consultants (wherever available)
- Trainees - ASHAs and local volunteers. Concerned supervisors of the team must also present during these orientation trainings.
- The objective of the trainings would be to build the capacity of all the field level workers (ASHA & FLW) to suspect TB cases in the community, collect/ transport sputum samples and record/ report daily activities.
- The orientation will cover the operational as well as the Interpersonal Communication (IPC) aspects of the ACF campaign.
- The instruction sheet for the search team, recording/ reporting tools, sputum collection & transportation methodologies, and Frequently Asked Questions (FAQs) should be distributed and discussed during this orientation.
- Demonstration of recording/ reporting tools and house markings followed by exercises for ensuring all operational skills as also role plays on IPC and FAQs should form an essential component of all FLW/ ASHA training sessions.
References
AssessmentAnswer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Training for the ACF campaign is held only at the district level.
True
False
False
Training for ACF is held at all levels – state, district, block and ward levels.
Yes
Yes
- One-day training workshop for District and Sub-district level officers will be conducted.
Contextualizing the algorithm for ACF campaign
ContentA good screening algorithm should have the following characteristics:
- High specificity (to reduce the number of false positives, ideally around 70%)
- High sensitivity (to reduce the number of false negatives, ideally around 90%)
- Low Number Needed to Screen (NNS)
- Low cost
- Rapid and simple to apply
- High client acceptability
The algorithm should be optimised so that the maximum number of cases can be detected with available resources.
Usually verbal screening using symptom complex (4S) are used. However ACF campaigns targeting high risk populations (household contacts, elderly homes etc.)can consider using X ray also as a screening tool. Chest X ray helps in picking up sub-clinical TB cases also which will be usually missed through verbal screening of symptoms.
A more sensitive test like NAAT is preferred over sputum microscopy in ACF campaigns as the cases will be in early stage and may be missed by testing using Microscopy.
References
- Optimising Active Case Finding – Implementation Lessons from South-East Asia. WHO SEAR, 2021.
- WHO Consolidated Guidelines on Tuberculosis – Module 2: Screening, WHO, 2021.
- High-priority Target Product Profiles for New Tuberculosis Diagnostics: Report of a Consensus Meeting, 28–29 April 2014, Geneva, Switzerland. Geneva: World Health Organisation, 2014.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Page ID Part of Pre-test
Part of Post-test
Which of these is a condition for a good screening algorithm for ACF? Minimise false positive results Ensure that the maximum number of cases are diagnosed with available resources The algorithm may differ from place to place depending on the local TB burden among different subgroups All the Above 4 A good screening algorithm is one which ensures a high yield of cases, with minimum resources and ensures equitable access to TB care. This algorithm has to be optimised locally based on research and previous prevalence data among subgroups. 2008 Yes Yes Identifying the resources for ACF campaign
Content1. Financial Resources
- Financial resources for ACF may be procured from the Centre/State or through local Private Provider Support Agencies (PPSA). When the funds for ACF are procured from the centre, it should be included under a separate budget head (DSTB Pool) under PIP.
- Each team would be eligible for an incentive of INR 500 for every new case of TB diagnosed and put on treatment under this activity OR as per approvals in the Programme Implementation Plan (PIP) in the National Programme Coordination Committee (NPCC) of the respective state or as approved by the state National Health Mission (NHM).
- Each state should ensure that local travel arrangements from the general health system are made available for the field visits by the team, supervisory visits, etc.
- Allowances to ensure Travel Allowance (TA)/ Dearness Allowance (DA) and refreshments as per entitlement are to be made from the respective source of salary for the field teams and supervisory teams.
2. Consumables
Logistics for an ACF campaign include:
a. IEC materials: Appropriate IEC materials are to be designed and printed in the local language. A prototype of the same will be shared with states from the CTD. IEC material printing/ distribution should be completed by two weeks before the start of field activities.
b. Additional logistics for testing:
- Additional slides, laboratory reagents, sample transport boxes, X-ray films, CBNAAT cartridges, falcon tubes (minimum 1000 per 1 lakh population) should be procured and supplied to health staff for collecting sputum samples from the eligible symptomatic at least two weeks before the start of field activities. Boxes for sputum sample transport should be provided to the health staff for carrying samples to DMCs.
- Additional sputum examination request forms needed – 500 per 1 lakh population
c. Recording and reporting forms: All recording and reporting formats requirement assessment is to be done by DTOs three weeks before the start of field activities
3. Human resource
Human resource for ACF is required for the following:
a. Field activities: House-to-house visits, symptom screening, sputum collection and transport to the Designated Microscopy Centre (DMC).
- One field visit team will comprise two members - one health worker from National TB Elimination Programme (Senior Treatment Supervisor (STS)/ Senior TB Lab Supervisor (STLS)/ TB Health Volunteer (TB-HV)) or a partner organisation (NGO outreach worker) or general health services (Auxiliary Nurse Midwife (ANM)/ Multipurpose Worker (MPW)/ Multipurpose Healthcare Supporters (MPHS) and one Accredited Social Health Activist (ASHA) or community volunteer. The states should decide on the team composition based on available resources and the population to be covered (as obtained from vulnerability mapping).
- House-to-house visits by health workers should involve community leaders, panchayat members particularly the women members, religious leaders and other local influencers like medical practitioners, local moneylenders, grocery shop owners, popular teachers, prominent youth, etc.
- Local community members/ influencers must accompany search teams during house-to-house visits in such areas, especially during revisit to houses.
b. Testing additional sputum samples for Mycobacterium tuberculosis (MTB): Laboratory technicians of the linked DMC and Cartridge-based Nucleic Acid Amplification Test (CBNAAT) labs should be well-informed about the increase in workload and recording of information during ACF activities.
c. Supervision and Monitoring of ACF activities: Supervision and monitoring of the campaign are done at various levels under the leadership of designated officers. It is required during the preparatory phase as well as the implementation phase of the campaign.The list of observers along with the districts/ blocks/ urban areas allotted must be shared with Central TB Division (CTD).
- Village level - Medical Officer of Primary Health Centre (PHC)/ Community Health Centre (CHC)/ Urban Health Centre (UHC)
- Block level - Block Medical Officer (BMO)/ Block Health Officer (BHO)
- District level - District TB Officer (DTO)
- State level - State TB Officer (STO)
- Regional level – Regional Directors of the Regional Office of Health and Family Welfare (ROH&FW) will be in charge of supervising activities in their respective states.
- National level - One national level officer for each state will be nominated by CTD to supervise and monitor activities including field visits to the states prior to and during the campaign.
References
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements is true about ACF ? ACF campaign is done once in 3 years.
ACF campaign doesn’t require additional manpower or logistics Each field team should screen a minimum of 100 targeted populations in 2-3 days. Each field team should have a community volunteer or ASHA worker. 4 1. ACF campaign should be done 3 times a year.
2. It requires additional manpower, logistics and financial resources
3. 500 persons to be screened in 2-3 days by each team.
Yes Yes Microplanning and execution of ACF campaign
ContentMicroplanning for ACF Campaign
A microplan is a detailed plan of action in terms of human resources, materials, money and time. A good microplan ensures that the health intervention reaches each individual beneficiary and is crucial to the success of the activity. For Active Case Finding (ACF), microplanning is performed at the health facility level and collated at the block, district and state levels. Training for the same is given to concerned personnel during state, district and block level meetings prior to the campaign. Microplan at PHI, Block, District and State levels should be ready at least 15 days prior to the initiation of field activities.
Microplanning is done with respect to:
I. Advocacy, Communication and Social Mobilization (ACSM)
A comprehensive IEC plan should be made with communication material for mass media, mid-media and print media to reach out up to the remotest village in advance.
II. Logistics
- Microplan should include planning additional consumables required for the campaign
- It includes additional slides, laboratory reagents, sputum cups, falcon tubes, sample transport boxes, X-ray films, Cartridge-based Nucleic Acid Amplification Test (CBNAAT) cartridges, etc. Additional sputum containers (minimum 1000 per lakh population) will be procured and supplied to health staff for collecting sputum sample from the eligible symptomatic two weeks before the start of field activities
- Linkages of Peripheral Health Institute (PHI) areas with Designated Microscopy Centre (DMC), X-ray facilities, CBNAAT lab, Extra Pulmonary (EP) sample collection and EP testing should be included in the planning up-front.
- Laboratory technicians of the linked DMC and CBNAAT labs should be well informed about the increase in workload and recording of information during ACF activities.
III. Field activities including human resources
- Maps prepared for other campaigns like Pulse Polio, Leprosy Case Detection Campaign (LCDC), etc. must be used while planning. If maps are not available with local bodies, search team members and supervisors should be sent to the area before the ACF campaign, in order to become familiar with the area and develop maps.
- The number of houses to be covered each day should be mentioned in the microplan. This number may vary from day to day depending upon the geographical situation of the area planned to be covered by the team on a particular day.
- Teams of two persons each should go house-to-house. Out of the two members in each team, one should be a local volunteer (including Accredited Social Health Activist (ASHA)).
- Each team should be allocated clear-cut, well-demarcated areas clearly mentioning the starting and ending points, identifiable with landmarks; for each day of House to House (h-t-h) activity.
- In special areas, one additional person from the local community, where the team will be working, should accompany the team.
- Human resources required for covering the mapped vulnerable population during field activities should be calculated and recorded.
- For planning and implementation purposes, urban areas should be divided into smaller planning units based on municipal wards or assemblies, or by roads or prominent landmarks. Each such unit should be put under the charge of a medical officer or nodal officer.
- Involvement of the local community, leaders, health officials, municipal bodies and their staff is essential in planning.
- Local staff is familiar with the layout of the urban areas and their inputs are vital for planning and supervision of house-to-house activities.
Execution of Microplan
The ACF campaign is executed as per the microplan and supervision is done with reference to the microplan
The House to House (h-t-h) survey is done for 2 weeks
A survey team consisting of 2 persons - one NTEP staff/ partner organization staff/ General Health services staff and one local volunteer / ASHA worker. They go from house to house in the mapped vulnerable areas/ key population groups and screen individuals for symptoms of TB. After screening, the eligible population for sputum examination includes: Persistent cough for ≥2 weeks, Fever for ≥2 weeks, Significant weight loss (>5% weight loss over last 3 months), Presence of blood in sputum any time during the last 6 months, Chest pain in the last one month, History of Anti-TB Treatment (previous/ current). If any one of these is present, a sputum cup or falcon tube is given to them and a sputum sample is collected. Sputum samples thus collected are transported to a designated lab using the sample transport system existing in the area. testing using smear microscopy/CBNAAT will be done for all symptomatic persons as per the state policy. Those who are microbiologically confirmed to be positive should be initiated on treatment within 2 days. Additionally, the team will look for other symptoms/diseases also. If person is having any symptoms or other ill health, s/he will be referred for evaluation by a Medical Officer for further management, if needed. Field Activity Report will be submitted by each health staff on a daily basis to the Medical Officer of the Peripheral Health Institution
Resources
- Active TB Case Finding – Guidance Document, 2017, Central TB Division, MoHWF, New Delhi.
- Active Case Finding for Tuberculosis in India: A Syntheses of Activities and Outcomes Reported by the National Tuberculosis Elimination Programme, Burugina Nagaraja S et al, Trop Med Infect Dis., 2021.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is wrong about microplanning in ACF?
Microplan is first made at the state level. It is a detailed plan of the human resources, logistics and field activities required in the ACF campaign.
A good microplan is important for the success of the ACF campaign.
Supervision of field activities is done with reference to the microplan.
1
Microplan is made at the health facility level and then collated at subsequent levels.
Yes
Yes
Recording formats under ACF campaign
ContentVulnerability mapping and Microplanning are 2 important activities of Active Case Finding which precede field activities. Vulnerable populations should be mapped and recorded in prescribed formats from health facility level onwards. Mapping data from PHI are consolidated at Block level, those at Block level are consolidated at district level and those at district level are consolidated at state level. Data from mapping formats is used for microplanning. Microplanning forms the basis of field activities. Microplans are also consolidated at subsequent levels. During supervision and monitoring, it is important to assess the activities with respect to the microplan.
The recording formats for ACF include:
1. Formats for mapping - Health Facility Level, Block Level, District Level and State Level
2. Formats for microplanning - Manpower, Logistics, Field Activity
FORMATS FOR MAPPING





Mapping details should also be entered in Ni-kshay under the section shown below:
Image
Fig: Ni-kshay section for reporting various ACF activities
FORMATS FOR MICROPLANNING
Based on the requirement obtained from the mapping exercise, microplanning is done with respect to human resource, logistics and field activities
Human Resource Planning Form



Field activities are captured in Form 1 & 2 of the ACF. The data from field activities are compiled at the PHI level and submitted to the District and State using google sheets at present. Although there is no specific mechanism to demarcate the presumptive TB patients and the confirmed (clinical and microbiological) TB cases in Ni-kshay, States follow different mechanism including marking in the Laboratory register as ACF testing and sending a separate sheet to the district in paper format.
Reference:
1. Active TB Case Finding - Guidance Document, Central TB Division & DGHS, MoHFW, 2017
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Vulnerability mapping and microplans for ACF should be recorded at
Health facility level
District level
State level
All the above
4
Mapping activities should be recorded at health facility level and consolidated at subsequent levels (district, state, etc)
Yes
Yes
Field Supervision of ACF campaign
ContentField supervision of Active Case Finding (ACF) is needed during both the preparatory phase and the implementation phase. Supervisory teams should be formed at the National, State, District, Block and Peripheral Health Institute (PHI) levels.
Field supervision during the preparatory phase:
The Field Supervisors should:
- Attend District and Block Coordination Committee meetings.
- Review the micro plan and check whether all components are present.
- All geographical areas have been included.
- Team composition is appropriate – all house-to-house teams have at least one Accredited Social Health Activist (ASHA) and at least one Non-government Organisation (NGO) worker and at least one National TB Elimination Programme (NTEP) field staff.
- Sensitisation training to detect the cases has been planned for all ASHAs and field staff.
- Workload of teams in terms of houses to be covered/ day has been rationalised.
- Areas requiring special attention have been identified and plans developed.
- Information, Education and Communication (IEC)/ social mobilisation plans have been developed and documented.
- All geographical areas have been included.
Field supervision during the implementation phase:
- All officers should again visit their allotted districts/ blocks/ urban areas during the implementation phase to assess the quality as well as the completeness of coverage of the area through house-to-house visits.
- Field Activity Report will be submitted by each health staff on a daily basis to the Medical Officer of PHI. The Field Activity reports from all health staff will be analysed and appropriate action will be taken by the Medical Officer of PHI and these reports will be combined and a report will be prepared and submitted to Block Medical Officer (BMO) on daily basis.
- Ensure a mechanism of daily feedback from the observers to the block and district control rooms to facilitate immediate corrective action at all levels. Tracking the cascade of care is a useful tool for assessing quality. (Cascade of care: Track No. of people targeted, no. of people screened out of targeted, no. of presumptive TB identified out of screened, no. of presumptive TB patients examined out of identified, no. of presumptive TB completely evaluated {like smear-negative patients examined with chest X-ray and Cartridge-based Nucleic Acid Amplification Test (CBNAAT), no. of TB patients diagnosed out of examined, no. of TB patients put on treatment out of those diagnosed.})
- Qualitative and quantitative assessment of the ACF campaign activity from observers should be utilised for long-term corrective actions like problems faced by ASHAs & Frontline Workers (FLWs) during the campaign, review of micro-plans etc. or immediate corrective actions like repeating the activity in an area where a significant number of uncovered houses are found after completion of the activity.
The Progress indicators and quality indicators for ACF should be monitored by the supervisory team while on field visit.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What should be the minimum limit for the sputum positivity rate in ACF? 2-3% 10% 8% 15% 1 For the quality of samples collected, in health facilities in passive strategy, an average of 15% positivity is found, but in active case finding it would be as low as 5%, but should not be below 2-3% in any case, and can be monitored as a quality indicator for the campaign. Yes Yes Monitoring of ACF campaign
ContentMonitoring should be an integral part of the Active Case Finding (ACF) interventions. It is accomplished by a strong data collection system enacted through a programme-based ACF data and recording in Nikshay.
Monitoring activities for ACF interventions broadly cover the number screened, number of presumptive TB cases based on symptoms or chest X-ray findings, samples collected for testing, samples transported for testing, samples tested, microbiologically and clinically diagnosed TB cases, TB notification and treatment initiation.
Monitoring Against the ACF Plan
1. Monitor the Number Needed to Screen (NNS), i.e., the number needed to be screened based on current TB symptoms, past history of TB, comorbidities, other socio-economic factors, etc.
2. Monitor the Number Needed to Test (NNT) which helps understand the efficiency of diagnostic testing and the efficiency of screening for presumptive TB.
3. Monitor the yield of ACF activities, i.e., TB cases found and compare the yield of different screening and testing methods (X-ray, smear, Nucleic Acid Amplification Test (NAAT)).
4. Monitor whether there was an additional increase in TB notification of bacteriologically confirmed TB cases compared to the previous year (or in comparison to a control district).
- Monitor notification trends, treatment outcomes and mortality (TB prevalence should decrease over years based on repeated ACF in the same population).
5. Monitor engagement of National TB Elimination Programme (NTEP) staff, non-governmental organisations, community volunteers and the private sector in ACF activities.
Monitoring Against the Cascade of Care
1. Monitor the proportion of people with presumptive TB who provide sputum.
2. Monitor linkage to health facilities, sample collection, transportation and tests done.
3. Monitor drop-outs between screening and diagnosis, dropouts between diagnosis and treatment.
4. Monitor public health action provided to notified TB cases.
Resources
- Optimizing Active Case Finding for Tuberculosis, 2021.
- Training Module (1-4) for Programme Managers and Medical Officers, NTEP, MoHFW, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Monitoring of ACF intervention is accomplished by a strong data collection system enacted through program based ACF data and recording in Nikshay. True False 1 Monitoring of ACF intervention is accomplished by a strong data collection system enacted through program based ACF data and recording in Nikshay. Yes Yes Reporting of ACF campaign
ContentThe ACF campaign has to be reported for documentation, monitoring and evaluating the performance of the activity and guiding the policy decisions.
The various formats used for reporting of performance of Active Case Finding (ACF) activities are as follows:
1. Field activity daily report
- Submitted by each health staff on a daily basis to the Medical Officer of Primary Health Centre (PHC)/ Community Health Centre (CHC)/ Urban Health Centre (UHC).
Table 1: Format for field activity daily report
Name of citizen
Type of target population
Address/ Place
Age
Sex
Symptom (write no of days)
Sputum sample collected?
Sputum
TB diagnosed?
TB treatment initiated?
Any other symptoms (specify)
Refer to (where)
Cough
Fever Weight Haemoptysis Chest pain h/o ATT 1
2
3
4
2. ACF activity reporting by Health Facility
- The Field Activity reports from all health staff will be analysed and appropriate action will be taken by Medical Officer of PHC/ CHC/ UHC.
- These reports are combined and a report will be prepared as per the following format and submitted to Block Medical Officer (BMO)/ Block Health Officer (BHO) on daily basis.
Table 2: Format for ACF activity by health facility
State: …………………………… District: …………………………………. TB Unit:………………………… PHC/CHC/UHC:………………
Total Population of PHC/CHC/UHC:………………
Total mapped target population:…………………..
Type of target population
Address / place
Population of target group
Number screened for symptoms
Number examined for sputum
Number of TB patients diagnosed
1
2
3
4
At the block level reports from all the reporting units will be compiled in the below format and sent to the District on a daily basis.
3. ACF activity reporting by Block/ Town/ City
Table 3: Format for ACF activity reporting by block/ town/ city
State: …………………………… District: …………………………………. Block/Town/City:…………………………
Name of PHC/CHC/UHC
Total mapped target population
Number screened for symptoms
Number examined for sputum
Number of TB patients diagnosed
1
2
3
4
And at the district level, reports from all blocks are to be compiled in the format below, and the consolidated report should be sent to the State.
4. ACF activity reporting by District
Table 4: Format for ACF activity reporting by district
State: …………………………… District: ………………………………….
Name of Block/Town/City
Total mapped target population
Number screened for symptoms
Number examined for sputum
Number of TB patients diagnosed
1
2
3
4
5. ACF activity reporting by State
Table 5: Format for ACF activity reporting by state
State: ……………………………
Name of District
Total mapped target population
Number screened for symptoms
Number examined for sputum
Number of TB patients diagnosed
1
2
3
4
- State TB Officer (STO) would be responsible for the overall coordination and implementation of campaign activities and reporting in the State/ UT.
- Data entry of district-level reports in electronic format will be ensured by District TB Officer (DTO) on a daily basis after the field activity is completed. Nikshay has a section on active case finding where the mapping of target population and reporting of various activities can be done.

Fig 1: Nikshay section for reporting various ACF activities
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Who is in the overall charge of activities and reporting of ACF campaign in a state?
Health minister
Medical college task force
State TB Officer
None of the above
3
State TB Officer would be responsible for the overall coordination and implementation of campaign activities and reporting in the State/ UT.
Yes Yes
-
-
STLS : Smear Microscopy
Fullscreen-
STLS: Collection & Storage of Good Quality Specimen
FullscreenAccepting the request for testing
ContentThree things are received by the Lab Technician- Sample for testing, request form, and request for test in Nikshay.
Accepting the request for testing includes the following steps:
1. The LT verifies details on the request form that has eleven parts.
- The first part contains details on the name of referring facility, name of the patient, complete address, age & gender of the patient, date of referral, type of presumptive TB, the key population to which the patient belongs and site of disease.
- The second part contains details of referring facilities, Nikshay ID, and the names of State, district and TB units.
- The third portion is for the diagnosis and follow-up of TB.
- The fourth portion is for the diagnosis and follow-up of drug-resistant TB.
- The fifth portion is to indicate the required tests with the details of the person requesting the test.
- Parts six to eleven are used for reporting test results.
2. The LT verifies the quality of the sample received.
3. LT captures details on the patient, reasons for testing, test requested, and the visual appearance of the sample in the TB Laboratory register.
4. LT verifies the test request generated in Nikshay against the test ID requested (Figure).

Figure: Test Details Added in Nikshay by the Referring Health Facility; Source: Guidelines for PMDT in India, 2021.
5. LT initiates the test requested.
Resources
- Guidelines for PMDT in India, NTEP, 2021.
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
For all new presumptive TB cases, Nikshay ID is generated by the referring facility.
True
False
1
For all new presumptive TB cases, Nikshay ID is generated by the referring facility.
Yes
Yes
Spot and early morning sputum sample
ContentPresumptive pulmonary TB patients are subjected to sputum smear microscopy (Ziehl Neelsen (ZN)/ Florescence Microscopy (FM)). Two consecutive sputum specimens will identify the vast majority (95–98%) of smear-positive TB patients
Two specimens are collected:
- One Spot and one early morning sample OR
- Two supervised spot specimens collected at least one hour apart, and smears made from both the samples.
If one or both smears are positive, the patient is diagnosed as a microbiologically confirmed pulmonary TB case.
- The spot specimen collected is labelled as 'a'.
- While the patient is given a labelled container with instructions to cough out sputum into the container early in the morning after rinsing the mouth with water. This is the early morning specimen. This is labelled as specimen 'b'.
- If the health facility is not a Designated Microscopy Centre (DMC), then the patient is given a sputum container with the instructions to collect an early morning specimen and go with the sputum specimen to the DMC where the spot specimen can be collected.
- In case the patient is not able to travel to the DMC, then the spot specimen could be collected at the nearest health facility or sputum collection centre and transported to the DMC.
- These two samples should be collected within a day or two consecutive days.
- Two supervised spot samples may be collected one hour apart if patient is too sick, coming from a long distance or likelihood of not giving a second sample is significant.
- Collection of early morning specimens is preferred because of the overnight accumulation of secretions. However, spot samples collected at any time for patients is also suitable if productive sputum is expectorated after deep cough.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The spot specimen collected for sputum microscopy is labelled as 'a'.
True
False
1
The spot specimen collected for sputum microscopy is labelled as 'a'.
Yes
Yes
Educating patient on Sputum collection and dispensing Sputum cup
ContentEducating patients on collection is essential to have good quality sputum. The healthcare worker (HCW)/ medical officer (MO) or the laboratory technician (LT) can educate patients on how to collect and dispense sputum.
The HCW/MO/LT provides a new sputum cup with the Laboratory Serial Number written on its side to the patient. They should explain that sputum should be collected in an open place or in a well-ventilated room; it should not be collected in closed rooms, toilets and ill-ventilated rooms
A specimen collected under supervision is likely to yield better results. Supervising person has to demonstrate how to collect good sputum and dispensing it:
- Using a laboratory sputum cup, demonstrate how to open the lid of the specimen container and place it conveniently within their reach, so they can close it immediately after collecting sputum and also how to screw the cap on the cup tightly so it doesn't leak.
- Demonstrate how to bring up sputum, beginning with rinsing their mouth as food particles may give false positive results.
- Demonstrate deep inhalation (2–3 times) and let the patient know that this will initiate the cough reflex in most individuals.
- Demonstrate how individuals can place their palms on the waist, squat or sit and continue deep breathing again. Tapping or thumping of the back
may encourage expectoration (Sitting and placing hands on the waist fixes the shoulder and pelvic muscles and brings the intercostal muscles of ribcage and diaphragm into action) - After deep inhalation and coughing deeply, the sputum should come up in their mouth. The sputum is retained in the mouth and allowed to fall from their tongue into the pre-labeled container. Patient should be encouraged not to spit into the container. The patient can also be encouraged to cough directly into the cup.
- The patient’s mouth should not touch the container and the patient must ensure that sputum does not touch the outside of the container.
- The patient should not open the sputum cup till they are ready to use it
- They should not rub off the number written on the side of the container
- They should not touch the inside of the container with their fingers or tongue while collecting sputum
The person collecting the specimen should make sure that no one stands in front of the individual who is trying to cough up the sputum. When an individual has only coughed up saliva or has not coughed up at least 2 ml of sputum, they should be encouraged to give good specimen that is of appropriate quantity.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
When collecting sputum into containers, which of the following should not be done?
Cough deeply and directly into the sputum cup.
Sputum can sometimes touch the outside of the container.
Always close the lid tightly, after putting the sputum into the cup.
None of the above
2
When dispensing sputum into the sputum container, sputum must never touch the outside of the container.
Yes
Yes
Steps to Ensure a Good Quality Sputum Sample
ContentThe Healthcare Worker (HCW) needs to carefully explain how to collect a good quality sputum specimen. He/she needs to demonstrate how to bring up sputum from the chest, what a good sputum specimen looks like, and the quantity of sputum required.
Characteristics of a Good Sputum Sample
- Thick (semi-solid) muco-purulent (yellowish) in consistency, coughed out deeply from the lungs
- Sufficient in amount i.e., 2 to 5 ml (or enough to cover the size of a fingernail at the bottom of the container)
- It should not be blood-stained (brownish colour) as far as possible.
Steps to Ensure Good Quality Sputum Sample
- Explain to the patient the characteristics of sputum - that it is thick and mucoid as compared to saliva which is thin and watery.
- The patient should preferably rinse his/her mouth to get rid of any food particles which may give false-positive results.
- One should demonstrate to the patient by action how s/he should take deep breaths and bring up the sputum.
- The patient is instructed to inhale deeply (2–3 times), which will initiate the cough reflex in most patients.
- The sputum is retained in the mouth and spit into the pre-labelled container without spilling.
- Some patients may not be able to expectorate with deep breathing, in which case HCW should demonstrate to them how they should place their palms on the waist, squat or sit and continue deep breathing again.
- Tapping or thumping of the back may encourage expectoration. (Sitting and placing hands on the waist fixes the shoulder and pelvic muscles and brings the intercostal muscles of the ribcage and diaphragm into action).
- When a patient has only coughed up saliva or has coughed up less than 2 ml (the size of a fingernail at the bottom of the container) of sputum, the patient should be encouraged to provide a better specimen.
Resources
Receiving a biological specimen at the Laboratory
ContentBiological specimen/ samples collected on reaching a TB testing laboratory needs to be formally received. The sample may be handed over by agents(couriers, health staff/ volunteers, patient representatives) or by patients themselves. The formal receipt of sample enables further processes such as testing and communication of results back to the patient. If the sample is successfully received, the appropriate testing process is initiated using the sample, else it is rejected and a fresh sample requested.
The designated Lab Technician (LT) at the Laboratory is responsible for receiving the sample. To initiate the receipt, the sample along with the patient, or the sample along with accompanying test request is required. If it is available, following are the steps to complete sample receipt:
- Compare patient information (Patient Name and Patient ID / Sample ID/ Test ID) to the test request that has been made.
- This is performed by searching the patient ID in Nikshay under the Diagnostics menu and comparing and matching the patient details and the label on the sample.
- If a physical form (Request for examination of Biological specimen for TB) is available, the details on the sample label and form needs to be compared and matched as well.
- If the details are matched the LT then checks the quality (mucopurulent, non-blood stained), quantity (adequate to perform the requested test) of the sample and ensures that there is no leakage.
- If the above checks are passed, then the LT Accepts sample. If not the LT rejects sample with a request to get a new sample. The rejection of the sample and request to obtain a new sample is recorded on Nikshay and is communicated to the patient and the person who requested the test.
- To register the receipt by accepting/Check in the sample for testing in Nikshay. The relevant information may also be captured in the TB Laboratory Register. Ensure that the Test ID (if not already present) / Lab serial number from the Lab register is labelled on the sample container.
Sample receiving in Nikshay

Figure: Sample Journey Tracking in Nikshay; Source: Nikshay Diagnostic Training Content.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Nikshay Zendesk, Nikshay Knowledge Base, FAQs.
- Nikshay Zendesk, Nikshay Knowledge Base, Diagnostics.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The process of receiving a sample does not involve the following
Requesting a test
Matching test request information and container label.
Checking in a sample on Nikshay
Rejecting an inappropriate sample. 1 Request for testing and sample transportation to the laboratory has to happen before a sample can be received.
Matching request information and checking in a sample on Nikshay and rejecting inappropriate sample are steps in the receiving process.
Yes Yes - Compare patient information (Patient Name and Patient ID / Sample ID/ Test ID) to the test request that has been made.
Storing a sputum sample
ContentStorage conditions of sputum sample can effect the test results.
- Sputum samples should be transported to the laboratory as soon as possible after collection.
- It is the responsibility of Laboratory Technician (LT) and Senior TB Laboratory Supervisor (STLS) to ensure proper storage and transport of sputum specimens.
- Sputum is stored to preserve the specimen quality.
- The stored sputum samples should not be frozen.
Storage of Sputum Samples
For microscopy
- For smear microscopy, sputum specimens should be examined on the same day and not later than 2 days after collection.
- If delay is unavoidable, the sputum collected should be stored in a cool place/ refrigerated at 4°C to inhibit the growth of unwanted microorganisms.
- Stored sputum samples should be protected from light and heat to prevent liquefaction of the sample, else it makes the selection of mucopurulent part of the sample difficult.
- Samples received over holidays/weekends should be stored in a cool place/ refrigerated at 4°C.
For liquid culture
- Sputum should be stored in a cool place/ refrigerated at 4°C to inhibit the growth of unwanted microorganisms; not later than 3 days after collection.
For molecular tests - Nucleic Acid Amplification Test (NAAT) and Line Probe Assay (LPA)
- Sputum must be stored by refrigerating at 4°C to inhibit the growth of unwanted microorganisms and transported in cool chain to the nearest molecular laboratory. It should not be stored beyond one week at 4°C.
Resources
Technical and Operational Guidelines; Chapter 3: Case finding and diagnosis strategy
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The sputum collected expecting a time delay for processing should be stored in cool place/ refrigerated at 4°C.
True
False
1
The sputum collected expecting a time delay for processing should be stored in cool place/ refrigerated at 4°C.
Yes
Yes
-
STLS: Sputum Smear Preparation
FullscreenSteps involved in Smear Microscopy
ContentSputum smears must be prepared promptly after samples are collected or received in the laboratory.
Steps in smear preparation are as follows:
- Cleaning and Labelling of slide (No 1)
- Making the smear (No 2-3)
- Drying and Heat fixing the smear (No 4-5)
- Staining and counterstaining the smear (No 6- 12)
- Examination of slide/Reading the Smear (No 13-14)
- Reporting and recording the observations (Digitally and TB Lab register)
- Storage of slides (as per Laboratory Numbers in closed box) (No 15)


Figure: Steps in Smear Preparation; 1- Labelling of the slide, 2- Using a broomstick to pick up purulent portion (A) while avoiding the salivary portion (B), 3- Spreading sample on a glass slide, 4- Air-drying the slides, 5- Heat-fixing the smeared slides,6- Staining with 1% Carbol fuchsin, 7- Heating of stained smear, 8- Decolorize with 25% Sulphuric acid, 9- Rinse off decolourizer, 10- Counter stain with 0.1% Methylene blue, 11-Rinse off counter stain, 12-Drying the prepared slide, 13-14 Examination of smears , reporting of observations, 15-Storage of slides; Source: Laboratory Diagnosis by Sputum Smear Microscopy.
Resources
- Laboratory Diagnosis by Sputum Smear Microscopy - The Handbook, GLI, 2013.
- Module for Laboratory Technicians, CTD, 2005.
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Sputum smears should be dried by heating. True False 2 Sputum smears should be air-dried. Yes Yes Clean, fresh, unscratched slides should be used for smear preparation.
True False 1 Prevents deposits on stained smear. Yes Yes Cleaning and Labelling Slide
ContentA Laboratory Serial Number is assigned to each presumptive TB patient who is examined at the microscopy centre.
Each Laboratory Technician (LT) needs to ensure that all the slides are labelled using the Laboratory Serial Number. This is essential for recording as well as for the review of the slide during the supervisory visit as well as during the quality assurance exercise.
For every test, a new slide needs to be used. It is essential that there are no fingerprints or any scratches on the side of the slide (see figure 1).

Figure 1: Always select new, clean, grease-free and unscratched slides
Once the LT is ready to prepare a smear, he/she needs to write the Laboratory Serial Number on the left side of the slide with a diamond marker or a grease pencil only (see figure 2). Avoid multiple labelling (see figure 3).

Figure 2: The laboratory serial number is written on one end of the slide using a diamond marker

Figure 3: Avoid Multiple Labelling; a grease pencil has been used to label the slide.
Labelling of slides needs to be monitored and supported by the concerned Senior TB Laboratory Supervisor (STLS) during External Quality Assessment (EQA) visits.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Making the smear
ContentThe National TB Elimination Programme (NTEP) has a standard procedure for sputum smear preparation, the steps for which are listed below:
The tools required for smear preparation include a clean work surface, new and clean glass slides, a discard bucket or a foot-operated bin with a plastic liner, bamboo or wooden applicator sticks or sterile wire loop, spirit lamp and a rack for drying smears.
- Use new, clean, unscratched glass slides and label the slide with the laboratory serial number.
- Prepare the smear in the centre of the slide covering 3 cm X 2 cm
The smear is prepared by using either a wooden stick (Figure 2) or a sterile wire loop (Figure 3).

Figure 2: Wooden stick used in smear preparation

Figure 3: Sterile wire loop used in smear preparation
Steps for Smear Preparation Using a Wooden Stick
- Break the wooden stick into two halves with uneven ends.
- Using the uneven end, select and pick purulent portions of the sputum specimen and transfer onto a new, clean, labelled, glass slide.
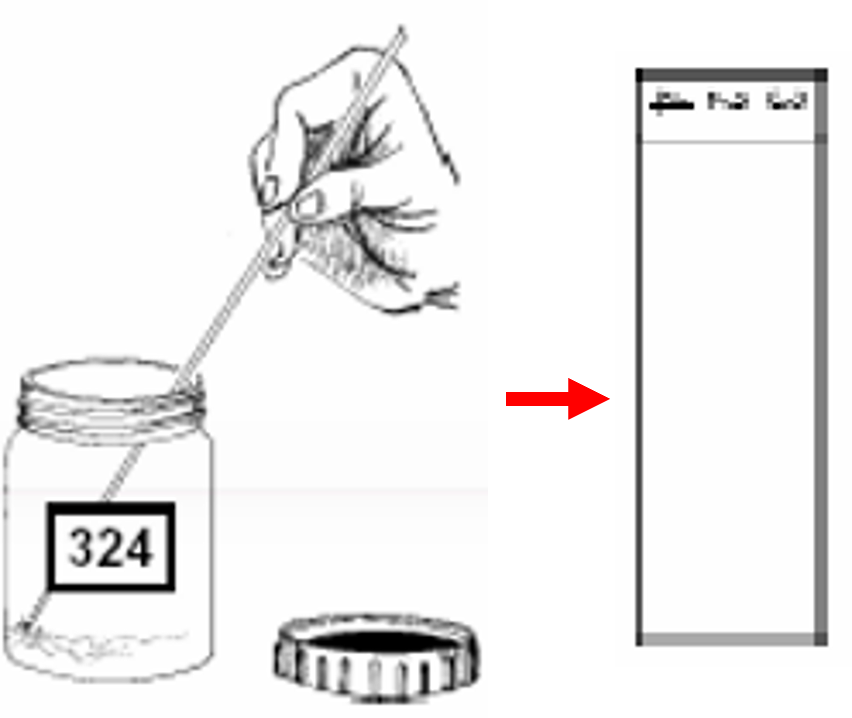
- Using the wooden stick, spread the sputum evenly, in a continuous rotational movement, to cover two-thirds of the central portion of the slide. Smear preparation should be done near a flame. This is required as approximately 6 inches around the flame is considered as a sterile zone which coagulates the aerosols raised during smear preparation.
- Discard the used wooden sticks in the discard bucket or a foot-operated bin with a liner and disinfectant. A different broomstick is used for each smear so that one patient's sputum is not mixed with another patient's sputum.

- Air-dry the smear slide on the rack for 30 minutes
- After air-drying, heat-fix the smear, using a lighted spirit lamp.
Steps for Smear Preparation Using a Wire Loop
- Take a nichrome wire loop or a disposable loop.

- Using the loop, select and pick purulent portions of the sputum specimen and transfer onto a new, clean, labelled, glass slide.
- Using the loop, spread the sputum evenly, in a continuous rotational movement, to cover two-thirds of the central portion of the slide.

- After use, sterilize the loop in an electric loop sterilizer or flame the loop to red-hot.


- Air-dry the smear slide on the rack for 30 minutes.
- After air-drying, heat-fix the smear using a lighted spirit lamp.
Resources
- Module for Laboratory Technicians (RNTCP), Central TB Division, MoHFW, 2005.
- Laboratory Diagnosis of Tuberculosis by Sputum Microscopy, GLI Initiative.
Kindly provide your valuable feedback on the page to the link provided HERE
Air drying and heat fixing
ContentFor sputum smear microscopy, the slides should be air-dried as heating the slide while the smear is wet can result in bubbling of TB bacilli into the air.
Fixation makes the sputum stick to glass slide and preserves the shape of the bacilli.
The procedure for air-drying and heat-fixing the slide is as follows:
- A smear prepared on a clean glass slide from mucopurulent portion of the specimen is air dried for 15-30 minutes on a rack (see Figure 1)

Figure 1: Rack for air-drying slides
- When dry, the smear facing upwards is fixed by heat from below. This can be achieved by passing the slide 2-3 times over the flame of a spirit lamp (as shown in Figures 2 and 3) for 3-4 seconds each time.

Figure 2: Fixing the Smear by Heat Fixation; Source: Laboratory Diagnosis by Sputum Smear Microscopy

Figure 3: Spirit lamp used to heat-fix smears
Important points to consider when fixing smears
- Heat fixing does not always kill Mycobacteria, exercise care when handling slides.
- Flame fixing may aerosolize bacilli from the smear.
- Overheating can damage the bacilli, burn the smear or break the slide.
- Insufficient heat or time can lead to smear washing off during staining steps.
- Heating for too short a period can result in a false-negative result because the TB bacilli will not be well preserved on the slide.
After the smears are fixed, they can be stained for examination or stored, or used in proficiency testing panel and quality control slides for staining.
Resources
Laboratory diagnosis by sputum smear microscopy
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Heat fixing does not always kill mycobacteria.
True
False
1
Heat fixing does not always kill mycobacteria.
Yes
Yes
Qualities of a good sputum smear
ContentGood quality smears are essential for accurate examination and results. A good quality sputum smear is one that is of uniform thickness and made from the mucopurulent portion of the sample in the center of the slide (Figure 1).
Do’s and Don’ts of a Good Quality Smear
- Do ensure that the smear size is 3 cm by 2 cm
- Do ensure there are no fingerprints on the prepared smear

Figure 1: Uniform spread of smear, not too thick or thin, and covering an area of 3cm by 2cm
- The smear should not be very thick, but it should be thin enough to visualize a newsprint as can be seen in Figure 2
Figure 2: Smear thin enough to visualise a print through it
- All smears should be air-dried for 30 minutes, before heat fixing to ensure that the smear is not washed off during staining
Common Mistakes to Be Avoided
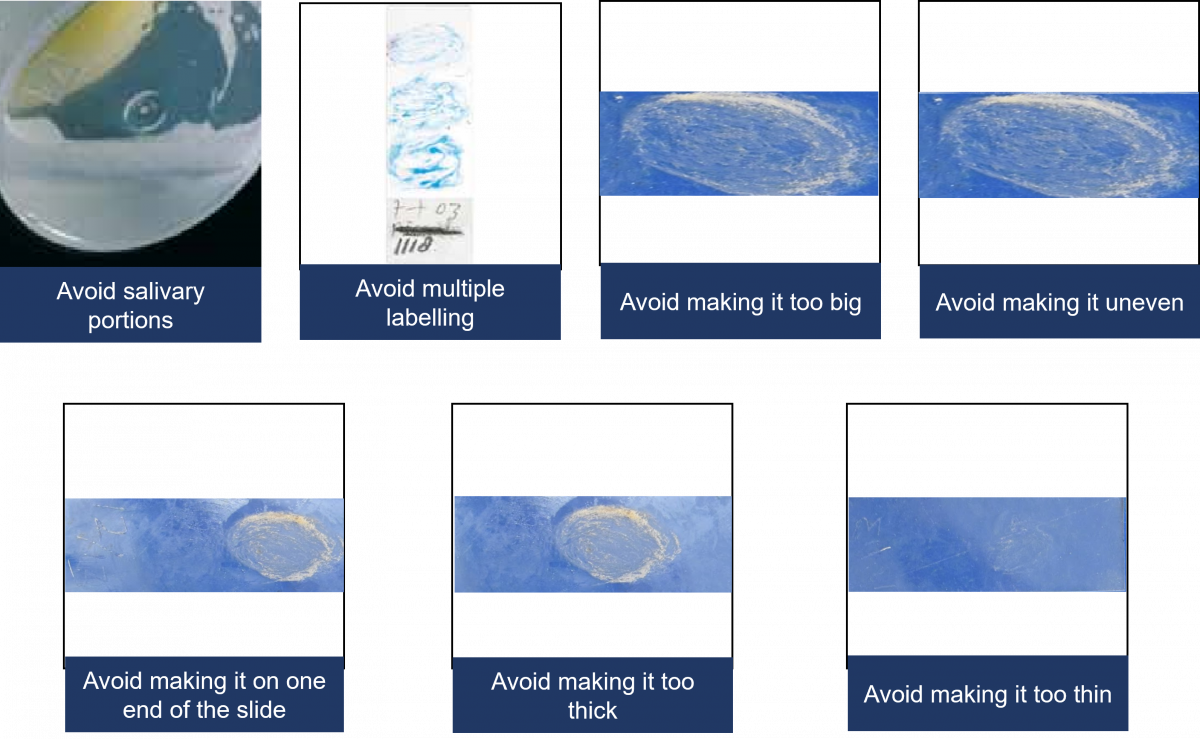
Resources
- The Handbook - Laboratory Diagnosis of Tuberculosis by Sputum Microscopy, 2013
- Module for Laboratory Technicians – RNTCP, 2005
- Manual for Sputum Smear Fluorescence Microscopy- RNTCP
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Preparation of Staining solutions
FullscreenPreparation of Reagents for ZN Microscopy
ContentThe National TB Elimination Program (NTEP) recommends freshly preparing reagents from commercial procured products, at the District TB units to be used for microscopy. Chemicals need to be carefully monitored for potency and the calculation needs to be accurate while preparing reagents for smear microscopy.
For Preparing 1% Carbol Fuchsin (500ml): The required chemicals and materials for preparing 500 ml Carbol Fuchsin are:
1. Basic Fuchsin
- Chemical name: Pararosaniline hydrochloride
- Chemical structure: C19H18N3Cl
- Molecular Wt: 323.8
- Colour: Metallic green
Potency correction factor: Note down the dye content – this should be available on the container. The dye content should be approximately 85% - 88%. To calculate the required amount of basic fuchsin, divide the actual amount required by the dye content. For example: dye content = 85%, actual amount required = 5gms, required amount of dye = 5/0.85 = 5.88 gms.
2. Ethyl Alcohol: 50 ml (Absolute alcohol, purity must be 98-100%)
3. Carbolic acid crystals (Phenol): 25 gms
- Chemical name: Phenol
- Chemical structure: C6H5OH
- Molecular Wt: 94.11
- Melting point: 40°C+2.5
4. Distilled purified water: 500 ml
Steps for Preparing 1% Carbol Fuchsin (500ml)
- Add 25 gms of phenolic crystals to a conical flask
- Add 50ml ethanol
- Mix well until the crystals completely dissolves. Add 50 ml distilled water if required.
- Conical flask should be kept in water bath set at 60°C or in a trough containing warm water
- Weigh required amount of basic fuchsin powder and transfer it into a conical flask
- Mix well until the crystals dissolve well.
- Make the total volume to 500ml by adding distilled water
- Filter using Whattman filter paper and transfer into a bottle
- Label as 1% Carbol Fuchsin - Primary stain
- Date of preparation, date of expiry, batch no. and the name of the technician or STLS who has prepared the stain should be clearly mentioned on the bottle.
- Store it in cool place, away from direct sunlight
- Any time particles start to form in the Carbol Fuchsin solution, the solution must be filtered again
For Preparing 25% Sulphuric Acid (500ml):
- Chemical structure: H2SO4
- Molecular wt: 98.08
- Purity: 95-97%
- Colour: Clear
- Measure 375ml distil water into a 1L flask
- In a glass cylinder, measure 125ml concentrated Sulphuric Acid. Pour it slowly and gently into the conical flask containing distilled water. Note: Always add acid to water. Never add water to acid
- To dissipate the heat generated, place the flask in a trough of water
- Mix well
- Allow to cool
- Transfer into a bottle
- Label as 25% Sulphuric Acid - Decolorizing Solution
- Date of preparation, date of expiry, batch no. and the name of the technician or STLS who has prepared the solution should be clearly mentioned on the bottle.
For preparing 0.1% Methylene Blue (500ml):
- Chemical name: Methylthionine chloride
- Chemical structure: C16H18ClN3S
- Molecular Wt: 319.9
Potency correction factor: Note down the dye content – this should be available on the container. The dye content should be approximately 82%. To calculate the required amount of methylene blue, divide the actual amount by the dye content. For example: dye content = 82%, actual amount required = 0.5gms, required amount of dye = 0.5/0.82 = 0.61 gms.
- Weigh the required amount of Methylene Blue
- Dissolve it in 500ml distilled water
- Transfer into a bottle
- Label as 0.1% Methylene Blue
- Date of preparation, date of expiry, batch no. and the name of the person who prepared the solution should be clearly written on the bottle.
Table: Preparation of different volumes of stains for ZN microscopy
Ziehl-Neelsen method
Quantity of reagent for 5L
Quantity of reagent for 1L
Quantity of reagent for 500 ml
Quantity of regent for 100 ml
Basic fuchsin (dye content/purity if 85%)
58.8 g
11.76 g
5.88 g
1.17 g
Alcohol
500 ml
100 ml
50 ml
10 ml
Phenol crystals
250 g
50 g
25 g
5 g
Distilled water
To make final volume 5000 ml
To make final volume 1000 ml
To make final volume 500 ml
To make final volume 100 ml
Carbol-fuchsin 1%
Sulfuric acid
1250 ml
250 ml
125 ml
25 ml
Distilled water
3750 ml
750 ml
375 ml
75 ml
H2SO4 25%
Methylene blue (dye content if 82%)
6.1 g
1.22 g
0.61 g
0.12 g
Distilled water
5000 ml
1000 ml
500 ml
100 ml
Methylene blue 0.1%
Always perform a quality check of the reagents prepared by using Quality Control Positive and Quality Control Negative. If purity is not available on the reagent bottle, then search the website of the company of which the reagent was procured or ask the company about the certificate mentioning about the purity of reagent
Please watch the video below for more information:
Video fileResources
- Module for Laboratory Technicians (RNTCP), Central TB Division, MoHFW, 2005
- TB Lab Consumables Specifications 2019
- SoP for preparation of Laboratory Reagents - WHO
- Laboratory Diagnosis of Tuberculosis by Sputum Microscopy, GLI Initiative
Kindly provide your valuable feedback on the page to the link provided HERE
Preparation of Reagents for FM Microscopy
ContentReagent preparation is an important activity and it’s essential to use certified chemicals and reagents. One should always check the potency of the chemicals used and calculate the amount to be weighed accordingly.
The following are the steps for reagent (primary stain and counter stain) preparation for Florescence Microscopy:
0.1% Auramine–O (1 L), the primary stain
- Weigh 1 gm Auramine–O and transfer to conical flask.
- Add 30 gm Phenolic crystals (99.5% purity) and mix well.
- Add 100 ml absolute Ethanol (98-100% purity) and mix well.
- Add 870 ml distilled water to make up final volume of 1 L.
- Filter and transfer to amber bottle.
- Label the bottle as 0.1% Auramine–O.
- Date of preparation, date of expiry, batch no. and name of the Senior TB Lab Supervisor (STLS) who has prepared the stain should be clearly mentioned on the bottle.
1% Acid Alcohol (1 L) to decolorize
- Dissolve 5 gm Sodium chloride in 250 ml distilled water.
- Add 5 ml concentrated hydrochloric acid.
- Mix with 750 ml absolute alcohol.
- Always add acid slowly to alcohol, not vice-versa.
- Store in amber coloured bottle.
- Label the bottle as 1% Acid Alcohol.
- Date of preparation, date of expiry, batch no. and name of the STLS who has prepared the stain should be clearly mentioned on the bottle.
0.5% Potassium Permanganate, KMnO₄ (1 L), the counter stain
- Weigh 5 gm of Potassium permanganate (99.5% purity).
- Transfer to a conical flask.
- Take 1 L of distilled water.
- Add small amounts of distilled water tothe conical flask containing KMnO₄ and mix well.
- Add the remaining distilled water to make up final volume of 1 L.
- Filter and transfer to a bottle.
- Label the bottle as 0.5% Potassium permanganate.
- Date of preparation, date of expiry, batch no. and name of the STLS who has prepared the stain should be clearly mentioned on the bottle.
Table: Preparation of Different Volumes of Stains for FM Microscopy
AURAMINE METHOD
QUANTITY OF REAGENT FOR 5 L
QUANTITY OF REAGENT FOR 1 L
QUANTITY OF REAGENT FOR 500 ML
QUANTITY OF REAGENT FOR 100 ML
Auramine
Ethanol
Phenol
Distilled water
0.1% Auramine
5.0 g
500 ml
150.0 g
To make final volume 5000 ml
1.0 g
100 ml
30.0 g
To make final volume 1000 ml
0.5 g
50 ml
15.0 g
To make final volume 500 ml
0.1 g
10 ml
3.0 g
To make final volume 100 ml
Hydrochloric acid
Sodium chloride
Ethanol
Distilled water
1% Acid–alcohol
25 ml
25.0 g
3750 ml
1250 ml
5 ml
5.0 g
750 ml
250 ml
2.5 ml
2.5 g
375 ml
125 ml
0.5 ml
0.5 g
75 ml
25 ml
Potassium permanganate
Distilled water
0.1% Potassium permanganate
25.0 g
5000 ml
5.0 g
1000 ml
2.5 g
500 ml
0.5 g
100 ml
Video fileResources
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Staining Sputum Smear
FullscreenZN Microscopy: Staining Process
ContentAfter air drying and heat-fixing of the smear, it needs to be stained for the identification of MTB during microscopy.
The reagents required for the ZN staining procedure are shown in Figure 1. The steps involved in the staining procedure are shown in Figure 2.

Figure 1: Reagents Required for ZN Staining

Figure 2: Steps involved in ZN staining procedure
For a visual representation of the above-mentioned steps, please click the video below.
Video fileResources
Laboratory Diagnosis by Sputum Smear Microscopy, GLI Initiative
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test When staining ZN slides, it is important to heat the slides until it begins to boil. True False 2 When staining ZN slides, it is important to heat the slides gently until you see vapours, but do not boil. Yes Yes ZN Microscopy: Properties of a well stained slide
ContentCharacteristics of a Well-stained Slide
- Staining and appearance of Mycobacterium species in ZN staining.
- The primary dye - carbol-fuschin stains all cells pink in sputum samples.
- The bacilli retain the primary pink carbol-fuschin on decolourisation with acid-alcohol.
- Epithelial, pus and mucous cells in the sputum decolourise on the addition of the acid-alcohol and take up the counterstain dye of methylene blue.
- Thus, Mycobacterium species appears pink against a background of epithelial, pus and mucous cells that appear blue.
- ZN-stained Mycobacterium species are visible as pink, long, slender rods with granules or V-shaped or in clumps.
- Mycobacterium species should not be stained too dark or pale pink.
- Possible reasons:
- Smear thickness is not appropriate
- Insufficient decolourisation
- Low acid concentration
- Carbol-fuchsin dries on smear
- Primary staining/ decolourisation time not appropriate
- Expired reagents used
- Possible solutions:
- Internal quality control of prepared smears and stains
- Use a stopwatch to time staining steps.
- Do not overheat carol-fuchsin.
- Possible reasons:
- The counter-stained cells should not be dark blue.
- Possible reasons:
- Smear thickness is not appropriate
- Excessive counterstaining time
- Inadequate washing after counterstaining
- Methylene blue concentration is not appropriate
- Possible solutions:
- Internal quality control of prepared smears and stains
- Use a stopwatch to time staining steps
- Possible reasons:
- There should not be any deposits on stained smears.
- Possible reasons:
- Stains not filtered
- Slides not clean
- Possible solutions:
- Internal quality control of prepared stains
- Filter stains
- Use clean, fresh, unscratched slides for smear preparation.
- Possible reasons:
Resources
- Laboratory Diagnosis of Tuberculosis by Sputum Smear Microscopy - The Handbook, GLI, 2013.
- Module for Laboratory Technicians, RNTCP, CTD, 2005.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of these is/are the characteristic/s of a well-stained slide? Mycobacterium species should not be stained too dark or pale pink. Mycobacterium species are visible as pink long slender rods with granules or V-shaped or in clumps. The counter-stained cells should not be dark blue. All the above 4 ZN-stained Mycobacterium species are visible as pink, long, slender rods with granules or V-shaped or in clumps. The bacilli should not be stained too dark or pale pink. The counter-stained cells should not be dark blue. Yes Yes - Staining and appearance of Mycobacterium species in ZN staining.
Fluorescent Microscopy: Staining Process
ContentAfter air drying and heat-fixing of the smear, it needs to be stained.
Fluorescence microscopy (FM) staining should always be carried out in a designated area. The reagents required for the FM staining procedure are shown in Figure 1. The steps involved in the staining procedure are shown in Figure 2.

Figure 1: Reagents Required for FM Staining


Figure 2: Steps involved in FM staining procedure
For a visual representation of the above-mentioned steps, please click the video below:
Video fileResources
Laboratory Diagnosis by Sputum Smear Microscopy, GLI Initiative
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the counterstain used in FM staining?
Acid Alcohol
Potassium Permanganate
Phenol
Auramine-O
2
In FM staining, Potassium Permanganate is used as the counterstain.
Yes
Yes
Fluorescent Microscopy: Properties of a well stained slide
ContentLight-emitting Diode Fluorescence Microscopy (LED-FM) utilises the fluorescent dye Auramine-O to stain and detect Mycobacterium species in clinical samples.
Characteristics of a Well-stained Slide
- Auramine-O stained Mycobacterium species are visible as bright yellow/ green long slender rods, slightly curved, with variable lengths, single or in clumps, with uniform staining or granular appearance against a dark background (Figure A).
-
Slides stained with Auramine-O should not have too much background fluorescence (Figure B)
Possible reasons:
- Smear thickness is not appropriate
- Insufficient decolourisation
- Counterstain too weak
- Auramine-O dries on the smear
-
Auramine-O not filtered
Possible solutions:
- Internal quality control of prepared smears and stains
- Use a stopwatch to time-staining steps
- Filter Auramine-O before use
- Add a sufficient quantity of stains to cover the smear
-
Slides stained with Auramine-O should not have pale fluorescence (Figure C)
Possible reasons:
- Smear thickness is not appropriate
- Low Auramine-O concentration
- Excessive decolourisation time
-
Stained smears exposed to daylight
Possible solutions:
- Internal quality control of prepared smears and stains
- Use a stopwatch to time-staining steps
- Store Auramine-O and stained slides in the dark
- Read stained slides as early as possible
- Non-fluorescent yellow/ green coloured bacillary shapes should not be considered as Mycobacterium species.
-
Slides stained with Auramine-O may contain stained artefacts/ background debris which are not Mycobacterium species.

Figure: Slides stained with Auramine-O showing bright yellow/ green slender rods (A); slide with too much background fluorescence (B); slide with pale fluorescence (C); Source: Laboratory Diagnosis by Sputum Smear Microscopy
Resources
- Laboratory Diagnosis of Tuberculosis by Sputum Smear Microscopy - The Handbook, GLI, 2013.
- Manual for Sputum Smear Fluorescence Microscopy, RNTCP, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of these is/are the characteristic/s of a well-stained FM slide? Mycobacterium species are visible as bright yellow/ green long slender rods against a dark background. Mycobacterium species are visible as pink, long slender rods.
Mycobacterium species are visible as pale yellow/ green long slender rods against a dark background. Mycobacterium species are visible as non-fluorescent yellow/ green coloured bacillary shapes. 1 Mycobacterium species are visible as bright yellow/ green long slender rods against a dark background. Yes Yes
-
STLS: Reading Smear and Reporting Microscopy results
FullscreenProcess of Reading a Smear
ContentThe manner and quality of smear reading has a major impact on the result of sputum smear microscopy and case detection. Each slide needs to be examined for at least 5 full minutes or 100 fields need to be examined.
The overall process of reading a smear is outlined in the figure below:

Figure: Process of reading a smear
Resources:
- AFB Smear Microscopy, Trainer Notes.
- Module for Laboratory Technicians.
- Laboratory Diagnosis of Tuberculosis by Sputum Microscopy.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the minimum time to be spent by an LT when examining a smear under the microscope?
30 minutes
5 minutes
2 minutes
30 seconds
2
Even the most experienced microscopist needs to examine each slide for at least 5 full minutes.
Oil immersion and focusing
ContentThe following are the measures to be kept in mind when adding immersion oil to the slide:
- Before adding immersion oil to the slide, ensure that the smear is facing upwards (Figure 1).
Figure 1: Slide should Face Upwards when Mounted on the Microscope Stage
- Add a drop of immersion oil, using the applicator (dropper bottle).
- The drop must fall freely onto the smear, so that the oil applicator does not touch the slide and get contaminated (Figure 2).

Figure 2: Oil Dropped onto Slide with an Applicator
- Mount the slide on the microscope and use the 10X objective lens to focus the smear, scan and look for mucoid material.
- Carefully rotate the 100X objective lens over the slide, adjust, sharp focus and observe under immersion oil.
Do’s and Don’ts:
- The 100X objective is the only lens requiring immersion oil.
- Keep the immersion oil away from other lenses.
- Use a good quality immersion oil.
- The immersion oil must have a medium viscosity and a refractive index (RI) greater than 1.5.
- Never allow the oil applicator to touch the slide.
- Do not use cedar wood oil diluted with xylene as it leaves a sticky residue on the lens and destroys the lens over time.
Resources
- Guidelines for Laboratory Consumables, Central TB Division, 2019.
- Laboratory Diagnosis of Tuberculosis by Sputum Microscopy, GLI Initiative.
Kindly provide your valuable feedback on the page to the link provided HERE
Reading a ZN stained smear
ContentImage
Resources
- AFB Microscopy Trainer Notes
- Module for Laboratory Technicians
- Laboratory diagnosis by sputum smear microscopy
Kindly provide your valuable feedback on the page to the link provided HERE
Reading a Fluorescent Stained slide
ContentSmears stained with the fluorescent dye, Auramine, are read with a Light Emitting Diode Fluorescence Microscope (LED-FM).
- The fluorescent-stained smears are to be read within 24 hours of staining in a dark room as the fluorescent stain fades on exposure to light.
- The slides are to be stored in the slide box to avoid exposure to light. Alternatively, they may be stored wrapped in brown or black paper and kept away from light.
- The slides should not be stored in a fridge as 4°C does not prevent or delay fading of fluorescent dye.
After fluorescent staining, smears are examined at much lower magnifications (typically 200x) than used for Ziehl Neelsen (ZN)-stained smears (1000x). Each field examined under fluorescence microscopy, therefore, has a larger area than that seen with bright field microscopy.
Examination Procedure
The steps include:
1. Switch on the LED-FM in a dark room.
2. Focus the stained slide using a 20x or 40x objective lens and view through the 10x eyepiece (magnification of 200x or 400x).
- Does not require the use of oil immersion.
3. Read smear in a linear pattern.
4. Count bacilli that appear as slender bright yellow fluorescent rods against a dark background in 30-50 fields. Rule out any artefact.
- For a trained and experienced Lab Technician (LT), each smear would take approximately 2 minutes for 30-50 fields or three horizontal sweeps.
Reporting Procedure
The smears are reported as negative/ scanty/ 1+/ 2+/ 3+ per the grading scale (Table).
Table: A Comparison between ZN (1000x) and FM (400x and 200x) for Grading of Smears at Different Magnifications
Result
1000 x magnification
1 length=100 HPF
400x magnification
1 length= 40 fields= 200 HPF
200x magnification
1 length=30 fields=300 HPF
Negative
Zero AFB/1 length
Zero AFB/1 length
Zero AFB/1 length
Scanty
1-9 AFB/1 length or 100 HPF
1-19 AFB/1 length
1-29 AFB/1 length
1+
10-99 AFB/1 length or 100 HPF
20-199 AFB/1 length
30-299 AFB/1 length
2+
1-10 AFB/1 HPF on average
5-50 AFB/1 HPF on average
10-100 AFB/1 field on average
3+
>10 AFB/1 HPF on average
>50 AFB/1 HPF on average
>100 AFB/1 field on average
Abbr: AFB: Acid Fast Bacilli; HPF: High Power Field
Resources
- Training Module (1-4) for Programme Managers and Medical Officers, NTEP, MoHFW, 2020.
- Manual for Sputum Smear Fluorescence Microscopy, RNTCP, MoHFW, 2007.
- Fading of Auramine-stained Mycobacterial Smears and Implications for External Quality Assurance.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Immersion oil is used to view fluorescent-stained smears.
True
False
2
Immersion oil is not required to view fluorescent-stained smears as they are observed with 20x or 40x objective lens.
Yes Yes Reporting and Recording results of Smear Microscopy (On paper)
ContentEach Designated Microscopic Center (DMC) needs to maintain a National TB Elimination Program TB (NTEP) Laboratory Register which collects information of all presumptive TB patients who undergo tests or confirmed patients who undergo follow-up tests.
- After doing the Acid-fast Bacilli (AFB) test, the laboratory technician needs to ensure that all the microscopy test results are entered against the name and the serial number of the presumptive/ confirmed TB patients.
- The result needs to be mentioned in terms of positive or negative test results along with the AFB grading.
- It is expected that the positive results are written in RED and negative in BLUE point pens.
- The AFB results can be mentioned for newly diagnosed TB patients for both spot as well as morning sample and must include the Nikshay ID of the patient as well as the test date and result.
- In case, the sample is repeated, the same is also mentioned.
- All the information also needs to be entered into NTEP Nikshay online application using a tablet or mobile phone.
- In a setting where Nucleic Acid Amplification Test (NAAT) is co-located, another sample needs to be tested for Rifampicin (Rif)-resistance and the same result also needs to be noted into the TB laboratory register.
- The performance of each laboratory is also entered into the monthly DMC extract called Annexure M which is consolidated for all DMCs by the concerned Senior TB Laboratory Supervisor (STLS).
- HIV and diabetes tests are also offered to each confirmed TB case and the details of the same are also part of the TB laboratory register.
- Patients who have been tested also need to be provided with the test results in a hard copy apart from the provision of information to the treating clinician of the health facility.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Reporting results of Microscopy (Digitally)
ContentResults of Ziehl–Neelsen (ZN) and Fluorescence Microscopy (FM) are added to Nikshay Diagnostic Module. After a patient is registered, test details are added which then leads to the page to add details on sample type, facility and test results (Figures 1-6).
Features of Nikshay Diagnostic Module
- A simplified user workflow for adding and updating test requests and results.
- Tests can be added and all the added tests’ history is available.
- Ability to map samples to one or more tests within Nikshay.
- A “Workbench” view is available to provide a single interface to view/ print/ copy the Test Summary, Add/ View Sample Details and Update/ View Result details.

Figure 1: Nikshay Screenshot to Add Tests under Diagnostics Module.
To add results for ZN/FM, the test types either Microscopy ZN or Microscopy Fluorescence should be selected from the drop-down menu (Figure 2).

Figure 2: Nikshay Screenshot to Add Reasons for Test under Diagnostics Module.
In case of follow-up with ZN/FM Microscopy, the reason for follow-up should be selected (Figure 3).

Figure 3: Nikshay Screenshot to add Follow-up ZN/FM Microscopy Test under Diagnostics Module.

Figure 4: Nikshay Screenshot to add Test Type for ZN/FM Microscopy and Facility Details under Diagnostics Module.
Details on sample type and sample description (mucopurulent/ blood-stained/ saliva) are added (Figure 5).

Figure 5: Nikshay Screenshot to add Sample Details and Description for ZN/FM Microscopy under Diagnostics Module.
Under test results, as shown in Figure 6, details of lab serial number, sample number, test date, test reported date and final interpretation of results are added based on the selection from a drop-down menu that includes options for:
- Negative
- Positive (1+, 2+, 3+)
- Positive (Scanty 1-9)
Figure 6: Nikshay Screenshot to add Test Results for ZN/FM Microscopy under Diagnostics Module.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What sample descriptions are added in Nikshay for ZN/FM Microscopy under Diagnostics Module?
Mucopurulent
Blood-stained
Saliva
All of the above
4
Sample descriptions (mucopurulent/ blood-stained/ saliva) are added in Nikshay for ZN/FM Microscopy under Diagnostics Module.
Yes
Yes
Generating the DMC Laboratory Register from Nikshay
ContentThe DMC lab register can be generated from Nikshay as a spreadsheet and stored electronically or printed for paper records.
Steps for generating DMC Register from Nikshay:
- Login to Nikshay Reports using your login ID and password.
- Under Reports, click on ‘Patient wise List’ and select the option for ‘DMC Register’ (see screenshot below)


Figure: Screenshot of Nikshay Reports to generate DMC Register
A few filters need to be selected to generate the register.
- First is the geographic location (State/ District/ TU/PHI); most of these are preselected.
- This is followed by a selection of the period for which the register has to be generated. This includes selection of ‘Frequency’ (either monthly or annually)of the report and the month or quarter for which the report is required.
- Click on the ‘Generate Excel’ button and it will lead you to a page from which you can download the register.
Things to remember:
- You can generate a DMC register for facilities below your login level (e.g., a district can generate a DMC register of a TB Unit or DMC of the same district. and a State can generate a register for any District under it)
- The data included in the register is based on the "Date reported" of a test.
Video fileVideo: Steps to access the DMC Register in Ni-kshay
Resource
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Where do you find the option to generate a DMC Register? In Nikshay under the "Admin" tab In Nikshay under the Others tab In Nikshay Reports under the "Patient wise List" tab In Nikshay Reports under the "Reports" tab 3 The option to generate a DMC Register is available under the Nikshay reports tab under the "Patient wise List" tab. Yes Yes
-
-
STLS: CBNAAT
Fullscreen-
STLS: CBNAAT as a Rapid Molecular Diagnostic tool
FullscreenStructure and Function of the CBNAAT Module
ContentThe CBNAAT module contains components that enable automated sample processing in the cartridge, and filling of the tube with the sample-reagent mixture for Polymerase Chain Reaction (PCR), followed by PCR amplification and detection.
The structure of the CBNAAT module is described below and shown in Figure 1:
- Syringe pump drive or plunger motor: Dispenses fluids into the different cartridge chambers
- I-CORE module: Performs PCR amplification and detection
- A cartridge loading and unloading mechanism ensures the proper movement of the cartridge in the instrument
- Reaction/PCR tube: Enables rapid thermal cycling and optical excitation and detection of the tube contents. The reaction tube is automatically inserted into the I-CORE module (hardware for PCR amplification and fluorescence detection) when the cartridge is loaded into the instrument.
- Valve drive: Rotates the cartridge valves to align the chambers with the syringe
- Ultrasonic horn: Lyses the sample
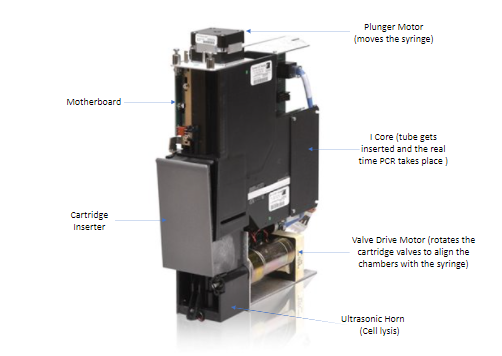
Figure 1: Structure of the CBNAAT module
The interior region of the cartridge insertion site also called cartridge bay and is shown in Figure 2.
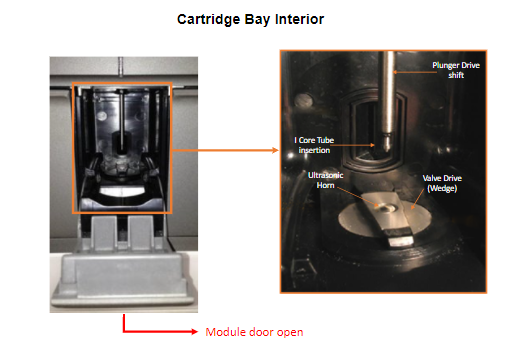
Figure 2: Interior of the Cartridge Bay
Mode of Operation of the CBNAAT Module
- The Intelligent Cooling/Heating Optical Reaction (I-CORE) module is the hardware component, within each instrument module, that performs PCR amplification and, fluorescence detection.
- As part of the cartridge load process, the PCR tube is inserted into the ICORE module.
- As the test starts, the sample and reagent mixture are pushed from the cartridge, into the PCR tube.
- During the amplification process, the ICORE heater heats up and the fan cools down the reaction tube contents.
Within the I-CORE, there is an optical system composed of two blocks: A six colour excitor and detector block excite the dye molecules, and detect the fluorescence emitted.
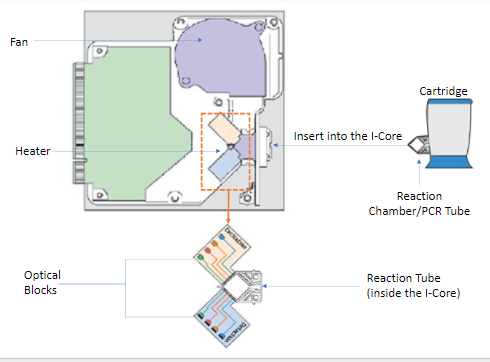
Figure 3: Mode of operation of the CBNAAT module
Video fileResources
Kindly provide your valuable feedback on the page to the link provided HERE
The CBNAAT Cartridge
Content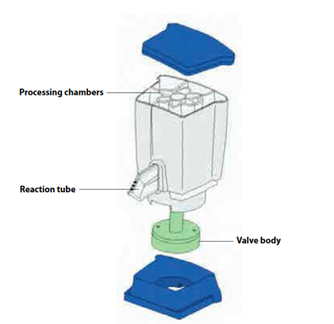
The disposable, single-use CBNAAT cartridge is a closed system unit to hold the samples and reagents. Inside of a CBNAAT Cartridge (CBNAAT operator manual). Each cartridge consists of the following components:
- Processing chambers: Hold samples, reagents, processed samples, and waste solutions. One chamber is designated as an air chamber to equilibrate pressures within the cartridge.
- Valve body: Rotates and allows fluid to move to different cartridge chambers and to the reaction tube. Within the valve body, the specimen is isolated, PCR inhibitors are removed, and the sample is mixed with PCR reagents and moved into the integrated reaction tube.
- Reaction tube: Enables rapid thermal cycling and optical excitation and detection of the tube contents. The reaction tube is automatically inserted into the I-CORE module (hardware for PCR amplification and fluorescence detection) when the cartridge is loaded into the instrument.
Video fileResources
Consumables required at CBNAAT Lab
ContentThe consumables required at a Cartridge-based Nucleic Acid Amplification Testing (CBNAAT) laboratory include the following:
CBNAAT/ GeneXpert Dx System consisting of CBNAAT machine preloaded with assay software, Computer and the Barcode reader
- CBNAAT assay kit (Figure) consisting of:
- CBNAAT cartridges: Kit contains 10 or 50 individually packed cartridges.
- CBNAAT reagent: 8 ml volume pack per cartridge. The sample reagent solution is clear but may range from colourless to golden yellow.
- Sterile pipette: Individually packed, disposable transfer pipettes, one per each test, with a single mark for the minimum volume of sample transfer to each cartridge.
- CD containing the Assay Definition File.

Figure: Contents of CBNAAT Assay Kit; Source: GLI Training Package for CBNAAT.
- Sputum containers
- Personal protective equipment:
- Laboratory coats
- Disposable gloves
- Disinfectants
- 1% Sodium hypochlorite solution
- 5% Phenol
- 70% Ethanol
-
Power stabiliser (UPS) for uninterrupted power supply to perform CBNAAT assay.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What are the components of the CBNAAT assay kit? CBNAAT cartridges CBNAAT reagent Sterile pipette All the 3 4 CBNAAT assay kit includes CBNAAT cartridges, CBNAAT reagent and sterile pipette. Yes Yes - CBNAAT assay kit (Figure) consisting of:
CBNAAT Testing Process Overview
ContentCartridge-based Nucleic Acid Amplification Test (CBNAAT) is used to detect Mycobacteria tuberculosis and rifampicin-resistance using GeneXpert IV Dx system and the Xpert MTB/ RIF cartridge.
The CBNAAT system integrates and automates sample processing, nucleic acid amplification, and detection of Mycobacteria tuberculosis and rifampicin resistance.
The system utilises the use of single-use disposable CBNAAT cartridges that hold the Polymerase Chain Reaction (PCR) reagents and hosts the PCR process.
The process involves the following steps:
- Sample processing: Specimens are processed by adding the sample reagent at 2:1 (v/v) ratio to the sputum sample, mixing and incubation for 15 minutes at room temperature. The sputum sample get liquified after the processing step.
- Loading sample into cartridge: Liquefied sample is added to the cartridge using a transfer pipette.
- Setting up the machine to run the test: After switching on the system, “Create Test” (Figure A) is clicked in the GeneXpert Dx system window, test details are added, the barcode label of the cartridge is scanned (Figure B) and “Start Test” (Figure C) is clicked to initiate testing.

Figure: Setting the machine to run the assay by creating test (A), adding test details, scanning barcode (B) to start test (C); Source: GLI Training Package for CBNAAT.
- Loading the cartridge: The instrument module door which displays the blinking green light is opened to load the cartridge. The door of module is closed firmly (an audible click sound should be heard). The green light stops blinking when the test starts.
- Obtaining the results: When the test is finished, the green light turns off. It takes around 1 hour 55 minutes to complete test run. On completion of test run, the result is generated automatically on the monitor.
- Ending the test run: When the system releases the door lock at the end of run, the module door is opened to remove the cartridge. The used cartridge is discarded.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Barcode is present on sterile pipette and CBNAAT cartridge.
True
False
2
Barcode is present on CBNAAT cartridge.
Yes
Yes
Other CBNAAT tests available
ContentIntroduction
Cartridge-based Nucleic Acid Amplification Test (CBNAAT) is an automated rapid molecular diagnostic test which detects targeted Deoxyribonucleic Acids (DNA) sequences of Mycobacterium tuberculosis (M.tb) genome by Real-time Polymerase Chain Reaction (RT-PCR) method.
CBNAAT uses the GeneXpert IV Dx system and the single-use disposable Xpert M.tb/ Rifampicin (RIF) cartridges that hold the Polymerase Chain Reaction (PCR) reagents and host the PCR process.
The various TB tests utilizing the CBNAAT platform:
1) GeneXpert MTB/ RIF
- The Xpert M.tb/ RIF assay is a Nucleic Acid Amplification Test (NAAT) that uses a disposable cartridge with the GeneXpert Instrument System to quickly identify possible Multidrug-resistant TB (MDR-TB) that is resistant to RIF.
- This test yields rapid results, i.e., within 2 hours and is therefore cost and time-saving.
2) GeneXpert MTB/ RIF Ultra
- The Xpert M.tb/ RIF Ultra assay is similar to the Xpert MTB/ RIF assay, just that it is even faster with a higher level of accuracy.
- The results are obtained in 80 minutes.
- It can detect paucibacillary TB disease.
3) GeneXpert MTB/ XDR
- This is a GeneXpert M.tb assay that detects mutations associated with Resistance Towards Isoniazid (INH), Fluoroquinolones (FLQ), Second Line Injectable Drug (SLID) (amikacin, kanamycin, capreomycin) and Ethionamide (ETH) in a single test.
4) GeneXpert Omni/Edge
- GeneXpert Omni/Edge is a battery-operated, wireless and web-enabled portable molecular diagnostics system, intended for use as the point-of-care diagnostic tool in remote and challenging settings.
- It is a single-slot platform i.e., runs one test per cycle, uses a 2-in-1 tablet/laptop and a compact printer and is expected to enable accurate, fast and cost effective test results.
Apart from TB, the CBNAAT platform can be used to diagnose several other pathogens using different cartridges. One of the common other pathogens detected using CBNAAT in India is COVID-19.
Note: Except GeneXpert MTB/ RIF , other CBNAAT tests are not currently being endorsed by NTEP.
Resources
- WHO Consolidated Guidelines on Tuberculosis. Module 3: Diagnosis - Rapid Diagnostics for Tuberculosis Detection 2021 Update.
- Guidelines for Programmatic Management of Drug-resistant TB (PMDT) in India; NTEP, CTD, MoHFW, India, 2021.
- Sachdeva K, Shrivastava T. CBNAAT: A Boon for Early Diagnosis of Tuberculosis-Head and Neck; Indian J Otolaryngol Head Neck Surg, 2018.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ‘Xpert M.tb/ RIF Ultra yields results faster than Xpert M.tb/ RIF’.
True
False 1 Xpert M.tb/ RIF Ultra yields results in approx. 80 minutes compared to Xpert M.tb/ RIF which gives results in approx. 110 minutes.
Yes Yes GeneXpert MTB/ RIF is the only CBNAAT tests that is endorsed by NTEP.
True False 1 Other tests using CBNAAT platform GeneXpert MTB/ RIF Ultra, GeneXpert MTB/ XDR and GeneXpert Omni/Edge are not endorsed by NTEP. Yes
Yes
Inbuilt Controls of CBNAAT Technology
ContentThe CBNAAT System automatically performs internal quality control for each sample.
During each test, the system uses the following inbuilt controls:
System Check Control (SCC)
- Checks integrity of the instrument, cartridges and PCR reagents.
Sample Processing Control (SPC)
- Ensures that a sample is correctly processed.
- Included in the cartridge and is processed with the sample. The DNA is detected by a PCR assay.
Probe Check Control (PCC)
- Performed during the first stage of the test.
- Verifies the presence and integrity of the labelled probes.
Video fileVideo 1: CBNAAT Technology -Inbuilt Controls
Video fileVideo 2: Summary of all In-built Control Checks
Resources
-
STLS: Sample processing for CBNAAT
FullscreenSpecimen Processing for CBNAAT
ContentThe CBNAAT system integrates and automates sample processing with amplification and detection of the target sequences
For sample processing, sample reagent is provided in CBNAAT kit, 8ml volume pack per each cartridge
- The sample reagent solution is clear but may range from colourless to golden yellow
Processing of clinical specimens should be performed as per laboratory biosafety standards
- Treat all sputum specimens as potentially infectious
- Wear protective gloves and laboratory coats when handling specimens and reagents
Sample processing from direct sputum and decontaminated sputum sediments is described in the Video given below -
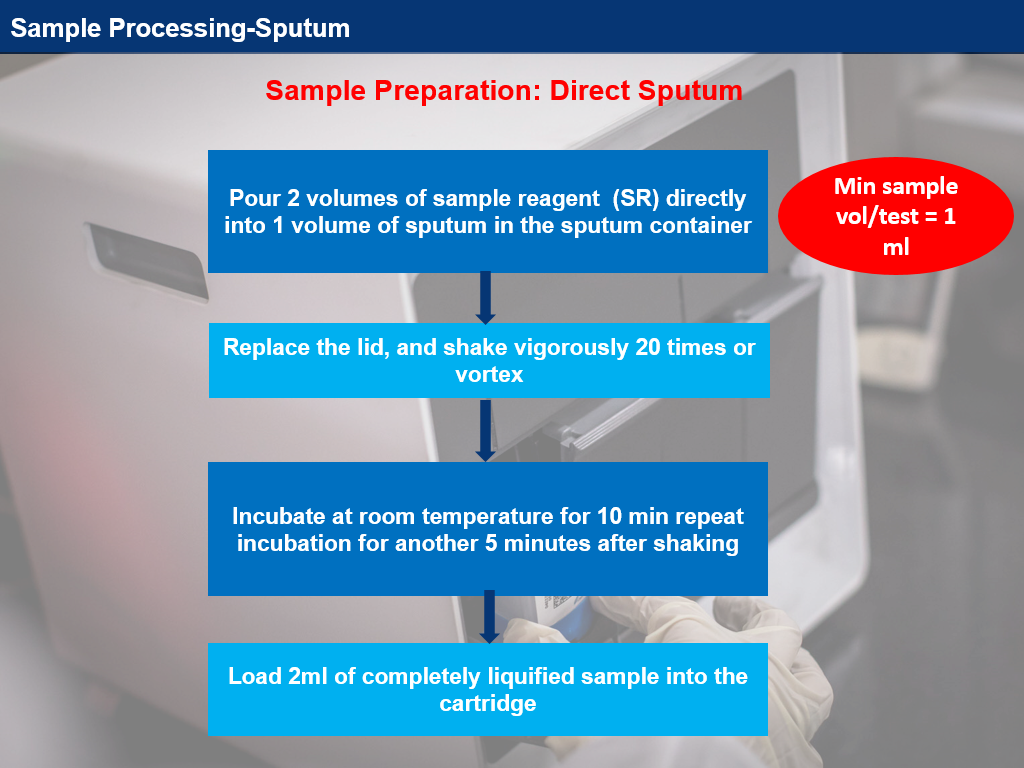
Video 1: Sample processing from direct sputum; Source: Challenge TB: Sample Processing Sputum
Video fileVideo : Specimen Processing for CBNAAT
Resources
CBNAAT Cartridge Loading
Content- Use the sterile transfer pipette provided in the CBNAAT kit to draw liquefied sample into the transfer pipette
- The minimum amount to be loaded into the cartridge is 2 ml
- Do not process the sample if there is insufficient volume
- Open the cartridge lid
- Transfer the sample into the open port (Figure 1) of the CBNAAT cartridge and dispense slowly to minimize the risk of aerosol formation
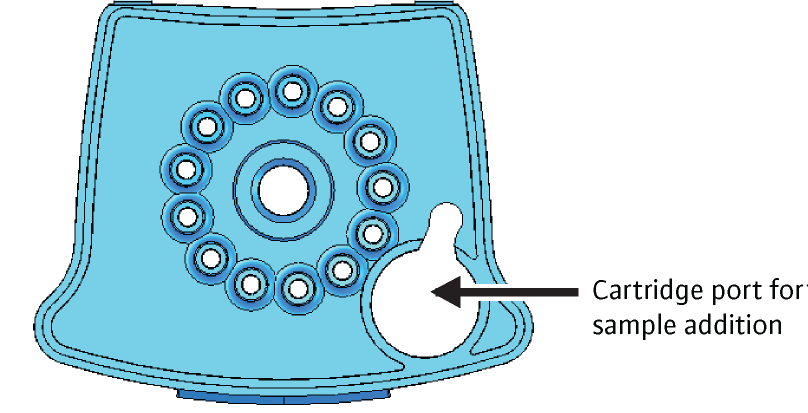
Figure 1: CBNAAT cartridge (top view) to show the open port
(SOP for GeneXpert MTB/RIF)- Discard the transfer pipette
- Snap the lid shut to close firmly
- Turn on the CBNAAT instrument
- Open the instrument module door, which displays the blinking green light
- Load the cartridge and close the door of the module firmly
- The test should be started within 30 minutes of adding liquefied sample to the cartridge
- The remaining liquefied sample may be kept for up to 12 hours at 2-8°C (for repeat testing)
Video fileVideo 1: CBNAAT loading
Video fileVideo 2: Sample Loading (Demonstration)
Resources
- Use the sterile transfer pipette provided in the CBNAAT kit to draw liquefied sample into the transfer pipette
CBNAAT Sample Processing for Other Body Fluids
ContentThe following procedures are recommended when processing various body fluids with the Cartridge-based Nucleic Acid Amplification Test (CBNAAT):
Bronchoalveolar Lavage (BAL):
Processing of BAL for CBNAAT assay is given here. However, it is important that each laboratory optimizes this protocol to minimize the error rate.
If the BAL volume is sufficient (approx. 5 ml), centrifuge and dissolve sediment into 1 ml sterile phosphate buffer/ saline, then add sample reagent in a 1:2 ratio.
If the BAL volume is less (less than 5 ml), take 1 ml and add 2 ml of sample reagent.
- If the BAL is mucoid or has more than 0.5% blood contamination, decontaminate using N-acetyl-l-cysteine–sodium hydroxide (NALC-NaOH) treatment.
- Decontamination of BAL should also be carried out if the error rate is more than 2%.
Pericardial/ Ascitic/ Synovial Fluid:
If the sample volume exceeds 5 ml, centrifuge and dissolve sediment into sterile phosphate buffer/saline to make volume 1 ml, then add sample reagent in a 1:2 ratio.
If the sample volume is less than 5 ml, take 1 ml and add 2 ml of sample reagent.
- Pleural fluid is a suboptimal sample, and pleural biopsy is preferred.
- A positive CBNAAT result in pleural/body fluid can be treated as TB, a negative result should be followed by other tests.
- Decontaminate/concentrate using standard NALC-NaOH treatment if bloody (more than 0.5% blood), thick and/or clots are present.
Pus/ Abscess/ Aspirates/ Semen:
- Liquid/ slightly viscous specimen: Use sample-to-sample reagent 1:2 ratio, mix well and follow routine CBNAAT protocol.
- If very thick, viscous or bloody specimens: Add 2 ml sample reagent to 0.2 - 0.3 ml pus, mix well to the vortex, and increase the incubation time, if required.
- Decontaminate, if required (>0.5 % blood).
*Each laboratory must optimize these protocols to minimize the error rate.
Resources
-
STLS: CBNAAT Result Interpretation and Recording
FullscreenVisualization of CBNAAT Test Results
ContentThe test results of the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) assay are displayed in the ‘View Results’ window, of the CBNAAT software.
For visualizing the results after the test is completed:
- In the CBNAAT Dx System window, click View Results on the menu bar.
- The View Results window appears.
- To select a test result, click View Test.
- ‘Select Test to Be Viewed’ - dialog box appears.
- Select the test of interest.
- Click OK.
Note: The selected test result appears in the ‘View Results’ window. A result will be displayed in PDF format.
To generate a PDF report
- To generate a report in PDF format, click on “Report” and then select the result you want.
- The PDF report will be generated.
Interpretation of Test Results
- The ‘View Results’ window displays information about the test, such as sample ID and run-time on the left-hand side panel.
- The interpretation of the result is in the center, and the real-time PCR amplification curves are displayed at the bottom.
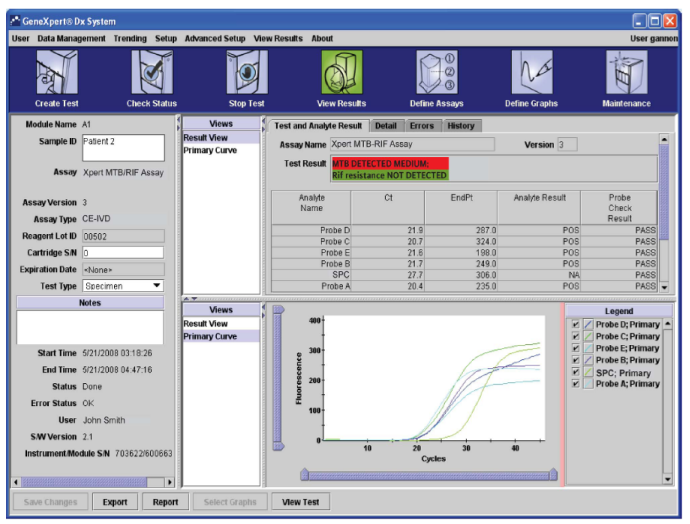
Figure: User 'View Results' Window showing the information about test, interpretation of results and real-time PCR curves
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
CBNAAT Results Interpretation
ContentOn completion of a test run, the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) gives the following results:
- MTB DETECTED; Rif Resistance DETECTED
- MTB DETECTED; Rif Resistance NOT DETECTED
- MTB DETECTED; Rif Resistance INDETERMINATE
- MTB NOT DETECTED
- Error
- Invalid
- No result
Conclusive results include: MTB NOT DETECTED, MTB DETECTED with Rif Resistance/ without Rif Resistance.
Non-conclusive results include: MTB Detected, Rif Resistance Indeterminate, Errors, Invalid and No Result - the test has to be repeated in these cases.
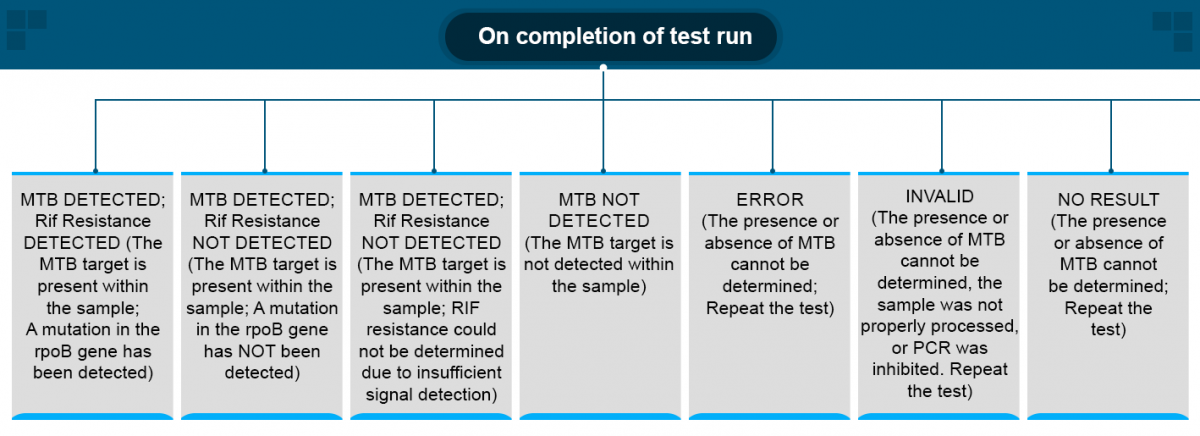
Figure: CBNAAT Result Algorithm
Video fileVideo : CBNAAT Results Interpretation
Resources
CBNAAT Assay Limitations
ContentThe Cartridge-based Nucleic Acid Amplification Test (CBNAAT) test has some limitations such as:
- Bacterial load below the Limit of Detection (LOD ~ 130 CFU/ml) may result in a false-negative result.
- Patients on an anti-TB regimen can still have positive results due to killed bacilli in the specimen and hence cannot be used for follow-up.
- A positive test result does not necessarily indicate the presence of viable organisms. It is, however, presumptive for the presence of Mycobacterium tuberculosis (MTB) and Rifampicin (Rif) resistance.
- MTB detection is dependent on the number of organisms present in the sample. Quality specimen collection and timely processing of the sample will minimize the errors.
- Test results might be affected by anti-TB medication. Therefore, therapeutic success or failure cannot be assessed using this test, because DNA might persist following antimicrobial therapy.
- Mutations or polymorphisms in primer or probe binding regions may affect the detection of new or unknown MDR or Rif-resistant strains, resulting in a false-negative result.
- Any modification in sample processing may alter the performance of the test.
- Results should be interpreted in conjunction with clinical data available to the clinician.
Video fileVideo:
CBNAAT Assay Limitations
Resources
Retest Procedure for CBNAAT
ContentThe assay needs to be repeated by using a new cartridge if one of the following test results occur:
INVALID: An INVALID result indicates that Sample Processing Control (SPC) failed. The sample was not properly processed, or Polymerase Chain Reaction (PCR) was inhibited.
ERROR: An ERROR indicates that Probe Check Control (PCC) failed, and the assay was aborted possibly due to the reaction chamber being filled improperly, a reagent probe integrity, syringe pressure issues, or failure of the CBNAAT module.
NO RESULT: A NO RESULT indicates that insufficient data were collected. For example, the operator stopped a test that was in progress.
RIF Indeterminate: RIF indeterminate result indicates that the sample has a less bacterial load.
Program guidelines recommend obtaining a second specimen to confirm rifampicin resistance in these scenarios.
How to Perform the Retest?
- Leftover sputum or fresh sputum or reconstituted sediment:
Treat it with a new Sample Reagent (SR) and load it into the new CBNAAT cartridge.
- Sufficient leftover SR-treated sample:
Use within 4 hours of initial addition of SR to the sample - Load into the new CBNAAT cartridge.
Do not use SR-treated sample if it is more than 4 hours old - Over-treatment may lead to false-positive test results.
Always use a new cartridge!
Video fileVideo : Retest Protocol for CBNAAT
Resources
-
STLS: Troubleshooting in CBNAAT
FullscreenTroubleshooting Process for CBNAAT
ContentThe most common situations that need troubleshooting while using CBNAAT are:
- Hardware or instrument problems
- Failures without error codes
- Failures with error codes
Troubleshooting Approach
- In case of an issue, a message will be displayed (often with an error code).
- Check if the error affects one particular module.
- Refer to the CBNAAT user manual and follow the recommended corrective action.
If the problem persists, continue to use other modules in the meantime (if possible), and exclude the faulty modules from the tests. Contact the technical support team.
How to reach the technical support team?
Image
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Hardware Problems with the CBNAAT Machine
ContentCommon hardware problems that can occur while using the CBNAAT machine and their recommended solutions are listed below.
- The system does not start - The instrument power connections can be checked.
- Hardware failure - The system can be turned off and software can be updated.
- The CBNAAT modules are not detected - Network cable can be connected, the software can be re-launched, IP address can be reset.
- The barcode scanner is not working - Re-plug the scanner into the computer.
- The red light on the instrument module is blinking - Perform a self-test manually and call technical support if the problem persists.
- The cartridge is stuck in the module - Click on ‘Maintenance’ on the CBNAAT system window, choose ‘Open module door or update EEPROM’ and ‘Open door’ to open the module door. Call technical support if the problem still exists.
- The test report is not printed at the end of the run - Check if the printer is online, paper is present, and toner is okay.
- Unable to create a test - Check that the assay is selected, assay dyes are calibrated, modules are not disabled, and the module temperature is checked.
- Unable to start a test - Check module reporters in the maintenance window, assay reporter is present and calibration status is valid.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
CBNAAT Hardware Problem: Barcode Scanner Failure
ContentIf the barcode scanner is not working, enter the cartridge barcode manually (Figure):
- Step 1: Click on “Create Test”
- Step 2: A dialogue box - Scan Cartridge Barcode will appear. Click on “Manual Entry”
- Step 3: Manually type the 2-line numbers of the cartridges
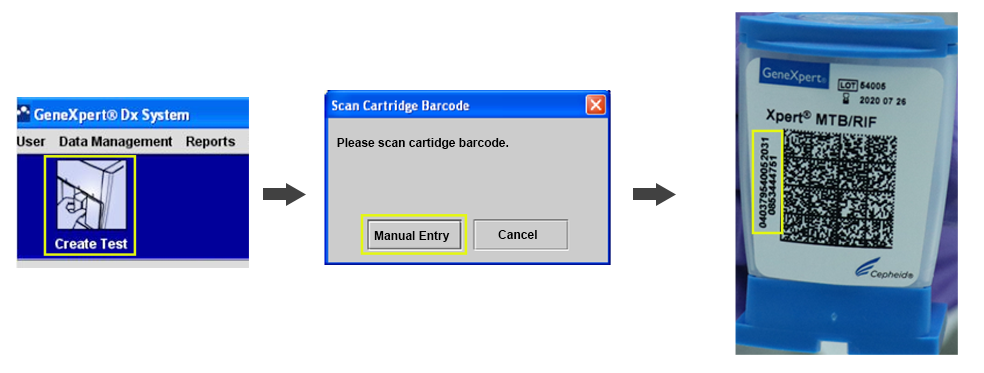
Figure: Process for Manual Entry of the Cartridge Barcode
In case of barcode reader failure, while using a new lot, this action cannot be performed. Contact the manufacturer or technical support to collect the Lot Specific Parameter.
Also, contact customer care for repair or replacement of the barcode reader.
Video fileResources
CBNAAT Hardware Problem: Stuck Cartridge
ContentThis hardware problem occurs when a cartridge is stuck inside a CBNAAT module.
Causes
- Module mechanical malfunction during the test
- Electrical failure
Solutions for releasing a stuck cartridge
Solution 1: Verify that the module door is not open. Gently try to open the module door.
Solution 2: Try to remove the cartridge from the software.
- In the CBNAAT System window, click ‘Maintenance’ on the menu bar and select ‘Open Module Door or Update EEPROM’ (see the figure below).
- Select the module. Click “Open Door” to open the module door.
Figure: CBNAAT system showing ‘Open Module Door’ and ‘Perform Self-Test’

Solution 3: If the door does not open, close the software, and re-launch the software.
When the software is re-launched, the module will reinitialize itself by putting the valve and the syringe in the correct position. This may help to open the door.
Solution 4: Turn the system off and restart the CBNAAT instrument and software.
Solution 5: In the CBNAAT system window, choose ‘Maintenance’ on the menu bar and select ‘Perform Self-Test' (see figure above).
Solution 6: If none of the solutions above work, manually remove the cartridge.
If the cartridge is not released, contact technical support, to manually remove the cartridge. If you are a senior lab supervisor, you may click here to see the steps to manually remove a stuck cartridge.
Video fileVideo : CBNAAT Hardware Problem: Stuck Cartridge
Resources
CBNAAT Hardware Problem: Modules Not Detected
ContentOne of the common problems encountered while using the CBNAAT machine is the non-detection of the module.
Usually, there is a loss of communication between modules and software, leading to non-detection.
Origins:
- Ethernet connection between Personal Computer (PC) and CBNAAT is bad
- Power supply issue (main power or Universal Power Supply (UPS) fluctuations)
- Bad connection points between gateway board and modules
- Too high room temperature
Solutions:
- Restart the instrument first and then the computer.
- Unplug and re-plug the ethernet cable between the PC and the instrument, then restart as above.
- Secure the power supply and use an adapted UPS/ surge protector.
- Check the temperature inside the module (should be below 39°C).

Figure: Troubleshooting protocol for the non-detection of CBNAAT Module
Video fileVideo : CBNAAT Hardware Problem: Modules Not Detected
Resources
Monitoring Different Types of Errors with CBNAAT
ContentWhile using the CBNAAT machine in a laboratory setting, many different causes can lead to an error (indicated on-screen as ‘ERROR’, as in figure 1).
Figure 1: Window showing how to click on “Errors” to learn more about the issue
Error Message Categories
The errors are displayed by the instrument’s software to highlight various technical issues that disrupt the test process. They are grouped into five categories by the software:
- Cartridge loading errors: Errors that occur during a cartridge loading process
- Self-test errors: Errors that occur during the self-test process
- Run-time errors: Errors that occur during a test.
- Operation terminated errors: Errors that abort a test
- Post-run analysis errors: Errors that occur during the data reduction process
You can view the errors by clicking the ‘Check Status’ icon on the CBNAAT software, as seen in figure 2.
Figure 2: 'Check Status' Window of the CBNAAT Software
Monitoring of Errors and Invalid/ No Results
- Rates of errors and Invalid/ No Results need to be monitored by the module and user.
- Identifying the most frequent types of problems can help to troubleshoot since certain errors may be associated with a user’s technique in sample processing while others with mechanical problems with the instrument modules or room temperature.
- Recurring errors should be timely reported to the manufacturer.

Figure 3: Monitoring of Errors on CBNAAT
Video file
Video : Monitoring Different Types of Errors with CBNAAT
Resources
CBNAAT Troubleshooting: Error- 5006, 5007, 5008 and 5009 [PCC Failed]
ContentErrors 5006, 5007, 5008 and 5009 (Probe Check Control Failed) sometimes appear on the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) machine in TB laboratories and need troubleshooting.
Problem:
Probe Check Control (PCC) failed, and the test was stopped before amplification.

Origins:
- Incorrect storage of cartridges (probe integrity issues detected)
- Dust on optical filters
- Sample too viscous
- Incorrect sample volume
- Improper fluid transfer (bubbles)
Solutions:
- Store the kits between 2 - 28°C.
- Use an optical brush to clean the optical filters (without a cleaning solution).
- Make sure the sample is totally liquified before transferring it to the cartridges.
- Add the correct volume of the specimen.
- Avoid making bubbles.
Video fileVideo : CBNAAT Troubleshooting: Error- 5006, 5007, 5008 and 5009 [PCC Failed]
Video fileVideo : Probe Check Control (PCC)
Resources
CBNAAT Troubleshooting: Error- 2008 and 2009
ContentDuring the use of the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) machine, Error- 2008 and 2009 may appear on the screen and needs troubleshooting.
Problem:
2008: Pressure reading exceeds the maximum
2009: Syringe pressure is below the protocol limit
Figure: Error 2008
Origins:
- The cartridge filter is clogged (due to too viscous sample or particles)
- Pressure sensor failed
Solutions:
- Make sure the sample does not contain any solid particles.
- Make sure the sample is totally liquified before transferring it to the cartridges.
- If after 15 minutes of incubation with the sample reagent, the sample is still too viscous, wait up to 10 more minutes.
- Use a new cartridge and add only a sample reagent to test. If the problem persists, it is likely a module problem: Contact Technical Support.
Video fileVideo : CBNAAT Troubleshooting: Error- 2008 and 2009
Resources
CBNAAT Troubleshooting: Error- 2014, 3074, 3075 and 1001 (Heating Component Related Issues)
ContentError - 2014, 3074, 3075 and 1001, in the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) machine are related to ‘Heating Component Related Issues’.
Problem:
Temperature/ Heater Failure
Origins:
- High temperature in module
- Heater component failure
- Broken fan
- Dust on filter near the fan
Troubleshooting:
In the CBNAAT Dx System window:
- Click “Maintenance” on the menu bar
- Select “Module Reporters” to check module temperature

Figure: Troubleshooting Heating Component Related Issues
If the problem persists, one needs to contact the manufacturer for technical support.
Video fileVideo : CBNAAT Troubleshooting: Error- 2014, 3074, 3075 and 1001 [Heating Component Related Issues]
Resources
CBNAAT Troubleshooting: Failures without Error Codes
ContentSome Cartridge-based Nucleic Acid Amplification Test (CBNAAT) machine errors will indicate test failure without Error Codes.
Error: Invalid
Problem:
Sample Processing Control (SPC) failed.
Origin:
Polymerase Chain Reaction (PCR) was inhibited due to food particles or blood in the sample.
Solution:
Laboratory Technician (LT) needs to collect another specimen, if necessary.
Prevention:
- Before mixing with the sample reagent for decontamination, check whether the sample contains food particles or blood.
- Allow food particles to settle down before adding the sample to the cartridge.
If the problem persists, one needs to contact the manufacturer for technical support.
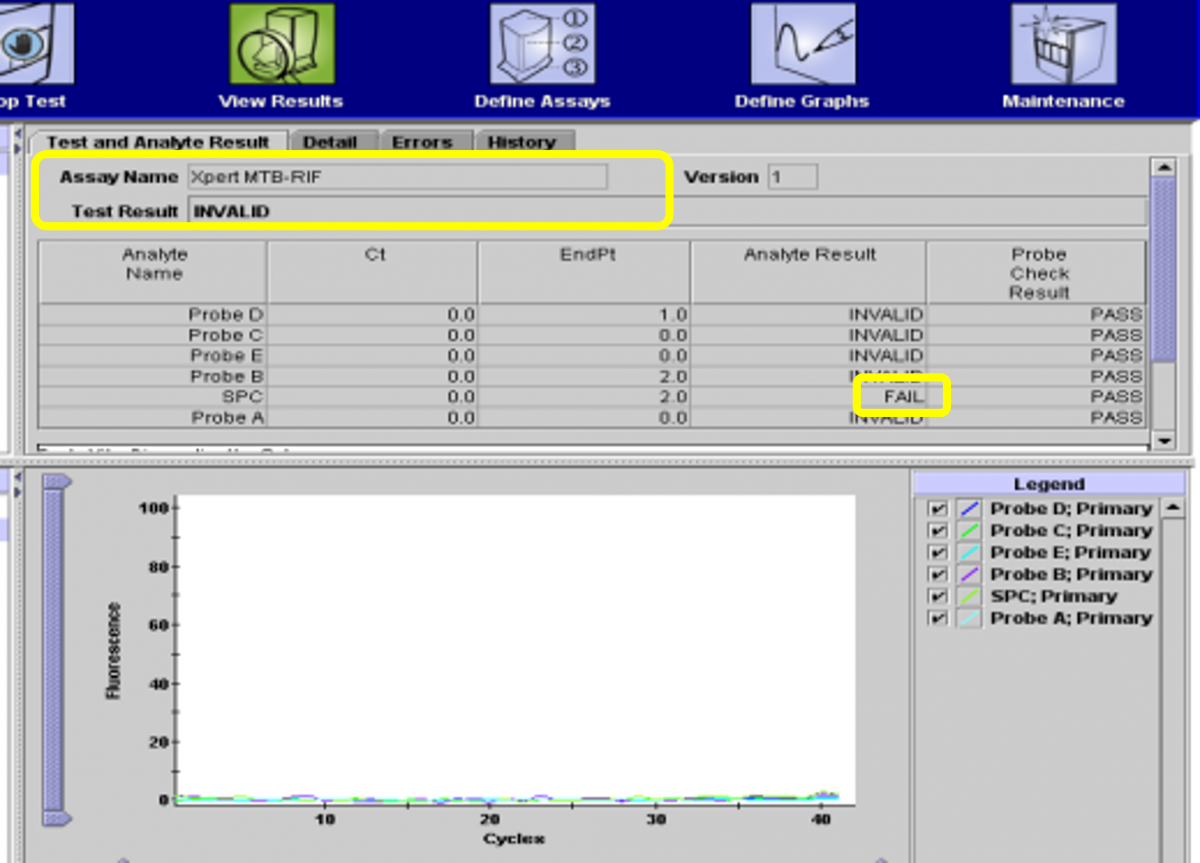
Figure: Error - Invalid
Error: No Result
Problem:
Test could not be completed and insufficient data collected.
Origins:
Software stops working before the test is completed due to:
- Windows or software freeze
- Power failure
- STOP TEST function was activated (accidentally or deliberately)
Solution:
Secure the power supply, restart the machine and repeat the test with a new cartridge.
Contact an authorized service provider if the problem persists.
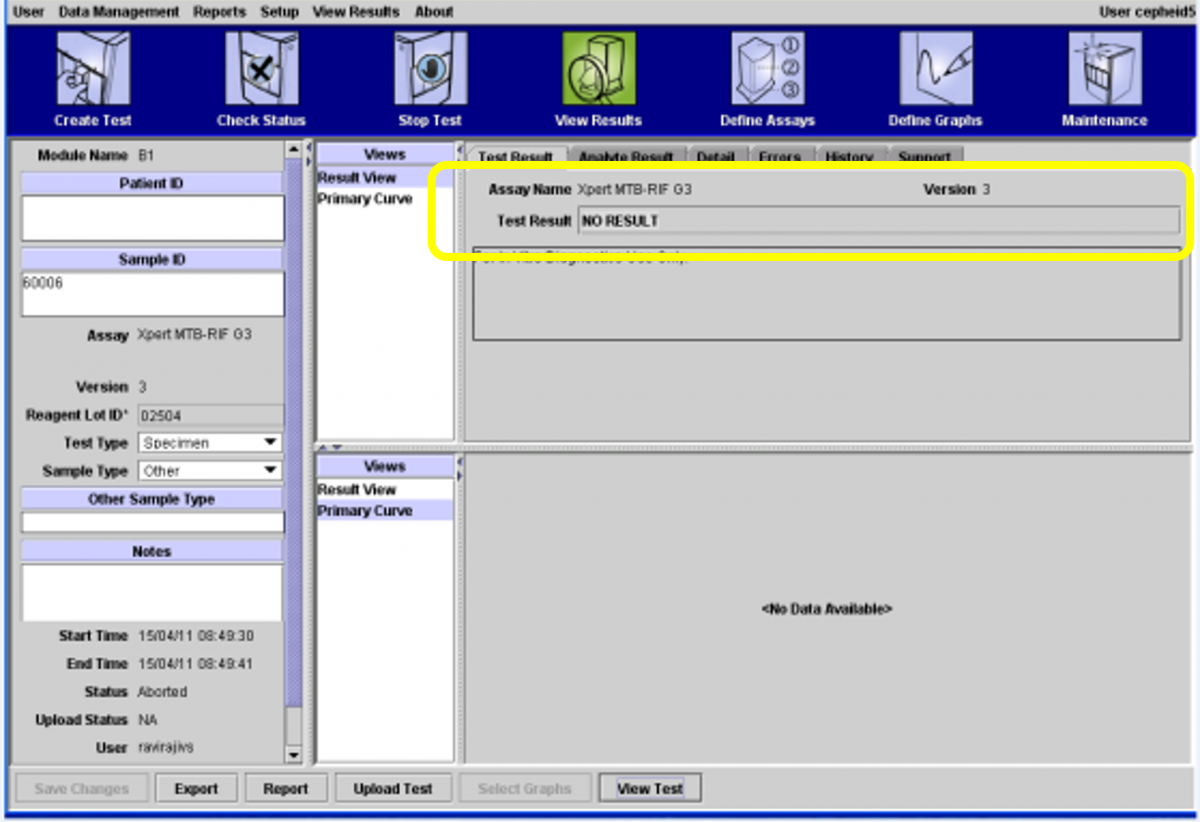
Figure: Error - No Result
Video fileVideo : CBNAAT Troubleshooting: Failures without Error Codes
Resources
Interfering Substances causing errors in NAAT Assay
ContentIt is common in laboratories to see specimens with the following particles which may potentially alter nucleic acid amplification test (NAAT) results:
- Food particles
- Blood
- Tobacco
- Pan
- Debris or tissue pieces
These interfering substances cause failures in Truenat assays and may have inhibitory effects on CBNAAT assays. This interferes with the accuracy of results, leading to false positive or negative tests and delayed cycle threshold values.
Hence, it is important to follow certain precautions when collecting the specimen to avoid contaminating the specimen with these substances.
In such situations, the following protocol needs to be followed:
- Reject frank blood/bloody samples; however, the presence of blood up until 30% does not interfere in Truenat assays
- For samples containing food/tobacco/tissue particles that cause interference in processing:
- Use a fresh sample, if available
- Use a sample after food particles or tissue pieces settle/sediment; otherwise, reject the sample

Figure: Blood in Sputum Sample Interferes with PCR
Resources
-
STLS: Maintenance of CBNAAT
FullscreenMaintenance of CBNAAT Instrument under NTEP
ContentMaintenance of the CBNAAT instrument is an essential activity to be performed in the laboratory setting and involves:
Preventive Maintenance Tasks
- Performed regularly by the user
- Ensure the good performance of the system
- Avoid problems of malfunction
Need-based Maintenance Tasks
- Performed in specific situations
- Performed or guided by manufacturer representatives
Frequency-based Tasks for the CBNAAT Instrument
DAILY WEEKLY MONTHLY ANNUAL OR AFTER 2000 TESTS PER MODULE - Remove and properly dispose off cartridges
- Clean and disinfect the work area
- Put on a dust cover when the instrument is not in use
- Disinfect the instrument’s surface
- Disinfect cartridge bay interior and plunger rod
- Filter cleaning
- Disinfect cartridge bay interior and plunger rod
- Clean instrument filter
- Archive and back-up test results
- Filter cleaning
Module Xpert Check (calibration) and maintenance of the module
Materials Required for CBNAAT Instrument Maintenance
- Freshly prepared 1% sodium hypochlorite solution
- 70% Ethanol
- Wipes, tissues, or cotton
- Disposable gloves
- Clean water and soap (for washing the filters)
- Replacement filters for the fan (available from the manufacturer).
Resources
CBNAAT Instrument Installation Criteria
ContentIt is important to adhere to the manufacturer's installation guide for optimal performance of the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) machine. This guide should be kept in the laboratory. It is important to thoroughly read the instalment steps given in the brochure supplied with the machine.
Strict monitoring of these criteria should be carried out by the laboratory personnel:
- The instrument should not be kept directly under an air-conditioning vent or window. Direct sunlight should also be avoided.
- The instrument's room should have temperature control (15-30°C).
- The instrument needs to be installed on a vibration free/ stable workbench with no centrifuge adjacent to it.
- There is a need for a stable electricity supply (for added safety, the instrument must be connected to an Uninterruptible Power Supply (UPS) or surge protector).
For safety purposes, one needs to provide 10 - 15 cm of clearance on each side of the instrument.
Compliance with equipment installation criteria is necessary. The Instrument Qualification Documents include:
- Installation Qualification - IQ
- Operational Qualification - OQ
- Performance Qualification - PQ
Installation Qualification
IQ provides evidence for the delivery, installation and configuration of the instrument as per the manufacturer’s standards using an installation checklist.
Operational Qualification
OQ is a collection of test cases used to verify the proper functioning of a system before the instrument is released for use.
Performance Qualification
PQ is a collection of test cases used to verify that the system performs as expected under simulated real-world conditions.
Video fileVideo : CBNAAT Instrument Installation Criteria
Resources
Daily Maintenance of the CBNAAT Instrument
ContentDaily maintenance tasks of the CBNAAT instrument include:
At the end of the day:
- Turn off the computer
- Turn off the CBNAAT instrument
At the beginning of the day:
- Turn on the CBNAAT instrument
- Turn on the computer
Daily Maintenance Tasks
- After testing, remove the cartridges from the instrument.
- Dispose off cartridges in the appropriate biohazard waste container.
- Remove clutter from the work area.
- Disinfect the work area (1% hypochlorite solution or 70% ethanol).
- Put on the dust cover when the instrument is not in use.
- Switch off the machine at the end of the day.
- Do not turn off the UPS power supply.
It is essential to wear disposable gloves for the cleaning procedure. Wearing gloves prevents one from being exposed to biologically hazardous samples.
Video fileVideo : Daily Maintenance of CBNAAT Instrument
Resources
Monthly Maintenance of the CBNAAT Instrument
ContentMonthly maintenance tasks of the CBNAAT instrument include:
Cleaning of the Cartridge Bay and Plunger Rod
The CBNAAT manufacturer recommends monthly cleaning of the cartridge bay and plunger rod. However, if the sample load is high, this task can be carried out on a weekly basis.
Cleaning of Module PCR Slot (Figure 1)
- Wear laboratory gloves.
- Remove cartridges from the modules.
- Make sure that all the bristles are fully inserted (up to the shoulder of the plastic shank of the brush).
- Brush the inside of the slot with up and down movements.
- Rotate the brush for approx. 180º and back, then repeat the previous step 2 times.
- Clean each module for at least 30 seconds.

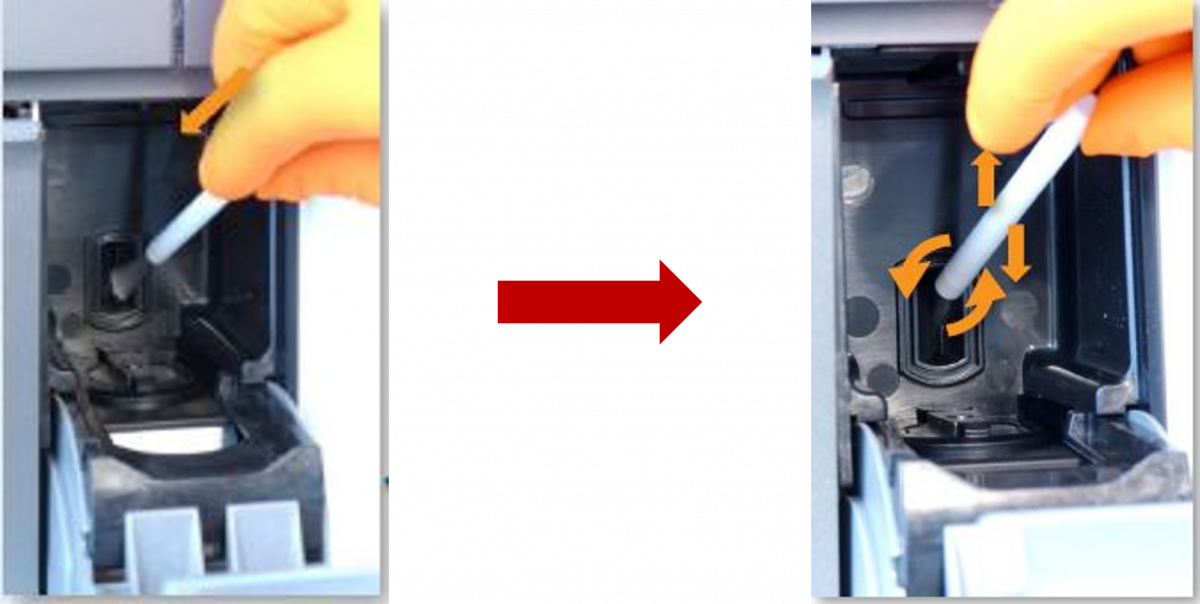
Figure 1: Cleaning of Module PCR Slot
Plunger Disinfection (Figure 2-7)
Plunger maintenance is initiated using the CBNAAT software. While cleaning, care should be taken not to touch the slit on the I-CORE module into which the cartridge reaction tube is inserted. Make sure that the cleaning cloth is damp but not dripping with disinfecting liquid.
1. To initiate the task, click on the “Maintenance” icon on the toolbar (Figure 2).

Figure 2: "Maintenance" icon on the toolbar
2. On the Maintenance menu, select “Plunger Maintenance” (Figure 3).

Figure 3: "Plunger Maintenance" in the Maintenance Menu

3. In the “Plunger Maintenance” window, select a module to clean or select “Clean All” (Figure 4).
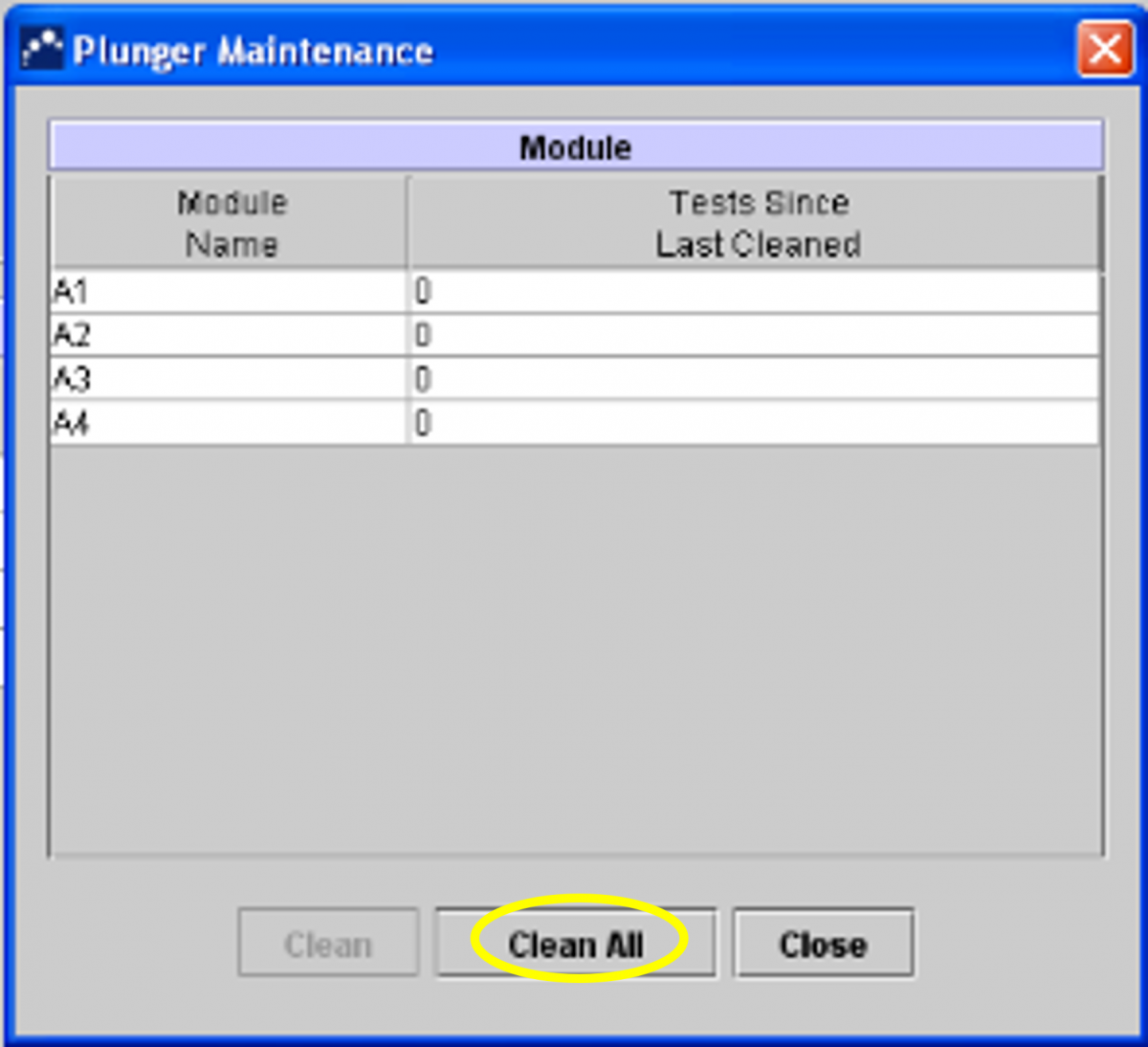
Figure 4: Selecting "Clean All" in the Plunger Maintenance Window
4. Follow the instructions in the Dialog box.
5. Click “OK” (Figure 5).
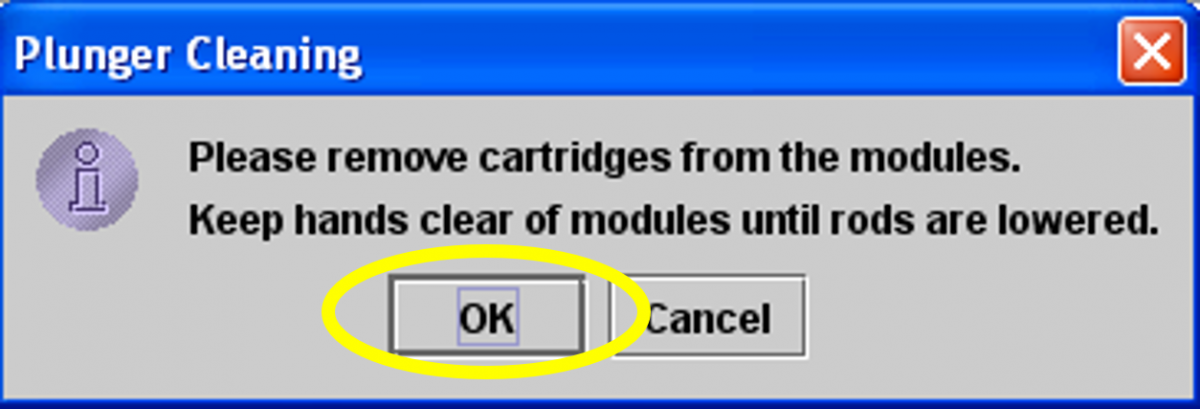
Figure 5: Click "OK" after following instructions in dialog box
6. The plunger rod in the chosen module will be automatically lowered (Figure 6).

Figure 6: Plunger Rod of Module
7. After cleaning the plungers, click on “Move Up All” and the plungers will return to their original position (Figure 7).
8. Click “Close”.

Figure 7: Click "Move Up All" and then "Close" after cleaning the plungers
Replacing and Cleaning the Fan Filters (Figure 8)
Clean the fan filters weekly if you operate in an area of high pollution, dust or smoke, otherwise monthly/ quarterly is sufficient.
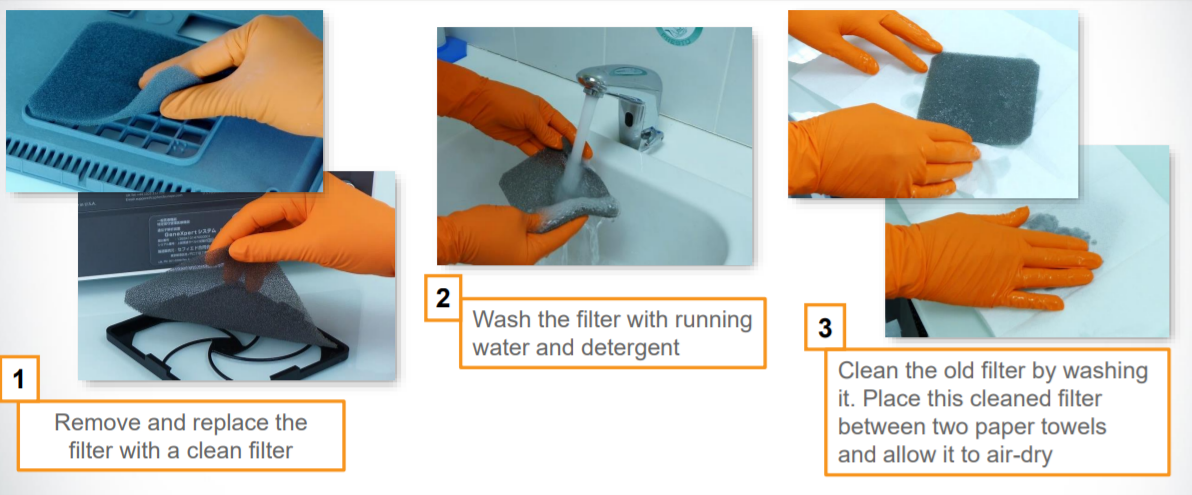
Figure 8: Steps for removing and replacing the filters
General Cleaning Procedure Outline


Make sure you wear disposable gloves for the cleaning procedure. Wearing gloves prevents you from being exposed to biologically hazardous samples.
Items required for cleaning:
- 1% Sodium hypochlorite solution (prepared within one day)
- 70% Ethanol
- Cotton swabs
- Disposable gloves
- Optical brush
Note: The current guidelines from the manufacturer suggest the use of freshly prepared 1% sodium hypochlorite (or 1:10 solution of household chlorine bleach).
- Dampen wipe/ swab with freshly prepared 1% sodium hypochlorite.
- Wipe the surface/ element.
- Discard the used wipe/ swab.
- Wait for 2 minutes.
- Dampen wipe/ swab with 70% Ethanol.
- Wipe the surface/ element.
- Repeat steps 5-7 three times.
Video fileVideo : Monthly Maintenance of the CBNAAT Instrument
Resources
CBNAAT Monthly Data Archive and Data Back-up Process
ContentThe Cartridge-based Nucleic Acid Amplification Test (CBNAAT) files should be archived and saved to a CD or other appropriate external media (preferably an external drive), at least once a month to ensure that no test data are lost.
Archiving tests creates copies of the test data in “gxx” files.
Importance of Archiving and Back-up
Archiving allows you to:
1. Back-up data to ensure it will not be lost if the computer breaks down.
2. Create a copy of the data to be sent to the manufacturer for assistance in troubleshooting problems.
How to Archive Results
1. Click “Data Management” (Figure 1).
2. Click on “Archive Test” (Figure 1).
3. Choose the tests that need to be archived (or “Select All”) (Figure 1).
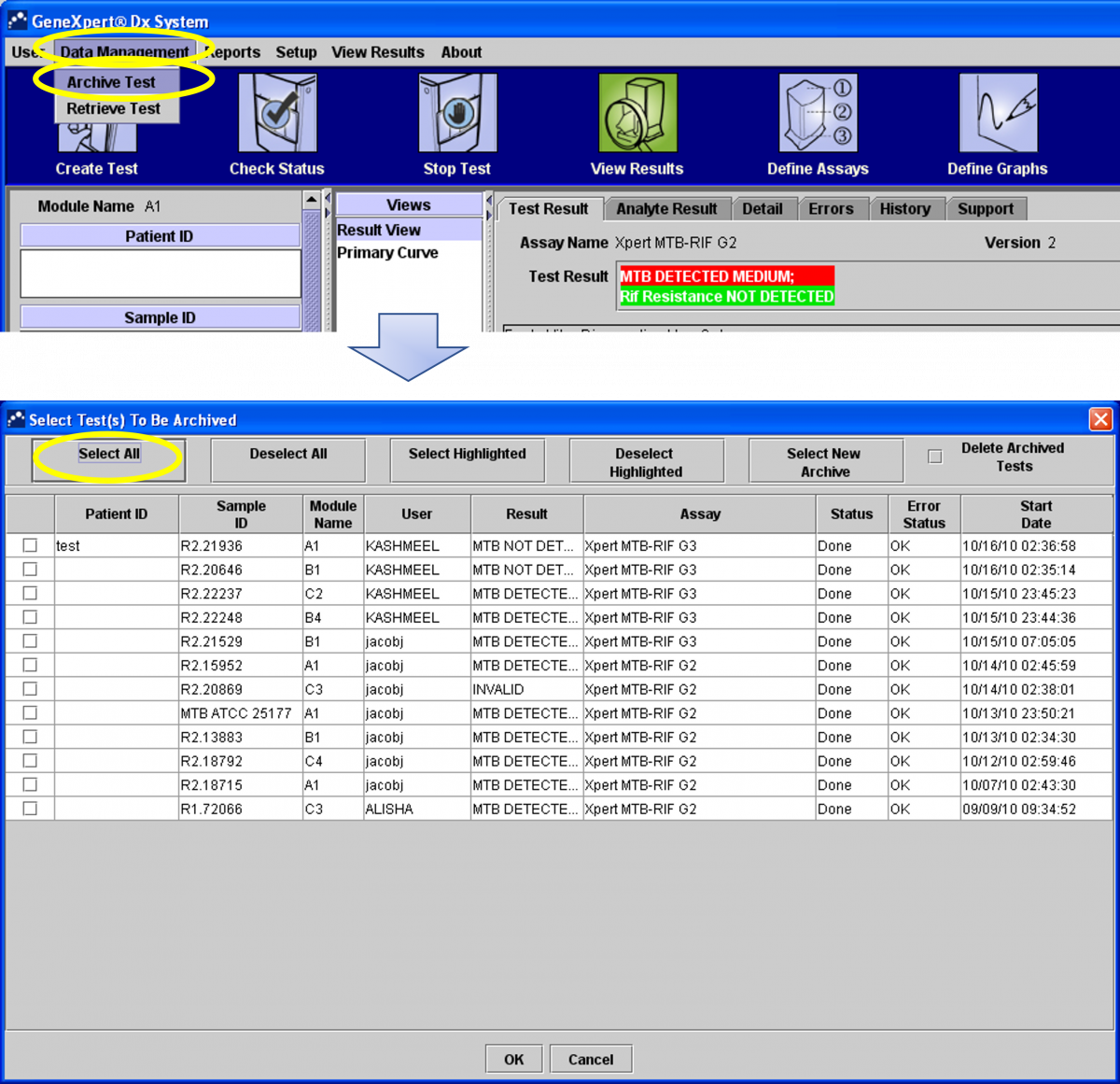
Figure 1: Steps to archive results
4. In the next dialogue box click “Proceed” (Figure 2).
5. The files will be saved in the folder “Export”. In the file name, you will see the date of archiving (Figure 2).
6. Click on “Save” (Figure 2).
7. Click “OK” (Figure 2).
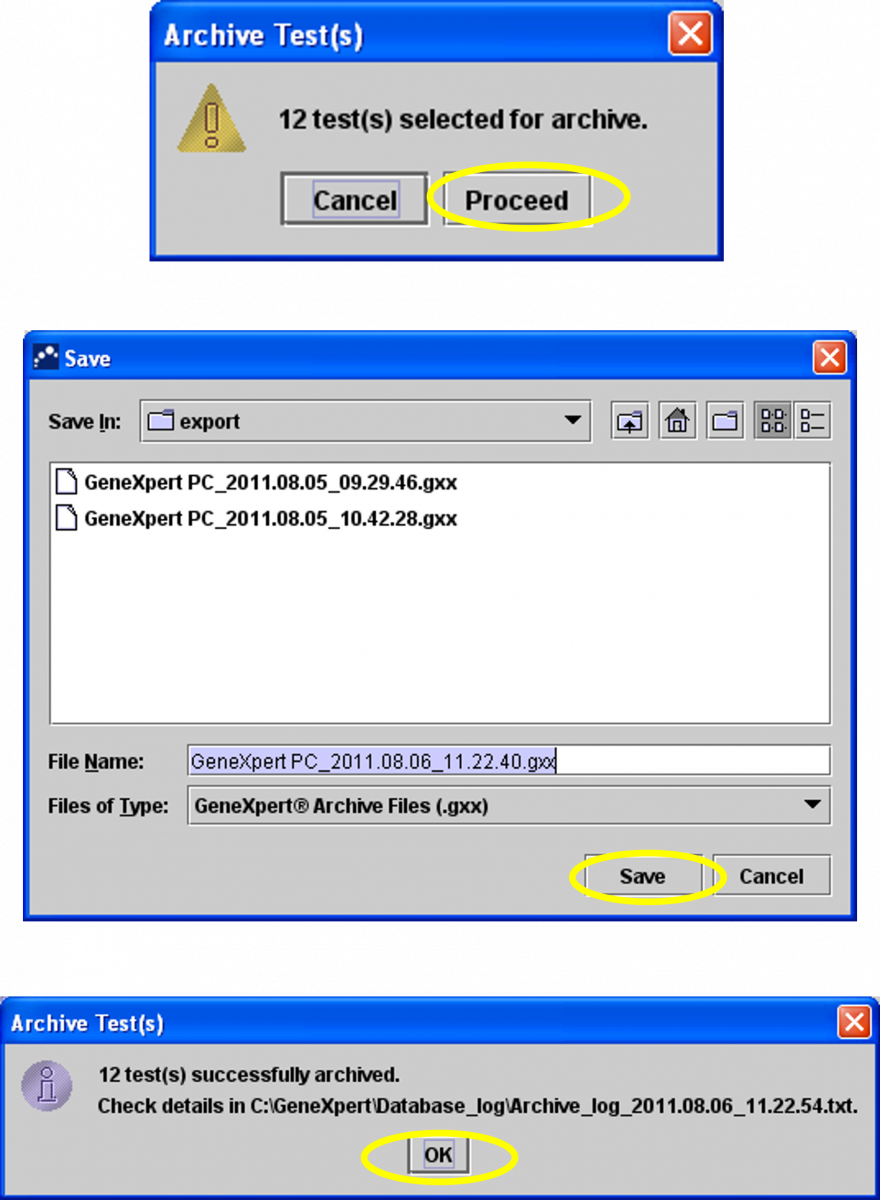
Figure 2: Steps to archive results (continued)
How to Retrieve Results
1. Click “Data Management” and then click “Retrieve Test” (Figure 3).
2. Select the file you want to retrieve.
3. Click on” Open” (Figure 3).
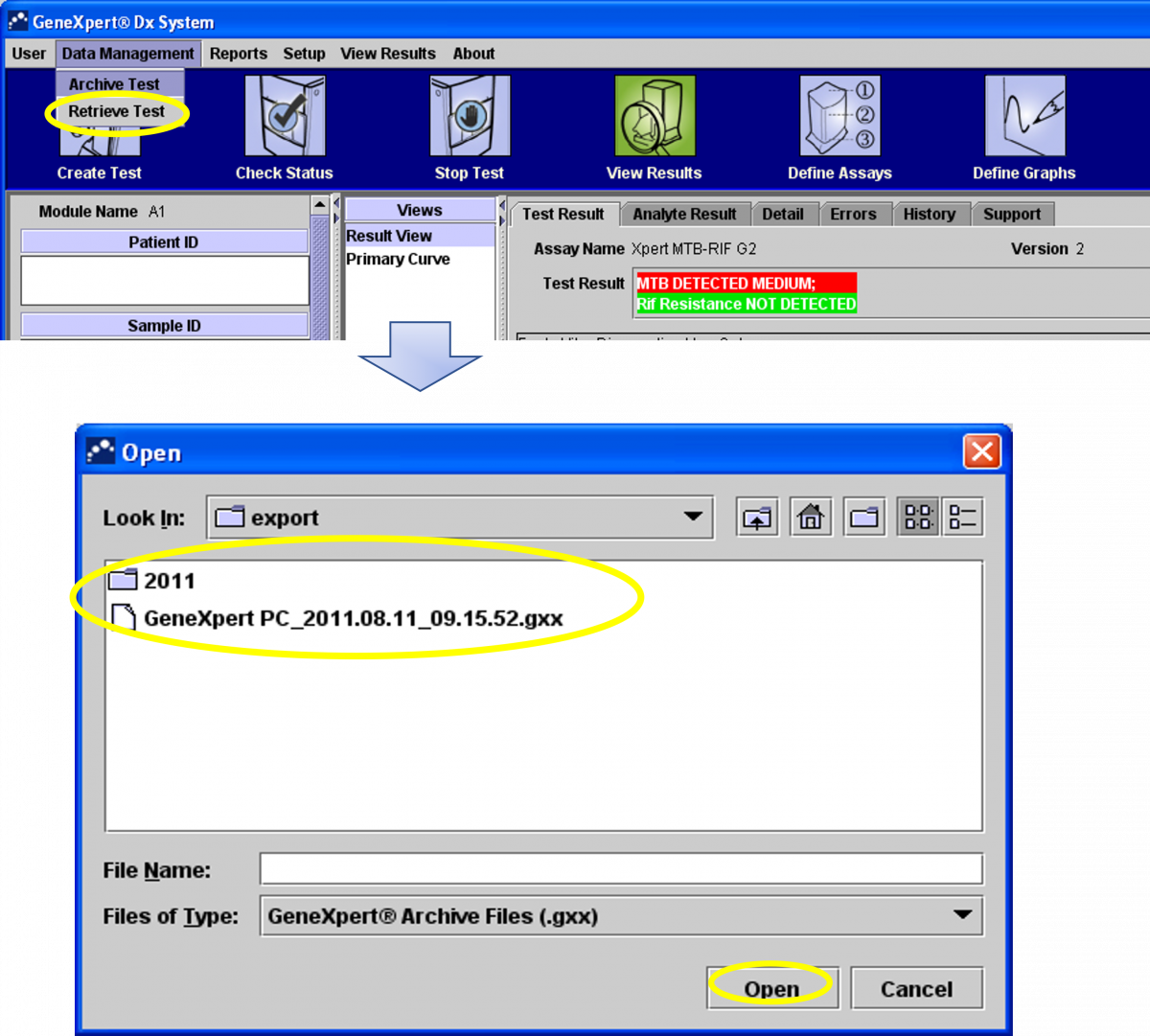
Figure 3: Steps to retrieve results
4. Select the test you may want to retrieve (or “Select All”) (Figure 4).
5. Click “OK” (Figure 4).
6. Click on “Proceed” (Figure 4).
7. Click “OK” (Figure 4).
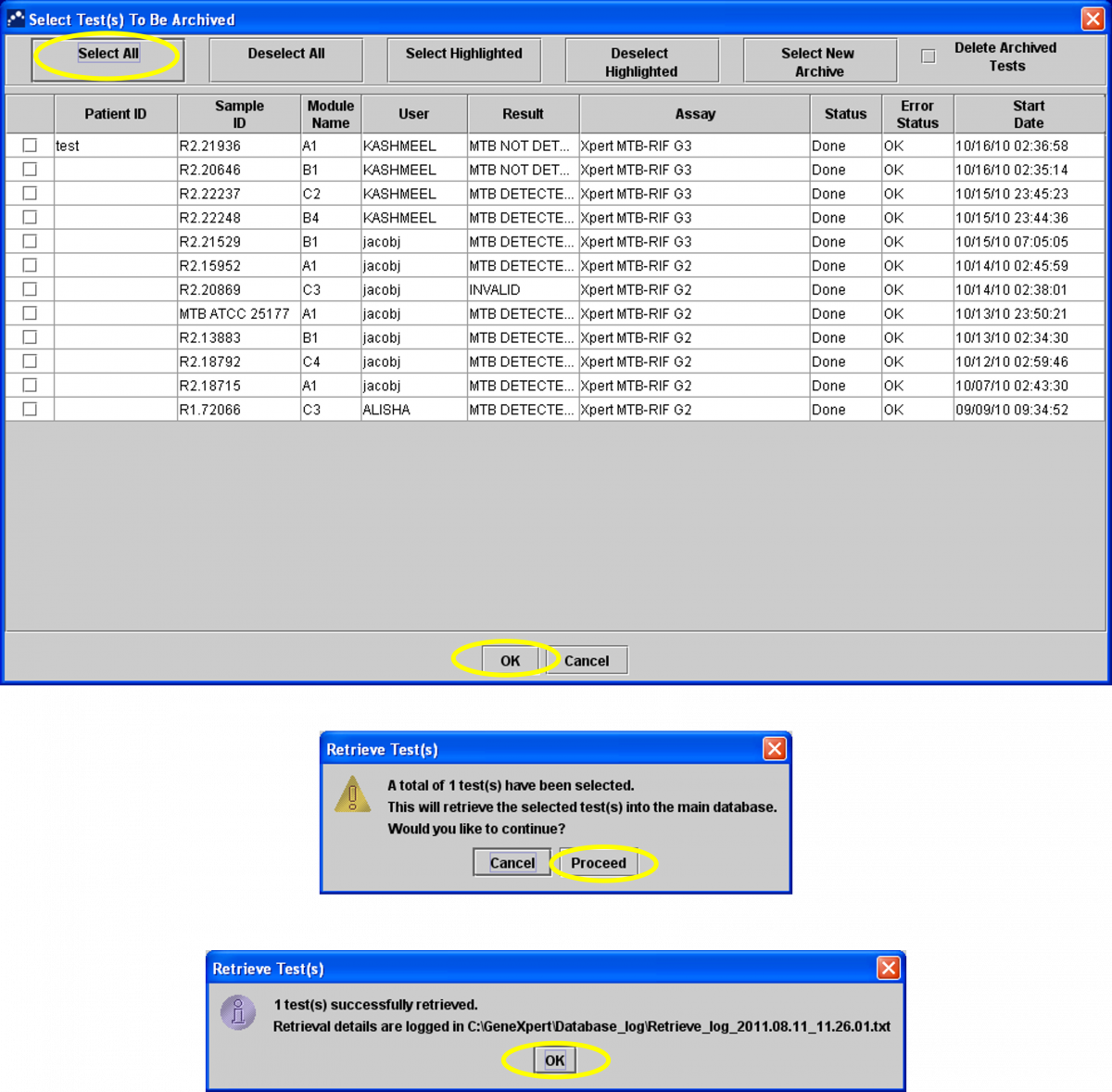
Figure 4: Steps to retrieve results (continued)
How to Back-up Data
Data backup should be carried out monthly.
1. Click “Yes” to the prompt (Figure 5).
2. Click on “Database Backup” (Figure 5).
3. Click on “Proceed” (Figure 5).
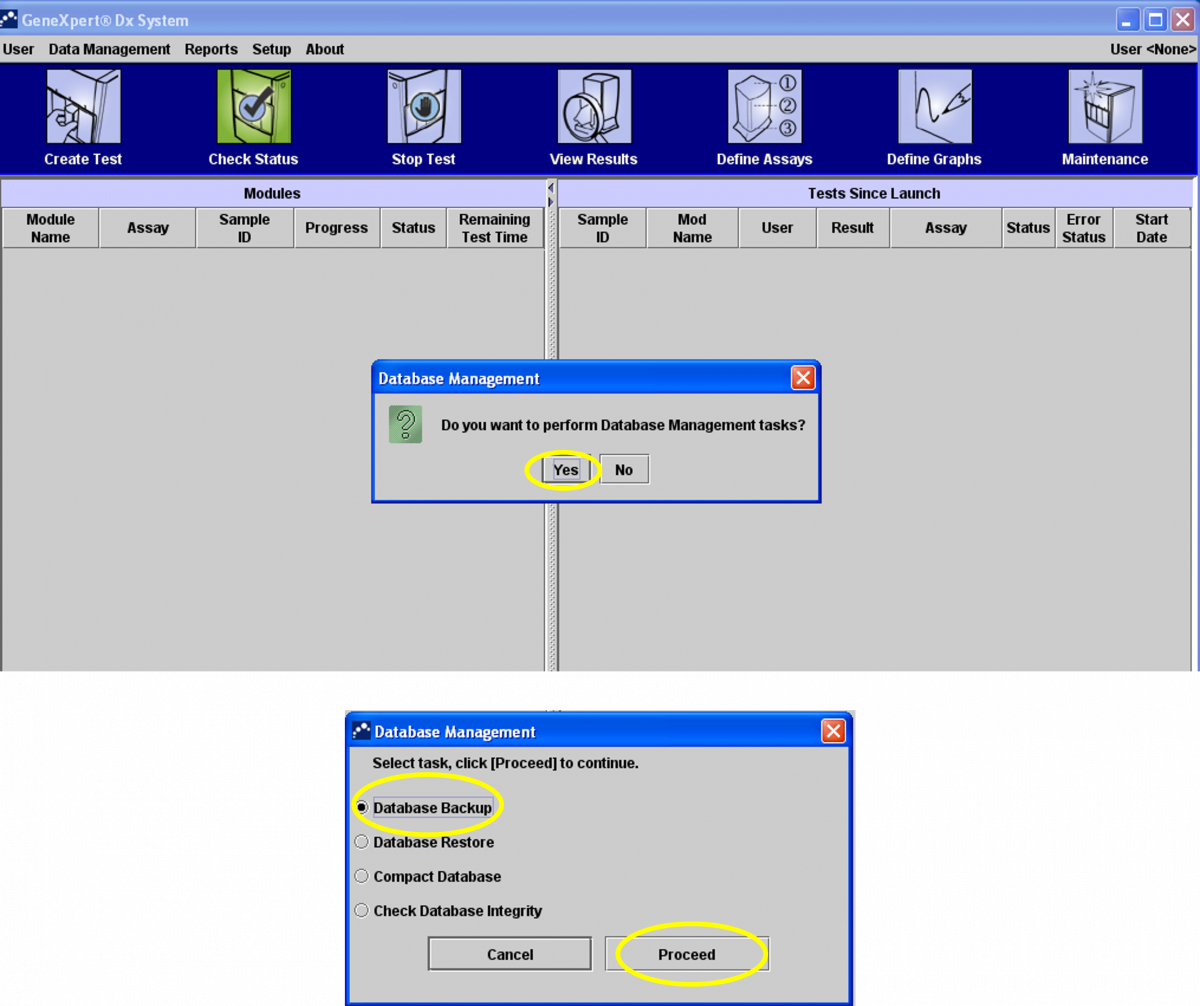
Figure 5: Steps to back-up data

4. The software will create a zip file with all the results (Figure 6).

Figure 6: Software creates a zip file for all results

5. The file is saved on the desktop in the CBNAAT folder -> Backup section.
6. Click on “Save” (Figure 7).
7. Click “OK” (Figure 7).
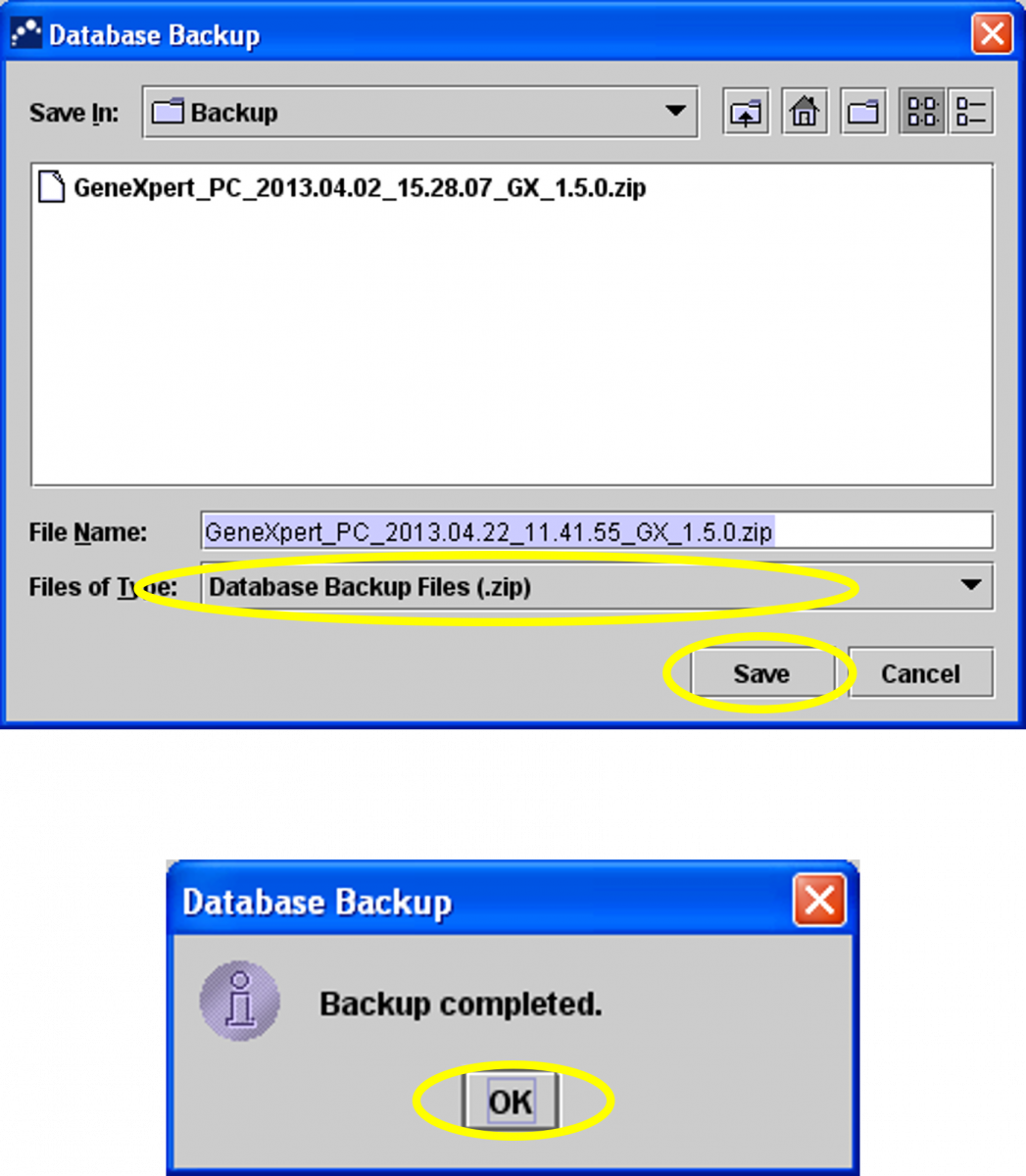
Figure 7: Steps to back-up data (continued)
Video file
Video : CBNAAT Monthly Data Archive and Data Back-up Process
Resources
CBNAAT Annual Maintenance Protocol
ContentThe annual maintenance protocol for the Cartridge-based Nucleic Acid Amplification Test (CBNAAT) instrument involves calibration of the machine.
Calibration:
- Calibration of the CBNAAT instrument is performed by the manufacturer before the system is shipped.
- Calibration is not required during the initial system setup.
- The manufacturer recommends that the system should be checked for proper calibration on an annual basis (or after every 2,000 runs on each instrument module).
- Based on the usage and care of the system, calibration checks may be recommended more frequently.
- The service engineer will perform the machine check during the annual maintenance visit.
Parameters Verified During Calibration
One calibration cartridge is used to calibrate a single module in conjunction with the calibration software.
- Recalibrate the optical system
- Verify the thermal system
- Module sub-system functionality: A series of system-level tests to ensure full system functionality within the instrument servicing specifications as provided by the manufacturer, and covers:
- Heater and fan performance
- Syringe drive and pressure performance
- Valve drive performance
- Ultrasonic horn performance
- Electronic components performance
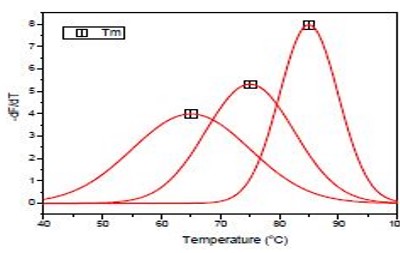
Figure: Temperature Calibration of the CBNAAT Instrument
Resources
-
-
STLS: Truenat
Fullscreen-
STLS: Truenat as a Rapid Molecular Diagnostic Test
FullscreenTruenat Cartridge and Inside Demonstration
ContentTruenat cartridges are components of Trueprep AUTO v2 Universal Cartridge Based Sample Prep Kit. As shown in the figure below, each cartridge is:
- Used with Trueprep Device for DNA extraction and purification
- Disposable
- Single-use
- Preloaded with Internal Positive Control.
Truenat cartridges are used with Trueprep devices for DNA extraction and purification. The components of the cartridge are illustrated in the following figure and include:
- Sample Chamber - Processed samples (pretreated with lysis buffer) are added to the sample chamber of the cartridge for processing on the Trueprep device.
- Matrix Chamber - DNA released by chemical and thermal lysis cells binds to the proprietary matrix here.
- Elute Chamber - Trapped DNA is washed with buffers to remove Polymerase Chain Reaction (PCR) inhibitors and is eluted from the matrix using the elution buffer. The purified DNA is collected from here.
- Waste generated is contained within the dump region inside the cartridge.

Figure: Inside of a TrueNAT Cartridge; Source: Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance
Resources
Consumables Required at a Truenat Lab
ContentConsumables required for Truenat test provided by the manufacturer include:
Trueprep AUTO MTB Sample Pre-treatment Pack for sample processing
- Liquefaction buffer
- Lysis buffer
- Disposable transfer pipette (graduated) - 1ml

Trueprep AUTO v2 Universal Cartridge Based Sample Prep Kit for DNA extraction
- The Reagent Pack contains the following reagents
- Wash Buffer A
- Wash Buffer B
- Elution Buffer
- Priming Waste
- The Cartridge Pack contains the following
- Cartridge
- Elute collection tube
- Elute collection tube label
- Disposable transfer pipette
- Disposable Transfer Pipettes (graduated) - 3 ml
- Reagent Reset Card

Truenat MTB Chip-based Real-Time PCR test for Mycobacterium tuberculosis
- Truenat MTB micro-PCR chip
- Microtube with freeze-dried PCR reagents
- DNase & RNase free pipette tip

Truenat MTB-RIF Dx Chip-based Real-Time PCR Test for Rifampicin Resistant Mycobacterium tuberculosis
- Truenat MTB-RIF Dx micro-PCR chip
- Microtube with freeze-dried PCR reagents
- DNase & RNase free pipette tip

Other Consumables
- Gloves
- Masks
- Sodium hypochlorite
Resources
- MolBio Diagnostics Product Details
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance
Kindly provide your valuable feedback on the page to the link provided HERE
Overview of the Truenat Testing Process
ContentThe Truenat Assay Technology works on Real-time Polymerase Chain Reaction (PCR).
The key steps include:
- Collection of specimens from a presumptive TB/known TB Patient (for UDST).
- Liquefaction and lysis of specimen using the Trueprep AUTO MTB sample pre-treatment pack (20 minutes)
- Extraction and purification of DNA using Trueprep AUTO v2 Universal Cartridge-based sample prep kit and Trueprep AUTO v2 Universal Cartridge-based sample prep device (20 minutes)
- Amplification of extracted DNA by the Truelab Real-time micro-PCR analyzer using freeze dry PCR reagent in microtubes on a Truenat MTB chip (35 minutes)
- DNA from positive test results is tested using Truenat MTB RIF Dx chip as a reflex test (55 minutes)
The process flow from sample to result for Truenat Assay Technology is described in the figure below.
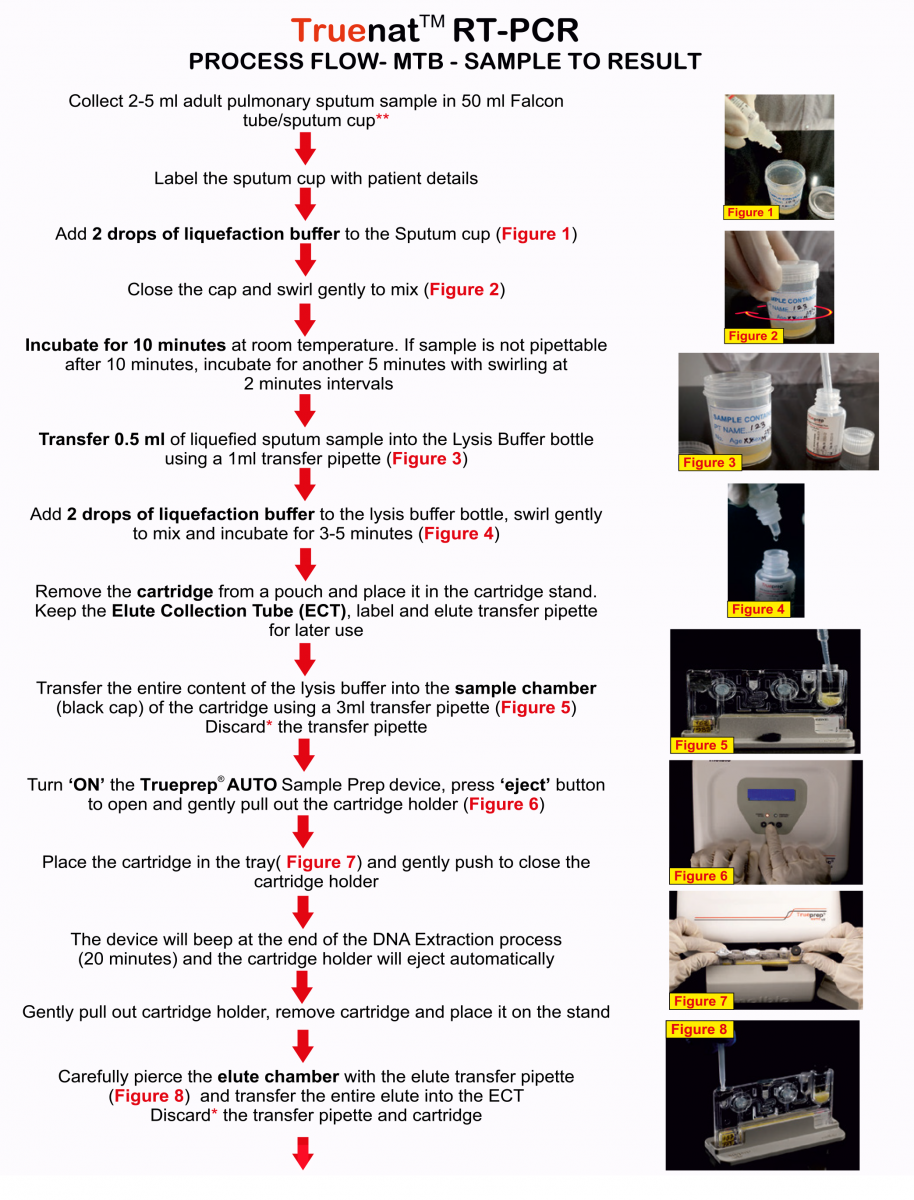
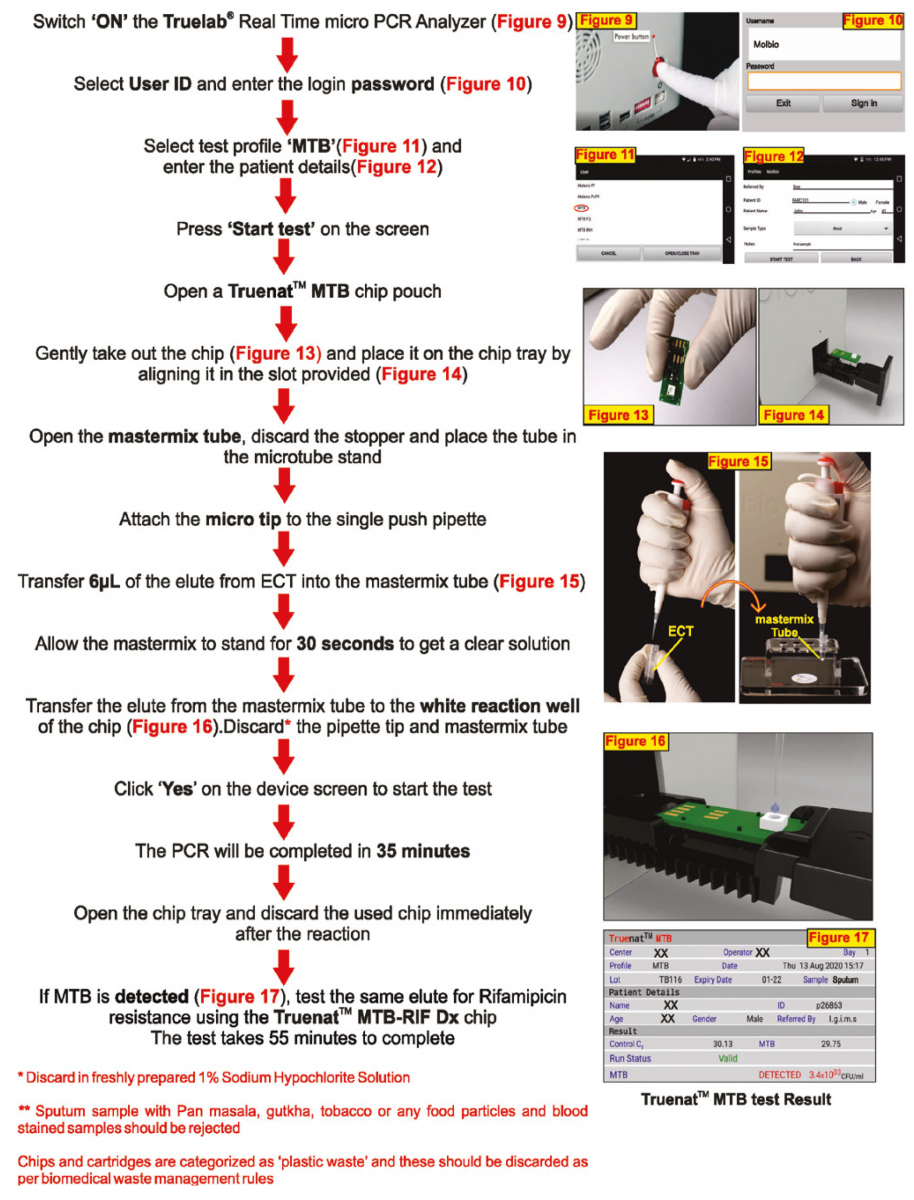
Figure: Process flow from sample to result for Truenat Assay Technology; Source: Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
Resources
- Truenat MTB Kit Insert.
- Trueprep® AUTO Universal Cartridge-based Sample Prep Device.
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
Kindly provide your valuable feedback on the page to the link provided HERE
Truenat MTB and RIF Assay as a TB Diagnostic Test
ContentThe tests are performed using Trueprep AUTO Sample Pre-treatment and Prep kits and Truenat micro-PCR chips.
To detect M. tuberculosis, the Truenat MTB chip amplifies a portion of the ribonucleoside-diphosphate reductase gene, nrdB with a Limit of Detection (LOD) of about 100 Colony Forming Units (CFU)/ml sputum sample.
DNA extraction and detection of M. tuberculosis takes approximately one hour.
When M. tuberculosis is detected, as a follow-on test, a small volume of the already extracted DNA is used to test for resistance to Rif using Truenat MTB Rif Dx chip.
Mutations associated with Rif-resistance within the RRDR region of rpoB gene are detected using a probe melt assay and read using the Truelab micro-PCR Analyzer.
The detection of Rif-resistance takes an additional one hour.
Truenat Testing Capacity
- The Truelab Analyzer is available as 1 (Uno), 2 (Duo) or 4 (Quattro) chip ports (figure below).
- The different ports can be used independently to test multiple samples.
- In an eight-hour daily work shift, the estimated throughput of Truelab Analyzer Uno, Duo or Quattro can be 7-9, 15-18, 30-36 specimens, respectively.
Results Reporting
A Truelab micro PCR printer (figure below) is used to print test results. It can also be connected via SIM card/ Wi-Fi/ Bluetooth to transmit results.

Figure: Different Equipments used in the Truenat Workstation
Resources
- Truenat MTB Pack Insert.
- Truenat MTB Rif Dx Pack Insert.
- Truelab Manual.
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin-resistance.
Kindly provide your valuable feedback on the page to the link provided HERE
Inbuilt Controls used in TrueNAT
ContentTruenat tests use Internal Quality Control to assess test validity using Internal Positive Control (IPC).
- The cartridge contains pre-loaded IPC.
- IPC is part of the full process control.
- IPC undergoes all processing steps along with specimen from extraction to amplification.
- IPC assesses the validity of the test run from sample processing to result and is illustrated in following figures (Figure 1(A) and Figure 1(B)).

Figure 1(A): Amplification of IPC in Valid Test; Source: MolBio Diagnostics Pvt. Ltd.
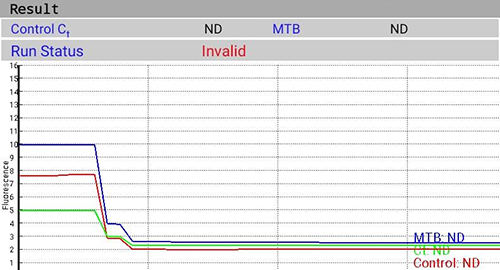
Figure 1(B): Invalid Test with Failure of IPC Amplification; Source: MolBio Diagnostics Pvt. Ltd.
Resources
- Truenat MTB Kit Insert.
- Trueprep AUTO Universal Cartridge Based Sample Prep Device.
- Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Specimen processing for Truenat
FullscreenProcessing of Sputum Sample before Truenat Testing
ContentThe sputum sample needs to be processed to liquefy and lyse the specimen before Truenat testing. This is because of the following reasons:
- Sputum samples contain Polymerase Chain Reaction (PCR) inhibitors but PCR amplification requires pure DNA from sputum samples.
- The sputum sample should be homogenized and pipettable before DNA extraction can begin.
- Pre-treatment also decontaminates specimen for storage/ transportation/ extraction.
The Trueprep AUTO MTB Sample pre-treatment pack is used for processing the specimen. It digests sputum, releases bacteria, and removes PCR inhibitors.
Steps for specimen pre-treatment include:
- Open a Trueprep AUTO MTB sample pre-treatment kit which contains a graduated 1 ml transfer pipette, lysis buffer bottle and liquefaction buffer bottle.
- The sample and all reagents including the liquefaction buffer, lysis buffer should be at room temperature before starting the steps of pre-treatment.
- Switch on the Trueprep AUTO v2 sample prep device.
- Label lysis buffer bottle with corresponding sample number and date of extraction.
- Add 2 drops of liquefaction buffer to the sputum sample, swirl mix, incubate for 10 minutes at room temperature. If the sample is not pipettable after 10 minutes, incubate for another 5 minutes and swirl at 2 minutes intervals.
- Transfer 0.5 ml of the liquefied sputum sample from the sample container to the corresponding lysis buffer bottle using the 1 ml graduated transfer pipette provided.
- Dispose of the used transfer pipette into the container filled with freshly prepared 1% sodium hypochlorite.
- Add 2 drops of liquefaction buffer into the lysis buffer bottle; swirl gently to mix and incubate the lysis buffer bottle at room temperature for 3-5 minutes.
- Ensure that the sample has completely liquefied.
- Sputum may be stored in lysis buffer for up to 1 week at 30°C with no degradation of DNA.
Video fileResources
- Trueprep AUTO MTB Sample Pre-treatment Pack.
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
Kindly provide your valuable feedback on the page to the link provided HERE
DNA Extraction in TrueNAT MTB and TrueNAT MTB/RIF DX Assay
ContentEquipment and Consumables
- Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device
- Trueprep AUTO v2 Universal Cartridge Based Sample Prep Kit
Steps in DNA extraction (Molbio Trueprep Auto Universal Cartridge Based Sample Prep Device)
1. Wear gloves, mask.
2. Insert the plug-in connector to attach the reagent pack to the Trueprep device (Figure 1).

Figure 1: Trueprep Cartridge Based Sample Prep Kit attached to the Trueprep Auto Device using the Plug-in Connector; Source: Practical Guide to Implementation of Truenat Tests for the Detection of TB and Rifampicin Resistance
3. Disinfect the work surfaces with the freshly prepared 1% bleach, followed by 70% alcohol.
4. Open the cartridge pouch, take out the cartridge.
5. Label the cartridge (Patient ID, Date), place it on the cartridge stand.
6. Open the black cap of the cartridge sample chamber.
7. Using a pipette transfer 3 ml contents of the lysis buffer bottle (processing step) in the sample chamber.
8. Discard the pipette and lysis buffer bottle (1% sodium hypochlorite).
9. Re-cap the sample chamber.
10. Press the “Power” button to switch on the Trueprep device.
11. Press “Eject” to eject the cartridge holder (Figure 2), pull out gently.

Figure 2: Top view of the Trueprep AUTO Universal Cartridge-based Sample Prep Device; Source: Practical Guide to Implementation of Truenat Tests for the Detection of TB and Rifampicin Resistance
12. Insert the cartridge in the cartridge holder (sample chamber to the right when seen from the front).
13. Push to close the cartridge holder (the click sound confirms the correct cartridge loading).
14. Press the “Start” button (Figure 2).
15. DNA extraction begins, reagents from bottles are automatically added to the cartridge (pre-programmed) (Figure 2).
16. On completion (18-20 min), the cartridge holder automatically ejects.
17. Remove the cartridge, place it on the cartridge stand.
18. Label the ECT tube (Elute Collection Tube) with Patient ID & Date.
19. Pierce the covering of elute compartment in the cartridge with a filter barrier pipette tip, aspirate elute (DNA) into the ECT tube.
20. Discard the used pipette tips, used cartridge (1% sodium hypochlorite).
21. DNA can be used immediately for amplification/ stored in fridge (4°C for up to 24 hours) or -20°C (for up to 1 year).
Video fileResources
- Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance.
- Operation of Molbio Trueprep AUTO Universal Sample Prep Device.
- Molbio Trueprep Auto Universal Cartridge-based Sample Prep Device.
Kindly provide your valuable feedback on the page to the link provided HERE
PCR Amplification of the Target genes in Truenat
ContentTruenat Mycobacterium tuberculosis (MTB) and Truenat MTB Rifampicin (Rif) Dx Assays amplify target genes through Polymerase Chain Reaction (PCR).
The presence of mutant gene is detected using probe melt assay.
The target genes include:
- Truenat MTB - ribonucleoside-diphosphate reductase gene nrdZ (the precursor for DNA synthesis)
- Truenat MTB Rif Dx assay – Rifampicin Resistance Determining Region (RRDR) region of the RNA polymerase Beta (rpoB) gene for resistance to Rif (between codon positions 509 and 533)

Figure: Image showing RRDR of the rpoB gene of M. tuberculosis; the target gene of Truenat MTB Rif Dx assay includes codons 509-533
Resources
- Truenat MTB Pack Insert.
- Truenat MTB Rif Pack Insert.
- Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance.
Kindly provide your valuable feedback on the page to the link provided HERE
Loading the sample into Truenat Cartridge
ContentVideo fileTrueNAT Sample Processing: Other Body Fluids
ContentThe extra-pulmonary samples (Non-sputum) can also be processed and used for MTB and Rif diagnosis using Truenat. The processing of various extra-pulmonary samples is described below.
Reagents required:
Trueprep AUTO MTB Sample Pre-treatment Pack for sample processing
- Reagents stable for two years (2-40°C) or one month (temperatures up to 45°C)
- Avoid exposure to light or elevated temperatures
- Do not freeze
Steps in processing of non-sputum samples
Non-sputum samples like tissue biopsy should not be processed at the Designated Microscopy Centre (DMC), but should be transferred to a higher centre.
General Instructions
- Disinfect work surfaces with freshly prepared 1% bleach, followed by 70% alcohol.
- Process fresh specimens immediately or store frozen at -20oC. Avoid more than three freeze thaws.
- Bring frozen samples and refrigerated reagents to room temperature (20-30°C).
- Open the Trueprep AUTO MTB sample pre-treatment pack that contains:
- Liquefaction buffer bottle
- Lysis buffer bottle
- Graduated 1 ml transfer pipette.
- Processing is to be done as instructed for each sample type.
- Non-sputum sample is stable for 3 days at up to 40°C and 1 week at 30°C in the lysis buffer.
A. Processing for Bronchoalveolar Lavage (BAL), Pleural fluid, Peritoneal fluid
Equipment: Centrifuge and centrifuge tubes (10-15 ml volume)
- Add 5-10 ml specimen in a centrifuge tube.
- Centrifuge at 4000x for 5 minutes to concentrate the sample.
- Discard the supernatant until 500 μl remains.
- Add two drops of the liquefaction buffer to the concentrated sample (500 μl).
- Transfer the contents to a labelled lysis buffer tube.
- Incubate for five minutes and proceed for DNA extraction.
B. Processing for Pus, Abscess, Lymph node aspirate, Cerebrospinal Fluid (CSF)
Equipment: Centrifuge tubes (1.5 ml volume)
- Add 0.5 ml specimen in a 1.5 ml tube.
- Add two drops of liquefaction buffer.
- Transfer the contents to a labelled lysis buffer tube.
- Incubate for 5 minutes and proceed for DNA extraction.
C. Processing for Tissue/ Biopsy Samples
Equipment: Mortar and pestle (for tissue homogenization)
- Homogenize sample by using 100 μl lysis buffer in mortar and pestle.
- Add two drops of liquefaction buffer.
- Transfer the contents to a labelled lysis buffer tube.
- Incubate for five minutes.
- Use only clear fluid for DNA extraction.
The processed samples will be used for DNA extraction and PCR amplification for diagnosis of MTB and Rif resistance.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Using Truenat autoanalyzer for MTB testing
ContentVideo fileUnloading the Truenat Cartridge
ContentVideo fileLoading the elute onto the Truenat MTB Chip
ContentVideo fileRetrieving test results from the Truenat machine
ContentVideo fileRecording Truenat Results
ContentVideo file
-
STLS: Truenat result Interpretation and recording
FullscreenTruenat MTB Assay Results Interpretation: Visualization
ContentTruenat MTB Assay results are visualized:
- During testing
- Completion of test
Test Status Screen (Figure 1)
Results visualization during testing include:
- “Green” Test Progress Bar helps to monitor the test progress and the current cycle number.
- “Yellow” Cycle Progress Bar indicates the progress of the current cycle.
- Test Details Bar indicates patient details, sample type, system health, battery level, current cycle temperature.
- “Red” Test Completion Indicator turns green when the test completes.
- PLOT button displays optical (fluorescence measure) and thermal graphs (temperature during PCR) on real time basis.

Figure 1: Test Status Screen; Source: TrueLab Manual
Test Result Screen (Figure 2(A)-(E))
On tapping the "Result" button, results visualization on the completion of test includes:
- Input details display; Patient details - Name, ID, Age, Sex, Referred by
- Chip details display; Type of Chip - Truenat MTB/ Truenat MTB Rif
- Test results of Truenat MTB:
- DETECTED
- NOT DETECTED
- Error
- Test results Truenat MTB-Rif Dx:
- Rif Resistance Detected
- Rif Resistance Not Detected
- Indeterminate
- Error
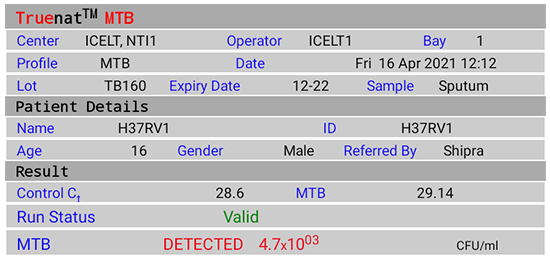
Figure 2(A): Truenat MTB Test Result Screen; DETECTED; Source: MolBio Diagnostics Pvt. Ltd.
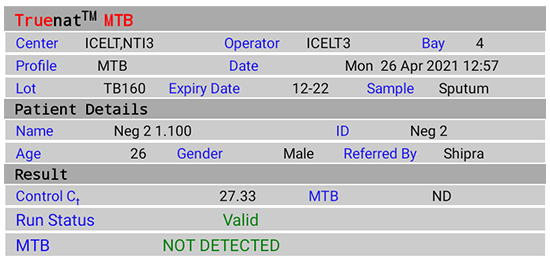
Figure 2(B): Truenat MTB Test Result Screen; NOT DETECTED; Source: MolBio Diagnostics Pvt. Ltd.

Figure 2(C): Truenat MTB Rif Test Result Screen; Rif Resistance Detected; Source: MolBio Diagnostics Pvt. Ltd.
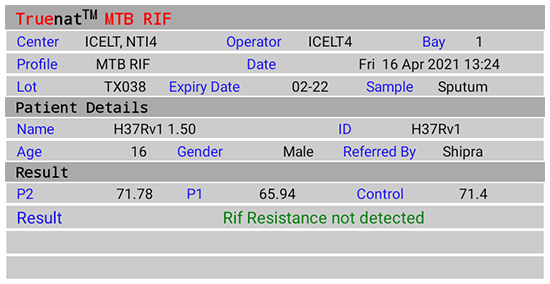
Figure 2(D): Truenat MTB Rif Test Result Screen; Rif Resistance Not Detected; Source: MolBio Diagnostics Pvt. Ltd.

Figure 2(E): Truenat MTB Rif Test Result Screen; Indeterminate; Source: MolBio Diagnostics Pvt. Ltd.
Video fileResources
Kindly provide your valuable feedback on the page to the link provided HERE
TrueNAT MTB Assay Results Interpretation: Detection of Mycobacterium tuberculosis and RIF Resistance
ContentOn completion of test run, the Test Result Screen displays the results for:
- Detection of Mycobacterium tuberculosis (Truenat MTB)
- “DETECTED” for Positive result, Cycle Threshold (Ct) value, Colony Forming Units per milliliter (CFU/ ml)
- “NOT DETECTED” for Negative result
- “Valid”/ “Invalid” for test validity based on amplification of Internal Positive Control (IPC)
- “Error” for test failure
- Detection of Rif Resistance (Truenat MTB-Rif Dx)
- “Rif Resistance Detected” if mutations to Rif are detected
- “Rif Resistance Not Detected” if mutations to Rif are not detected
- “Indeterminate” when test did not determine resistance to Rif
- “Error” for test failure
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
- Detection of Mycobacterium tuberculosis (Truenat MTB)
Amplification and Detection of MTB and MTB-Rif
ContentProcedure
Equipment and reagents
- Truelab Uno/ Duo/ Quattro Real Time Quantitative micro–PCR analyzer
- Truenat MTB micro-PCR kit
- Truenat MTB Rif micro-PCR kit
- Truepet fixed volume (6 μl) precision micropipette
Amplification and detection of Mycobacterium tuberculosis (MTB)
- Wear gloves, laboratory coats, mask.
- Clean working surfaces with 1% Sodium hypochlorite, followed by 70% alcohol.
- Clean instruments with a paper towel dipped in 70% alcohol.
- Switch on the Truelab device by pressing the red button for two seconds.
- Select test bay.
- Select test profile: “MTB”, enter Details (Referred By, Patient ID, Gender, Patient Name, Age).
- Select the sample type.
- Press “Start Reaction". For Truelab Uno Dx, Press the eject button to open the chip tray. For Truelab Duo/Quattro, the chip tray opens automatically on tapping the “Start Reaction” .
- Take out “Truenat MTB chip” from the chip sleeve (check desiccant colour. If blue -chip can be used; discard chip if desiccant is pink/ white which indicates moisture is absorbed).
- Place the chip on the tray by aligning the registration holes with tray pins without touching the white reaction well. (the white reaction well should face upward).
- Open the microtube containing the freeze-dried PCR reagent (white colour) and place it on the microtube stand.
- Pipette 6 μl DNA from the Extraction Chamber (After DNA extraction and purification step) into the microtube.
- Wait 30-60 seconds for the DNA elute and PCR reagent to mix (clear solution obtained).
- Use the same tip to pipette 6 μl treated DNA from the microtube and load on the white reaction well of the chip.
- Discard the microtube and microtip (1% sodium hypochlorite).
- Start the test run.
- The test completes in 35 minutes, press ‘’RESULT’’ to view the result screen.
- Possible results:
- MTB Detected/ Not Detected/ Errors/ Invalid
- If MTB detected, test the same DNA eluate for Rif resistance using MTB-Rif chip. Select the MTB-Rif assay.
- If the result is Invalid/ Error, repeat amplification using the same extracted DNA and a new “Truenat MTB chip”. If Invalid again, repeat the test with a fresh sample.
- Tap “Open/ Close Tray” button to eject the chip tray.
- Lift the chip and discard (1% sodium hypochlorite).
Amplification and Detection of MTB Rif
- DNA from the MTB positive elutes is tested for Rif-resistance using the MTB-Rif chip.
- Select the test profile “MTB Rif”.
- Select the sample type.
- Press “Start Reaction". For Truelab Uno Dx, Press the eject button to open the chip tray. For Truelab Duo/Quattro, the chip tray opens automatically on tapping the “Start Reaction”.
- Take out “Truenat MTB Rif Dx chip” from the chip sleeve (check desiccant colour. If blue -chip can be used; discard chip if desiccant is pink/ white which indicates moisture is absorbed).
- Follow steps 10-16 as described in Amplification and detection of MTB (above).
- The test completes in 55 minutes, press ‘’RESULT’’ to view the result screen.
- Possible results:
- MTB Rif resistance detected/ MTB Rif resistance not detected/ Error/ Indeterminate.
- If result is Indeterminate/ Error, repeat the amplification using the same extracted DNA and new “Truenat MTB Rif Dx chip”. If Indeterminate/ Error again, repeat the test with a fresh sample.
- Tap “Open/ Close Tray” button to eject the chip tray.
- Lift the chip and discard (1% sodium hypochlorite).
The algorithm for Truenat MTB Assay (Figure) describes interpretation of test results obtained for Truenat MTB and Truenat MTB Rif Dx assays.
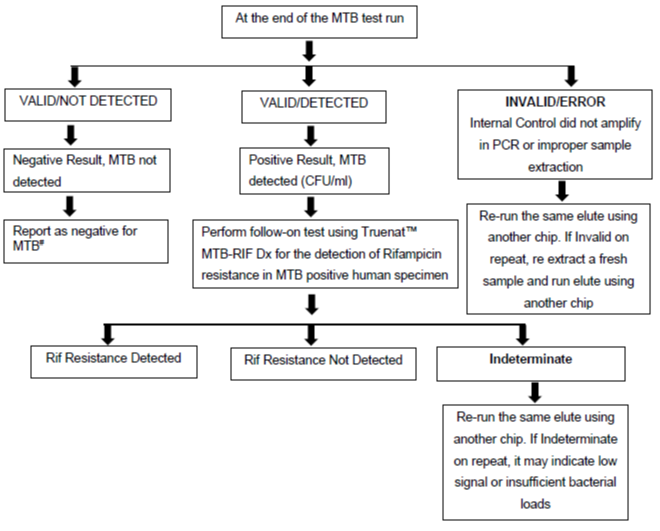
Figure: Truenat MTB Assay Results Interpretation: Algorithm; Source: Practical Guide to Implementation of Truenat Tests for the Detection of TB and Rifampicin Resistance
# Test is Valid as Internal Positive Control amplified
Video fileResources
- Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance.
- Truenat MTB Pack Insert.
- Truenat MTB Rif Pack Insert.
Kindly provide your valuable feedback on the page to the link provided HERE
Results Entry in Lab Register for NAAT
ContentThe results for Nucleic Acid Amplification Test (NAAT) assays are entered in Culture and Drug Susceptibility Testing (C&DST) register. The key variables entered are shown in the table below.
Table: Key Variables entered in C&DST Register; Source: Guidelines for PMDT in India, 2021. VARIABLES SET 1 VARIABLES SET 2 VARIABLES SET 3 VARIABLES SET 4 Test ID Health Facility (HF) name Residential district Current facility HF type Date of test updated in Nikshay Lab type Type of test Predominant symptom Date tested Patient ID Reason for testing Predominant symptom duration Date reported Episode ID Treatment status History of Anti-TB Treatment (ATT) Test status Name Diagnosis date No. of Health Care Provider (HCP) visited before the diagnosis of the current episode Type of specimen Gender TB treatment start date The visual appearance of sputum Date of specimen collection Age Current facility state State name Primary phone Current facility district District name Address Current facility TB Unit (TU) TB unit Residential state Current facility HF NAAT results are reported in the results section of “Request Form for examination of biological specimen for TB” including:
- Select Type of test: Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ TrueNAT
- Select Sample: A/B
- Select M. tuberculosis: Detected/ Not Detected/ Not Available (NA)
- Select Rif Resistance: Detected/ Not Detected/ Indeterminate/ NA
- Select Test: No result/ Invalid/ Error; Error code
- Date tested
- Date Reported
- Reported by (name and signature)
- Laboratory name
Video fileVideo : CBNAAT/Truenat Results Entry in Lab Register
Resources
Monitoring Different Types of Errors with Truenat
ContentMonitoring of Truenat errors
There are various types of errors that occur with the Truenat machines, which include:
- Coded errors related to the Trueprep AUTO v2 sample prep device
- Coded errors related to the Truelab micro-PCR Analyzer
- Non-coded system errors/failures
Monitoring the Trueprep AUTO v2 errors
-
The Truenat system is a closed amplification system (i.e., the amplified product is sealed in the chip), and an enzyme system is incorporated in the reaction mix to prevent previously amplified material from getting re-amplified.
- It is recommended that testing sites perform negative control tests using Trueprep AUTO lysis buffer reagent and sterile Phosphate Buffered Saline (PBS) monthly or when contamination is suspected (e.g., an unusually high proportion of specimens with ‘M.tb detected’).
- Swab testing of work surfaces and both the Truelab and Trueprep machines should be conducted monthly.
- Used and expired cartridges should be discarded as per the protocols, so they are not re-used.
Monitoring the Truelab errors
-
To ensure that the Truelab micro Polymerase Chain Reaction (PCR) Analyzer is working accurately, the manufacturer recommends running positive and negative controls (which can be purchased as part of the Truenat™ Positive Control Kit- Panel I) periodically.
- The positive and negative controls can also be used for lot-to-lot verification and assessment of reagents if the temperature of storage areas falls outside the recommended ranges.
- An optional “Plot” view on the digital interface is also available while the process is being performed that allows for monitoring test progress in real-time.
- Truelab Analyzers can be configured to send data on device performance to the manufacturer’s (default configuration) or local servers to allow the manufacturer (without sharing any patient data) and/or the National TB Elimination Programme to monitor instrument performance on a real-time basis.
- This helps in the identification and possible prevention of instrument malfunctions or breakdowns, detection of user errors and retraining needs, and monitoring of instrument and test utilization across fleets of instruments.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India;CTD, MoHFW, India,2021.
- Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device; User Manual V4.
- TRUELAB UNO Dx Real Time Quantitative micro PCR Analyzer; manual VER 04.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Identify if the statement is True or False
Running positive and negative controls periodically is recommended to ensure that the Truelab micro PCR Analyzer is working accurately.
True False 1 Running positive and negative controls periodically is recommended by the manufacturer to ensure that the Truelab micro PCR Analyzer is working accurately Yes Yes Truelab Analyzers can be configured to send data on device performance to the manufacturer’s (default configuration) or local servers to allow the manufacturer (without sharing any patient data) and/or the National TB Elimination Programme to monitor instrument performance on a real-time basis.
True False 1 This helps in the identification and possible prevention of instrument malfunctions or breakdowns, detection of user errors and retraining needs, and monitoring of instrument and test utilization across fleets of instruments. Yes
Yes
-
STLS: Troubleshooting in Truenat
FullscreenTrueprep Error Classes and actions
ContentTrueprep Error Classes
The Trueprep errors are classified as:
-
Cartridge Errors
-
Reagent Pack Errors
-
Device Errors and Warnings
Image
Figure 1: Classification of Trueprep errors
Trueprep Error Actions
I Cartridge Error Actions
Image
Figure 2: Actions for Trueprep cartridge errors
II Reagent Error Actions
Image
Figure 3: Actions for Trueprep reagent errors
III Device Error and Warning Actions
Image
Figure 4: Actions for Trueprep device errors and warnings
Resource
-
Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
-
Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device; User Manual V4.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In ‘E11 – RTD L Error’, what does L stand for?
Liquid
Lower
Light
Lysis
4
In E11 - RTD L Error (The code L is for error in the Lysis Heater)
Yes
Yes
-
Truelab Error Classes and actions
ContentHere we discuss the error classes and actions in Truelab.
Truelab Errors - Classes and Actions
Error Class
Error Name
Reason for the error
Error Actions
Error 1
Thermal Cycling Error
Occurs when the test chip is faulty and the thermal cycling does not happen.
Re-run the same elute using another chip. If the error repeats, process the sample again and re-run the elute using another chip. If the problem still persists, contact the Molbio support team.
Error 2
Test Stopped Manually
Occurs when the user has manually stopped the ongoing test and the analyser does not have sufficient run time to compute data.
Error 3
Incorrect Optical Profile
Occurs when there is a deviation in the expected optical profile due to a reduction in reaction volume in the chip during the course of the reaction.
Error 4
Runtime Error
Occurs when run data capture/ analysis is incomplete.
Error 5
Probe Check Error
Occurs in the event of a low initial signal due to insufficient mastermix dispensed onto the chip.
Invalid
Whenever Truelab displays the result as 'INVALID', it means that the internal control did not amplify in Polymerase Chain Reaction (PCR) or sample extraction was not proper.
Resources
-
Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device, User Manual Version 4.
-
Truelab UNO Dx Real-time Quantitative Micro PCR Analyzer Manual Version 4.
-
Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
When does thermal cycling error occur in Truelab's real-time micro PCR analyzer?
Occurs when the test chip is faulty and the thermal cycling does not happen.
Occurs when run data capture/ analysis is incomplete.
Occurs in the event of low initial signal.
Occurs when the user has manually stopped the ongoing test.
1
Thermal cycling error occurs when the test chip is faulty and the thermal cycling does not happen.
Yes
Yes
When does the Runtime Error occur in Truelab's real-time micro PCR analyzer? Occurs when the test chip is faulty and the thermal cycling does not happen.
Occurs when run data capture/ analysis is incomplete.
Occurs in the event of low initial signal.
Occurs when the user has manually stopped the ongoing test.
2 Runtime error occurs when run data capture/ analysis is incomplete. Yes
Yes
-
Troubleshooting Failures Without Error Codes
ContentThe Truenat is a rapid molecular diagnostic method based on the Nucleic Acid Amplification Testing (NAAT) principle. Truenat uses portable, battery-operated devices to rapidly detect Mycobacterium tuberculosis Complex Bacteria (MTBC) and Rifampicin resistance.
Truenat system involves two main devices:
- Trueprep® AUTO v2 Universal Cartridge based Sample Prep Device: Used for the automated extraction and purification of DeoxyriboNucleic Acid (DNA).
- Truelab® Real Time micro-PCR Analyzer: Used for performing Real-Time Polymerase Chain Reaction (RT-PCR), resulting in the semi-quantitative detection of MTBC.
The errors in Truenat are broadly categorised as:
- Errors with codes (Trueprep and Truelab errors)
- Errors without codes (System failures)
The errors without codes in Truenat and the ways to resolve them are listed in the table below:
Sl. No. System failures Reason Troubleshoot 1 ‘Unable to read chip information’ Analyzer was unable to read chip memory Check if the chip was loaded properly into the tray. Remove the chip and re-select the profile from Status Screen and repeat the steps. If the message reappears, load a new chip and re-load the elute again 2 ‘Could not initialize. Please try again’ The system was unable to establish an internal connection Attempt the test again by using a new chip and re-loading the elute again 3 “Chip is already used” OR “Chip loaded is expired” User loaded a used chip/expired chip in the tray Use a fresh chip and re-load the elute 4 Login attempt failure Login failed due to incorrect password entered Re-enter the correct password 5 Invalid patient name in sample details screen The patient’s name in the sample details section is blank Fill patient’s name in the sample details section Resource
-
Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India; CTD, MoHFW, India. 2021.
-
Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device; User Manual V4.
-
TRUELAB UNO Dx Real Time Quantitative micro PCR Analyzer; manual VER 04.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What should you do when you get a system failure alert as:
“ Chip is already used” ?
Re-insert the same chip
Insert a fresh chip
Do not insert any chip
None of the above
2
When you get a system failure alert as: “ Chip is already used” , Use a fresh chip and re-load the elute.
Yes
Yes
What should you do when you get a system failure alert as:
"Unable to read chip information"
Re-insert the same chip
Insert a fresh chip
Do not insert any chip
Check if chip is loaded properly, remove the chip and reselect the profile from status screen and repeat the steps.
4 When you get a system failure alert as "Unable to read chip information" Check if the chip was loaded properly into the tray. Remove the chip and re-select the profile from Status Screen and repeat the steps. If the message reappears, load a new chip and re-load the elute again Yes
Yes
Reset Procedure for Truenat Testing
ContentAfter completion of the set number of nucleic acid extractions (i.e., buffer count 05/ 25/ 50/ 100 completed) the Trueprep AUTO v2 device will prompt the alert on its 2- line LCD screen to “Change the reagent pack” and “Insert Reagent Reset Card & Start” on the screen alternatively. When this happens, the new reagent pack needs to be inserted into the device and the buffer count needs to be reset.
Image
Flowchart: Procedure for Reset in Truenat Testing
Image
Figure: 1) The Trueprep AUTO v2 Back Panel, with tubing and caps for plugging in reagent bottles 2) The Trueprep AUTO v2 device Back Panel with Reagent Pack 3) Reagent Reset Card; Source:Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device User Manual.
Resources
- Trueprep AUTO v2 Universal Cartridge Based Sample Prep Device User Manual.
- Trueprep AUTO v2 Pack Insert Version 04.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The buffer count in the Trueprep Auto V2 device will be set to what after the reset procedure is completed? 0 1 10 100 1 The buffer count will be reset to ‘0’ once the reset procedure is completed. Yes Yes
-
STLS: Truenat Instrument maintenance and record keeping
FullscreenMaintenance of the Truenat Instrument - General Principles
ContentLike any other laboratory instrument, the TrueNAT machine needs a periodic maintenance.
Maintenance of Truelab and Trueprep instruments includes:
- Cleaning the instrument
- Disinfecting the surfaces
- Cleaning the spillages
- Discarding the used consumables
- Calibrations
- Replacement of parts
- Flush protocol
- Data backup
- Troubleshooting errors, alerts, warning messages
Frequency of maintenance:
The following schedule is required to maintain TrueNAT instrument(s):
- Daily, monthly maintenance by lab personnel
- As and when required (need based) by lab personnel/ manufacturer
- Annual maintenance by the manufacturer.
Posters on maintenance provided by manufacturer are shown in Figure 1(A)- (B)
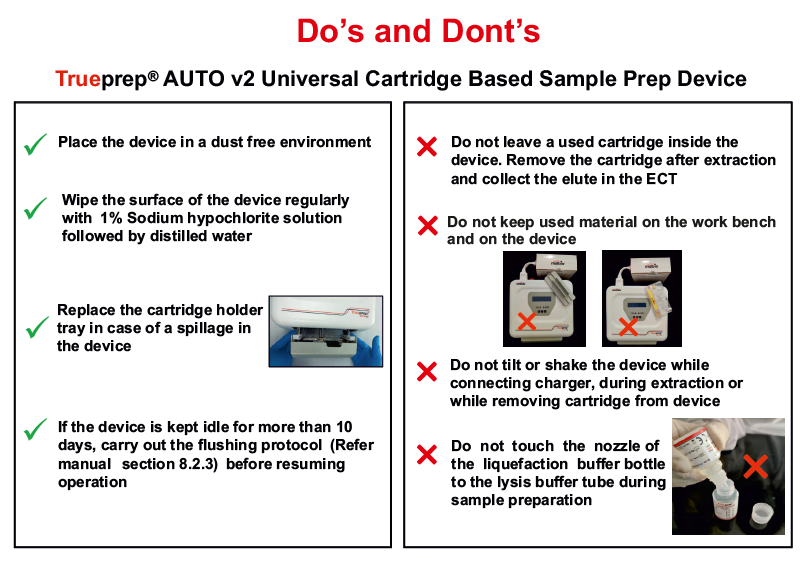
Figure 1(A): Considerations (Do’s and Don’ts) for use of Trueprep Device; Source: MolBio Diagnostics Pvt. Ltd.
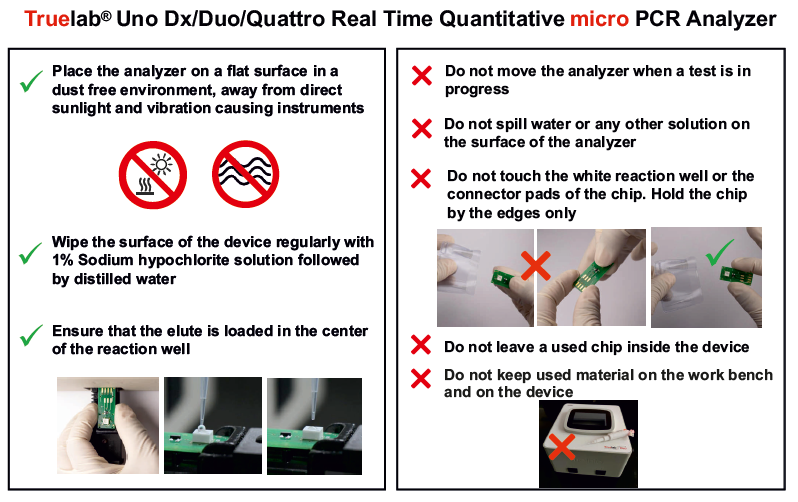
Figure 1(B): Considerations (Do’s and Don’ts) for use of Truelab Device; Source: MolBio Diagnostics Pvt. Ltd.
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- Trueprep Manual.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
Ensuring Compliance of Truenat Instrument Installation Criteria
ContentCompliance to equipment installation criteria is necessary to/for:
- Establish accurate and reliable results as claimed by the manufacturer
- To assure standard/specific requirements are met
- Provide proof that the process will consistently produce predetermined outcome
- Equipment safety
- Improve overall performance of the equipment
- Decrease work interruptions due to equipment failure
- Lower repair costs
- Cover equipment warranty and free maintenance
Instrument Qualification Documents include:
- Installation Qualification- IQ
- Operational Qualification- OQ
- Performance Qualification- PQ
Installation Qualification
IQ provides evidence for delivery, installation and configuration of the instrument as per manufacturer’s standards using an installation checklist.
Operational Qualification
OQ is a collection of test cases used to verify the proper functioning of a system before the instrument is released for use.
Performance Qualification
PQ is a collection of test cases used to verify that the system performs as expected under simulated real-world conditions.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Daily, Weekly and Monthly Maintenance of Truenat Instrument
ContentDaily maintenance of Truelab and Trueprep instruments performed by the laboratory personnel includes:
- Maintaining a dust-free environment by wiping the exterior of instruments with a dry, lint-free cloth
- Cleaning the surface of the Trueprep device once with 70% ethanol
- Cleaning the spill or leak with a cloth or tissue-paper dipped in disinfectant (1% sodium hypochlorite solution, followed by 70% ethanol)
- Not spilling water or any other solution on the surface of instruments
- Discarding used cartridges, chips, reagent bottles and other consumables in 1% sodium hypochlorite solution, soaking for minimum 30 minutes, and disposing as per the biomedical waste management guidelines.
Monthly maintenance of the Truelab Analyzer performed by laboratory personnel includes:
- Cleaning the surface of the Truelab Analyzer with 70% ethanol
- Cleaning the Truelab bays
- Calibrating temperature.
Annual/ need-based maintenance of the Truenat instrument performed by the laboratory personnel/ manufacturer includes:
- Flush protocol for the Trueprep device when the device is left idle (not used) for 10 days and/ or errors relating to extraction process occur
- Replacement of spillage tray or linear motion guide tray for the Trueprep device in case of sample spillage on trays during extraction or when cross-contamination is suspected
- Replacement of slider glass for Truelab Analyzer after 200 tests and/ or when related errors occur
- Temperature calibration for Truelab Analyzer when error related to temperature occur and/ or when the temperature curve is abnormal (shows blips)
- Calibration of micropipettes (every 6 months/ biannual).
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- Trueprep Manual.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
NAAT Instrument Monthly Data Archive and Data Back-up
ContentSecurity of laboratory data and confidentiality of TB patient data are important. Hence, it is recommended to archive or take periodic data backup.
The Truelab Analyzer has an internal memory to store 20000 test results. The digital data can be transmitted through connectivity via email, SIM card, Wi-Fi or Bluetooth.
Recommended ways of documenting the results and archiving data are:
- Records should be maintained in the National TB Elimination Program (NTEP) recording and reporting formats.
- Entries should be made in Nikshay online platform of NTEP.
- Monthly/ periodically data should be exported in CSV format and saved on external devices-desktop/ laptop/ hard drive.
- Data records from Nucleic Acid Amplification Testing (NAAT) instruments should be kept in a secure area.
- Data access should be given to authorized personnel only.
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
Annual Maintenance of the Truenat Instrument
ContentNeed-based maintenance for Truenat instrument is done by lab personnel/ manufacturer while the manufacturer does annual maintenance.
The tasks included under annual maintenance are:
- Flush protocol for Trueprep device when the device is left idle (not used) for 10 days/ annually and/or errors relating to extraction process occur.
- Spillage tray or linear motion guide tray replacement for Trueprep device in case of sample spillage on trays during extraction or when cross-contamination is suspected/ done annually.
- Slider glass replacement for Truelab Analyzer after 200 tests/ annually and/or when related errors occur.
- Temperature calibration for Truelab Analyzer when error related to temperature occur and/or when temperature curve is abnormal (shows blips)/ annually.
- Annual calibration of micropipettes.
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- Trueprep Manual.
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
STLS: TB infection testing
Fullscreen-
STLS: TB infection
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
Contact Tracing and Investigation
ContentContact tracing is a process to identify people who are at a high risk of developing TB due to their contact with a known TB case.
The aim of contact tracing is to find other people with TB disease and those infected with TB
All close contacts, especially household contacts of a Pulmonary TB patient, should be screened for TB.
In paediatric TB patients, reverse contact tracing for the search of any active TB case in the child's household must be undertaken.
Particular attention should be paid to contacts with the highest susceptibility to TB infection.
Figure: Contacts to be Prioritized for contact TB screening
How to do contact tracing
ContentIndex TB patient: Initially identified person of any age with new or recurrent TB in a specific household or other comparable settings in which others may have been exposed. The Index TB patient is the person on whom a contact investigation is centred, but is not necessarily the source/ primary case.
Contact: Any individual who was exposed to a person with active TB disease
Household Contact (HHC): Person who shared the same enclosed living space as the index TB patient for one or more nights or for frequent or extended daytime periods during the three months before the start of current TB treatment.
Close contact: Person who is not in the household but shared an enclosed space, such as at a social gathering, workplace or facility, for extended periods during the day with the index TB patient during the three months before the commencement of the current TB treatment episode.
Contact tracing: Contact tracing is the process of listing out all the contacts (household contacts and close contacts) of the index TB patient. Contact tracing has to be done for all Index TB cases, whether pulmonary (sputum positive or negative) or Extra-pulmonary (EPTB). As per the current policy, it is compulsory to trace household contacts but it is desirable to trace other close contacts (workplace, social gathering etc) also.
Why Contact Tracing is done: Contact tracing is followed by contact investigation to identify active TB cases and Tuberculosis Preventive Treatment (TPT) beneficiaries.
Contact investigation: This is a systematic process for identifying previously undiagnosed people with TB disease and TB infection, among the contacts of an index TB patient.
Conducting Contact Tracing and Contact Investigation
Once a new/ recurrent TB case is diagnosed (ideally within 1 week), a healthcare worker (usually the Multipurpose Worker (MPW) from the nearby public health facility visits/ tele calls the patient’s household, interviews the patient about his/her contacts in the household and other settings such as workplace or social gatherings. The contacts’ details are recorded in a standardised format and entered in Ni-kshay contact tracing module. Each contact's details enter the workflow as a presumptive TB case or TPT beneficiary.
The traced contacts are screened for TB using a symptom checklist and if found to have any symptoms suggestive of TB, they are tested using X-ray/ sputum microscopy/ Cartridge-based Nucleic Acid Amplification Test (CBNAAT) as required.
Outcome of Contact Tracing and Contact Investigation
- Those contacts diagnosed with active TB are initiated TB treatment.
- As per the current policy, those HHC of sputum-positive Pulmonary TB (PTB), in whom active TB disease is ruled out, are considered for TB Preventive Therapy (TPT)
References
- Guidelines for Programmatic Management of TB Preventive Treatment in India, 2021.
- Technical and Operational Guidelines for Tuberculosis Control in India, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements are true?
Contact tracing should always be followed by contact investigation.
Household contacts of Extrapulmonary TB are offered TPT.
The index case is always the primary source of infection in the household.
Contact tracing and investigation need to be done only during ACF campaigns.
1
2- Only HHC of Sputum positive PTB cases are offered TPT.
3 – The index case need not be the primary source of infection in the household.
4 – Contact tracing and investigation are to be done routinely for all TB cases. ACF campaigns are only an added measure.
Yes
Yes
Recording and Reporting Contact Tracing [Ni-kshay]
ContentContact Tracing plays an important role in the detection of all those who are secondarily infected for proper diagnosis and prompt treatment. This process can be recorded and reported in Ni-kshay under the ‘contact tracing’ option. The process of recording contact tracing in Ni-kshay is given below.
Process Overview
Image
Detailed Step-wise Procedure
Step 1: Login to the Ni-kshay ecosystem and enter the patient ID for which the contact tracing details are being recorded.
Step 2: Click on the ‘Contact tracing’ tab to reach the contact tracing window.
Image
Step 3: Click on the 'Edit' tab and fill in the relevant information in the fields provided.
Image
Step 4: Once the details are entered, click on the ‘update’ tab present at the upper right corner of the window to finish the process. A message will be displayed by the system once the details are updated successfully.
Image
Step 5: Once the details are updated successfully, an option to add the contact will appear at the upper right corner of the contact tracing window. This option can be used to add contacts as Beneficiaries (Presumptive TB/ TB Preventive Treatment (TPT) beneficiaries) in the system.
Image
Step 6: Selecting the 'Add contact' tab will take the user to the enrollment window. The process of entering information in this window is similar to adding a New presumptive TB case in Ni-kshay, except that the option of “Contact of Known TB Patient” is automatically selected for the field “Key Population”.
Once the contact is added as a beneficiary (Presumptive TB/ TPT beneficiary) in the system, the contact details can be seen in the contact tracing tab.
Video fileVideo: Recording Contact tracing in Ni-kshay (Web)
Video fileVideo: Recording Contact tracing in Ni-kshay (Mobile App)
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Pre-test Contact tracing plays an important role in the detection of all those who are secondarily infected. False True 2 Contact tracing plays an important role in the detection of all those who are secondarily infected for proper diagnosis and prompt treatment. Yes Yes
-
-
STLS: Ensuring Smooth functioning of Lab Services
Fullscreen-
STLS: Biomedical waste management in a microscopy lab
Fullscreencolor coding and type of container
ContentThe National TB Elimination Programme (NTEP) utilizes different coloured bags for the segregation of waste generated in TB laboratory settings as shown in the table below.
Table: Waste Segregated and Collected According to Colour-coded Bags
Yellow bag:
- Broomsticks
- Parafilm tape & plastic bag – contaminated with samples
- Löwenstein-Jensen (LJ) media without the bottle
- Microbial sample/ blood/ body fluids contaminated paper/ cotton/ swab
- Blood bags
- Microbiological cultures Truenat chips (MTB/ Rif)
- Used mask/ gowns
- Expired medicines/ drugs/ antibiotics
Red bag:
- Specimen collection tubes
- Sputum cups
- Cartridge Based Nucleic Acid Amplification Test (NAAT)/ Truenat cartridges
- Infected plastic
- Contaminated tips
- Pasteur pipettes
- Polymerase Chain Reaction (PCR) tubes
- Mycobacteria Growth Indicator Tube (MGIT) tubes
- Disposable LJ tubes
- Contaminated falcon tubes
- Used gloves
- Contaminated droppers
- Empty Cartridge-based Nucleic Acid Amplification Test (CBNAAT) reagent bottles

Blue bag:
Glass slide in Truenat machine and used microscopy slides. Slides should not be broken.
All these bags are to be labelled with the Biohazard logo (figure below) on them.
Figure: Biohazard Logo
- Waste generated in the Culture Drug Susceptibility Testing (CDST) laboratories is autoclaved prior to segregation in colour-coded bags.
- The biohazard materials are collected and handed over to handlers authorized by the pollution control board.
- Personnel handling/segregating biomedical wastes must use appropriate Personal Protective Equipment (PPE) and should be trained in spill management.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, 2021.
- Guidelines for Management of Healthcare Waste as per Biomedical Waste Management Rules, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
Preparation of TB Lab Disinfectants
ContentDisinfectants used in lab settings include:
1% Sodium Hypochlorite
- Broad spectrum antimicrobial action
- Used to disinfect surfaces
- Used to disinfect infectious material and disposal of used Truenat consumables (reagent bottles, cartridges, tips, chips)
- Hazardous and corrosive, to be used with care
- Is highly alkaline so can corrode metal
- Waste soaked in Sodium Hypochlorite should not be discarded by autoclaving.
70% Alcohol
- Bactericidal action
- Used for surface decontamination only
- Highly inflammable; keep away from fire
- Used to disinfect biosafety cabinets, laboratory benches and surface of instruments.
5% Phenol
- Used for decontaminating Cartridge-based Nucleic Acid Amplification Testing (CBNAAT) equipment and single-use items like CBNAAT cartridges prior to disposal
- Highly irritating to the skin, eyes and mucous membranes.
Preparation of these disinfectants is described below.
Preparation of 1% Sodium Hypochlorite
- Use commercially available 4% sodium hypochlorite solution.
- Dilute with distilled water to prepare required amount of 1% sodium hypochlorite
- E.g.: To prepare 100 ml of 1% sodium hypochlorite: 75 ml distilled water plus 25 ml 4% sodium hypochlorite solution.
- Sodium hypochlorite solutions (domestic bleach) contain 50 g/l available chlorine, and should therefore be diluted to 1:50 or 1:10 in water to obtain the final concentrations of 1 g/l or 5 g/l when used as a general-purpose disinfectant for TB laboratories.
- To be prepared fresh.
Preparation of 70% Alcohol
- Use commercially available absolute alcohol.
- Dilute with distilled water to prepare the required amount of 70% alcohol
- E.g.: To prepare 100 ml of 70% alcohol: 70 ml absolute alcohol plus 30 ml distilled water.
Preparation of 5% Phenol
- Melt 5 g of phenol by heating it.
- Dissolve in 100 ml distilled water.
Video fileVideo : Preparation of TB Lab Disinfectants
Resources
Disposing Off Contaminated Material Safely in DMC Laboratory Settings
ContentThe Laboratory Technician (LT) must safely discard contaminated, biohazard waste generated by tuberculosis (TB) laboratories. This waste must be discarded along with the overall waste of the health facility in which TB services are provided.
There are 2 types of waste generated from DMC laboratory settings:
- Sputum containers with specimen and wooden sticks
- Stained slides
Disposal of Sputum Cups with Left-over Specimen, Lids and Wooden Sticks
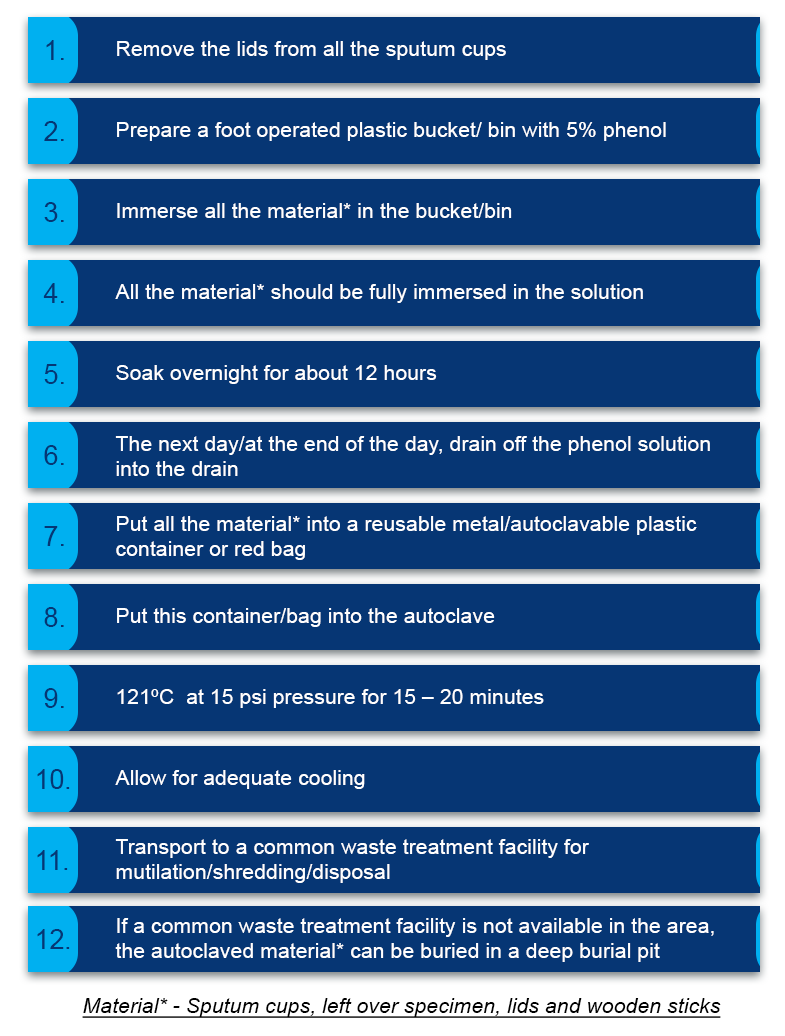
Figure 1: Steps for disposal of sputum cups with specimen, lids and wooden sticks
Important Points to Remember
- If autoclaving is not possible, boil in a pressure cooker of 7 litre capacity with water and submerge the contents for at least 20 minutes
- LTs and support staff handling biological waste need to wear gloves
- The red bag used for autoclaving must:
- Have a biohazard symbol
- Have adequate strength to withstand the load of the waste material
- Be made of non-PVC plastic material
Disposal of Stained Slides
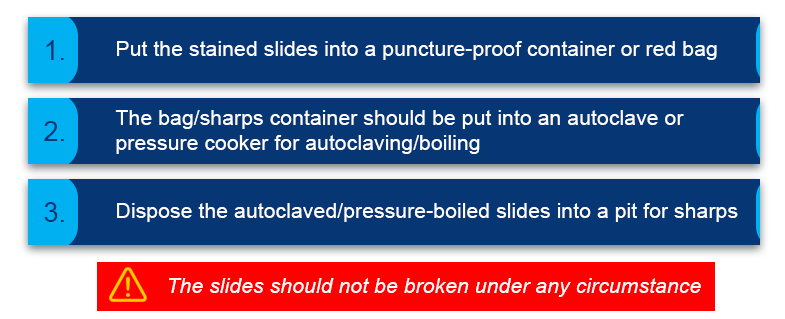
Figure 2: Steps for disposal of stained slides
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Biomedical waste management in CBNAAT Lab
FullscreenBiosafety measures required for CBNAAT
ContentIt is essential to follow biosafety protocols while handling specimens and cartridges. This will prevent anyone handling the specimens and cartridges from getting infected.
General Biosafety Requirements for CBNAAT
Cartridge-based Nucleic Acid Amplification Test (CBNAAT) is a low-risk procedure and requires the same level of precautions, like those used for direct Acid-fast Bacillus (AFB) sputum smear microscopy:
- Carry out the procedure in a well-ventilated area.
- Wear gloves and a laboratory coat at all times when handling patient samples.
- Minimize the generation of aerosols during sample processing and handle specimens carefully and responsibly.
Based on risk assessment, additional biosafety precautions may be required in CBNAAT laboratories, such as the use of N95 respirators or biosafety cabinets.
Personal Protective Equipment (PPE) is important, but it does not replace good microbiological and good laboratory practices. They include:
Gloves: Essential (disposable and powder-free)
Laboratory coats: Essential
Respirators: Usually not required, but:
- May be needed, based on risk assessment.
- Must always be included in a spill kit.
- Recommended respirators are N95 or chosen based on program guidelines.
Precautions to take while preparing samples for CBNAAT testing
- The sample reagent should be added to the specimen in such a manner that the procedure minimizes aerosol generation.
- Although the sample reagent inactivates M. tuberculosis bacilli, it reduces, but does not eliminate, the biosafety risk to the laboratory technician.
- There is an increased risk of generating aerosols when splitting and handling concentrated and extrapulmonary TB specimens. These procedures must be performed in a certified biosafety cabinet.
Precautions during cartridge loading and transport
- When transferring cartridges to the machine for loading, an appropriate size enclosed container should be used.
- Care should be taken, as samples may leak if the cartridges are toppled during transport.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Disposal of Infectious Samples and Used Cartridges in CBNAAT Lab
ContentDisposal of biohazardous waste is essential to prevent contamination and possible infection of those handling the infected specimens.
At the end of each day, Cartridge-based Nucleic Acid Amplification Test (CBNAAT) laboratories generate contaminated material such as:
- Used sputum containers
- Used cartridges
- Transfer pipettes.
All used materials should be considered contaminated.
All infectious samples should be sealed in a biohazard bag and disposed off according to Biohazard Waste Disposal Guidelines under the National Pollution Control Guidelines, 2019.
- Contaminated materials should be picked up with a gloved hand and placed in a closed lid container of 5% phenol solution or a biohazard bag.
- At the end of the day, the phenol should be drained, and the materials/ bags should be autoclaved at 121°C at 15 psi pressure for 20 minutes.
- Once done, the materials should be cooled and sent to the common waste treatment facility for mutilation/ shredding or disposal.
It is a good practice to display the Standard Operating Procedures (SOPs) for the disposal of each item in the CBNAAT laboratory.
Resources
-
-
STLS: Ensuring Quality TB lab services at TDCs
Fullscreen-
STLS: General concepts in quality assurance
FullscreenStoring slides at a DMC for QA
ContentIt is important to store slides, after reading as these will be required for Quality assurance - internal rechecking by the supervisor, and for External Quality Assurance (EQA) as per National TB Elimination Programme (NTEP) guidelines.
- Prior to storage slides need to be dried by gently placing the slide gently face down on the tissue paper or by wrapping it in the tissue paper and leaving it overnight to remove excess oil (Figure 1).
Figure 1: Using Tissue Paper to Drain Oil
- The slides are to be stored in the slide box in the same order as they are listed in the laboratory register (Figure 2).
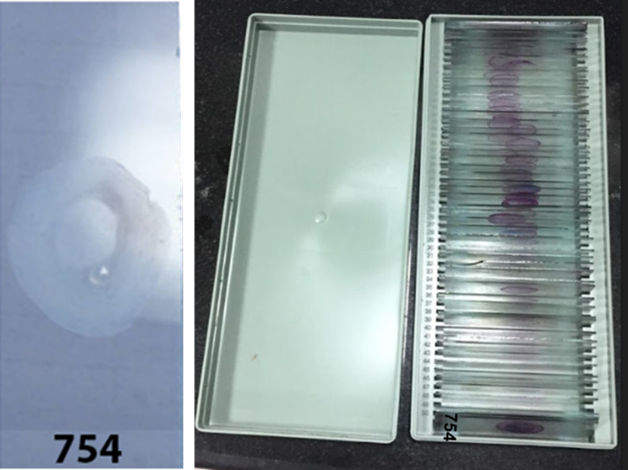
Figure 2: Keeping the Slides in Same Order as Listed in the Laboratory Register
- One blank place must be left behind the first slide from a patient suspected with TB this allows the second slide of the same patient to be added after reading. This process will keep results consistent with the laboratory register (Figure 3).
Figure 3: Keeping Blank Spaces Between Slides for Consistency
- Always store slides in closed slide boxes away from sunlight (Figure 4).

Figure 4: Storing Slides in Closed Slide Boxes

Resources
- Manual for Sputum Smear Fluorescence Microscopy, RNTCP, MoHFW, 2007.
- Laboratory Diagnosis of Tuberculosis by Sputum Microscopy, GLI Initiative.
Kindly provide your valuable feedback on the page to the link provided HERE
False Positivity and False Negativity in Microscopy
ContentFalse result: It’s a situation where the test result is different from the truth.
Types of False Results
- False Positive: When the test result is positive but the patient does not have TB.
- False Negative: When the test result is negative but the patient has TB.
Both cases will lead to wrong categorization and incorrect treatment. The consequences of false results are shown in the figure below:
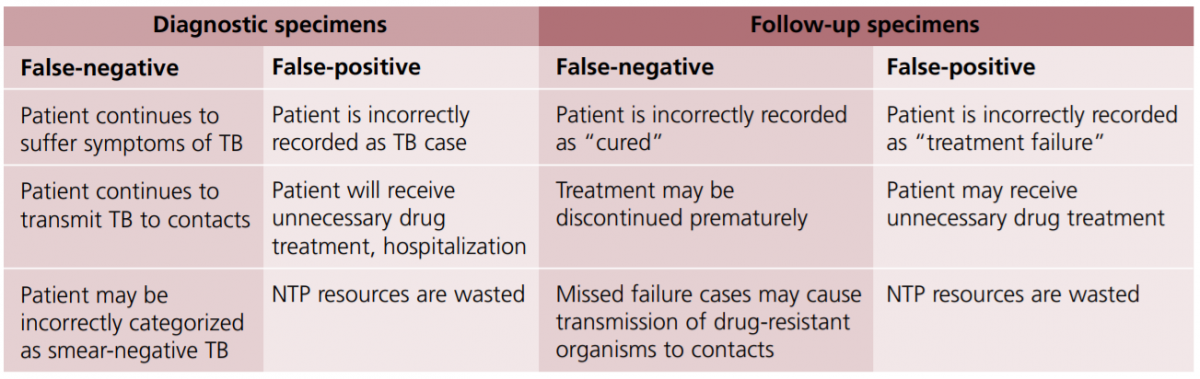
Figure: Consequences of False Results in Sputum Smear Microscopy; Source: Quality Assurance of Sputum Microscopy in DOTS Programmes.
Resources
- RNTCP Module for Laboratory Technicians, CTD, MoHFW, 2005.
- Quality Assurance of Sputum Microscopy in DOTS Programmes Regional Guidelines for Countries in the Western Pacific, WHO, 2003.
Kindly provide your valuable feedback on the page to the link provided HERE
Need for Quality Testing and Control
ContentQuality Assurance (QA) is a systematic process used to determine the quality standards of TB laboratories.
Poor quality diagnosis may results in failure to diagnose TB or unnecessary treatment of non-TB case. Thus an effective QA mechanism is important for reliability of laboratory diagnosis.
QA in National Tuberculosis Elimination Programme (NTEP) consists of:
- Internal Quality Control (QC)
- External Quality Assessment (EQA)
- Continuous Quality Improvement (QI)
QC or Internal Quality Assurance is a systematic internal monitoring of working practices, technical procedures, checking equipment, new lot of reagents, smear preparation, grading etc
EQA is a process to assess laboratory performance by comparing laboratory results with a laboratory in higher tier i.e.Intermediate Reference Laboratory (IRL)/ National Reference Laboratory (NRL) through on-site evaluation, panel testing and random blinded rechecking of slides. Figure 1 depicts an eg of on-site evaluation with roles of various stakeholders and frequency of this activity.

Figure 1: On-site evaluation (RNTCP Laboratory Network Guidelines)
QI is continuous monitoring of laboratory performance, finding non compliance and taking remedial measures to prevent recurrence of problems
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Quality Improvement mostly relies on effective on-site evaluation visits?
True
False
1
Quality Improvement mostly relies on effective on-site evaluation visits.
Yes
Yes
Measures for Quality Assurance in Microscopy
ContentSputum smear microscopy is an integral part of the National TB Elimination Programme's (NTEP’s) diagnostic services and can majorly impact the success of the programme.
It is essential to have a credible and well-established quality assurance system to assess the performance of the microscopy service.
NTEP has implemented a multi-level quality assurance network system of sputum smear microscopy in the country consisting of:
- Internal Quality Control (IQC)
- External Quality Assessment (EQA)
- Quality Improvement (QI)
- Internal Quality Control is a process of effective and systematic internal monitoring of the working practices.
- It includes technical procedures, checking instruments, quality of new batches of staining solution, smear preparation, grading, equipment infection control measures, waste management, etc.
- For the purpose of IQC, it should be ensured that all staining reagents’ dye content is mentioned on the bottle, concentrated acids are stored carefully in separate containers and stains are filtered before use.
- Further, after each new batch of reagents is made, Quality Control Positive (QCP) and Quality Control Negative (QCN) slides should be prepared by the Senior TB Lab Supervisor (STLS) for quality control.
- QCP slides should be prepared by pooling 3+ grade sputum samples, while QCN slides are to be prepared by pooling negative sputum samples with an adequate number of pus cells (≥10 pus cells/ field).
- One set of QCP-QCN slides should be stained by STLS and another set should be given to the Designated Microscopic Centre (DMC) Lab Technician (LT) along with the reagent, and the results of both should be entered in the batch register/ IQC document.
- All quality control slides should be stored for a maximum period of Four months. For the microscope, the lens should be cleaned with tissue paper after examining each slide and stored inside a microscope box at the end of the day.
- The microscope box should contain silica gel and an electric bulb of 10-15 watts for desiccation to prevent fungal growth on the lens. The silica gel should be dehydrated periodically under direct sunlight. All microscopes should be covered under the Annual Maintenance Contract (AMC) with routine preventive maintenance.
- External Quality Assessment (EQA) is a process to assess the performance of the peripheral laboratories by a more competent laboratory, like the intermediate or the national reference laboratory.
- EQA has 3 components:
1) Onsite evaluation of peripheral laboratories by the supervisors from the reference laboratory under actual working conditions, in order to review the internal quality control mechanisms in place.
2) Panel testing of the slides (unstained and stained) received from the reference laboratory by the peripheral laboratory LT to evaluate the smear microscopy process. This helps to determine whether the LT can adequately perform Acid-fast Bacilli (AFB) smear microscopy.
3) Random blinded re-checking of a small sample of routine slides (both positive and negative) in the peripheral laboratory by the reference laboratory to assess the accuracy of the reading.
- Quality Improvement (QI) is a process by which all components of smear microscopy diagnostic services are continuously monitored and carefully analysed with the aim to identify the problems and implement corrective actions (including retraining) to prevent the recurrence of the problems.
Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- Guidelines for Quality Assurance of Smear Microscopy for Diagnosing Tuberculosis, RNTCP Lab Network, CTD, MoHFW, India, 2005.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of these is systematic internal monitoring of working practices that includes technical procedures, staining solution, smear preparation, grading, equipment infection control measures and waste management? Onsite evaluative (OSE) External Quality Assessment (EQA) Internal Quality Control (IQC) Quality Improvement (QI) Internal Quality Control (IQC) Internal Quality Control (IQC) is systematic internal monitoring of working practices that includes technical procedures, staining solution, smear preparation, grading, equipment infection control measures and waste management. Yes Yes Quality control slides should be stored for a maximum period of how many months? 3 6 5 2 1 All quality control slides should be stored for a maximum period of three months.
Yes
Yes
Quality assurance of Stains and Internal Quality Control
-
STLS: External quality assurance
FullscreenGood Laboratory Practices
ContentGood laboratory practices help to maintain biosafety in TB lab settings. However, it is good to keep in mind that:
- NOTHING can totally eliminate the safety risk associated with the TB laboratory.
- Good laboratory practices with an emphasis on biosafety, significantly reduce the risk of laboratory-acquired infection.
- Specialized equipment aids good laboratory practice but does NOT replace it.
Good Laboratory Practices
- Biohazard signs (Figure 1) should be posted at the entrance to laboratories performing work on infectious agents and hazardous chemicals.
Figure 1: Biohazard Sign
- Laboratory access should be limited to essential staff.
- No eating, drinking, or smoking (Figure 2).
- No mouth pipetting (Figure 2).

Figure 2: No eating or mouth pipetting in lab
- No placing pencils or pens in the mouth.
- Keep hands away from eyes and face.
- Always wash hands before leaving the lab.
- Remove gloves before handling phones, instruments or computers.
- Minimize the use of mobile phones.
- Lab coats must be decontaminated and laundered regularly (never take them home for laundering!)
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Panel Testing
ContentPanel testing is a method of External Quality Assurance (EQA) that is used to determine the adequacy of a laboratory technician to perform Acid-fast Bacillus (AFB) smear microscopy. This method evaluates individual performance in staining and reading and not the other laboratory activities.
- Panel testing under National TB Elimination Programme (NTEP) is used for Intermediate Reference Laboratories (IRLs) and District TB Centres (DTCs) during on-site evaluation, because these institutions do not have routine slides for blinded rechecking.
- A panel consists of a batch of stained and/or unstained smears that are sent out by the higher-level reference laboratory to the peripheral laboratories for processing, reading, and reporting of results
- Panel testing is not performed as a routine in DMCs, as they will have regular on-site evaluation and blinded rechecking.
Uses of Panel Testing
- Supplement re-checking programmes
- Provide information on the capabilities of the peripheral laboratories prior to
implementing a re-checking program - Assess status level of performance or to quickly detect problems associated with very poor performance
- Evaluate proficiency of laboratory technicians following training
- Monitor performance of individuals when adequate resources are not available to implement a re-checking program.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Panel testing is useful to evaluate the proficiency of laboratory technicians following training.
True
False
1
Panel Testing is useful to evaluate the proficiency of laboratory technicians following training.
Yes
Yes
Onsite Evaluation[OSE]
ContentA field visit is an ideal way to obtain a realistic assessment of the conditions and skills practiced in the laboratory. Under National TB Elimination Programme (NTEP), On-site Evaluation (OSE) of Intermediate Reference Laboratories (IRLs) and District TB Centres (DTCs)/ Designated Microscopy Centres (DMCs) is therefore an essential component of a meaningful Quality Assurance (QA) programme.
OSE should be performed a tleast once a year by personnel from a higher-level laboratory (IRL/ National Reference Laboratory (NRL)) in order to evaluate the overall operational conditions in the microscopy centers.
Laboratory Supervisors must be knowledgeable in all operational and technical elements of AFB smear microscopy and have sufficient expertise to observe technicians performing routine tasks.
Importance of OSE
- Ensures that Standard Operating Procedures (SOPs) are in place and are displayed in all DMCs, internal Quality Check (QC) as per RNTCP is performed, and a functional binocular microscope is available
- Provides an opportunity for immediate problem-solving corrective action and on-site retraining.
Frequency of OSE (Figure)
- At least once a month visit by Senior TB Lab Supervisor (STLS) to the DMC, is required with re-checking of five positive and five negative slides.
- Regular on-site evaluation by District TB Officer (DTO) is important to assure recording and reporting of results; assessing operational conditions, safety, supplies, equipment and total workload.
- At least once a year visit by laboratory supervisors is recommended for IRLs by NRLs and for DTCs by IRLs.
- When poor performance has been identified through OSE, blinded rechecking or panel testing, additional visits by trained laboratory personnel from a higher-level laboratory (the IRL or NRL laboratory) supervisor are mandatory to perform a comprehensive evaluation of all laboratory procedures, implement corrective action, and provide training.
Components of OSE (Figure)
The visit includes:
- Comprehensive assessment of laboratory safety including infection control measures; conditions of equipment, adequacy of supplies as well as the technical components of Acid-fast Bacillus (AFB) smear microscopy. Sufficient time must be allotted for the visit to include observation of all the work associated with AFB smear microscopy, including preparing smears, staining and reading of smears.
- Examining a few stained positive and negative smears to observe the quality of smearing and staining as well as condition of the microscope
- Facilitating quality improvement through on the spot problem solving and suggestions for corrective action, wherever needed.
The NRLs provide training to all IRL personnel responsible for OSE. Additionally, non-laboratory personnel (e.g., DTOs) should acquire working knowledge of routine laboratory operations, including proper NTEP procedures, appropriate supplies, laboratory safety, basic microscope operations, and requirements of panel testing or rechecking programmes.

Figure: Frequency and Components of On-site Evaluation; Source: RNTCP Laboratory Network Guidelines
Checklist for IRL OSE and NRL OSE
On-site quarterly evaluation report of DTCs visited by IRL team to be given to concerned State TB Officer (STO), IRL and NRL using an IRL OSE Checklist while OSE checklist for NRL Laboratory Personnel to IRL is prepared using a NRL OSE Checklist.
Resources
RNTCP Laboratory Network Guidelines.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
On-site Evaluation provides an opportunity for immediate problem solving, corrective action and on-site retraining.
True
False
1
On-site Evaluation provides an opportunity for immediate problem solving, corrective action and on-site retraining.
Yes
Yes
OSE Feedback and action required
ContentDocumentation of any significant problems (technical, operational, others) and feedback for corrective action during On-site Evaluation (OSE) is necessary to formulate plans with the District TB Officer (DTO), Senior TB Laboratory Supervisor (STLS), Medical Officer (MO), Intermediate Reference Laboratory (IRL), National Reference Laboratory (NRL) and Laboratory Technician (LT) to improve the quality of smear microscopy.
Checklists for OSE
- OSE is done through comprehensive checklists.
- The checklist must be used by NRL, IRL and District TB Center (DTC) STLS and a shorter version by DTO/ Medical Officer TB Center (MOTC) during each OSE visit to document observations and corrective action.
- The checklists contain open, non-leading questions and recommended observations along with objective criteria for acceptable practices so that the supervisor can assess how well the technician understands proper procedures.
Feedback
Feedback is the process of communicating results of External Quality Assurance (EQA) to the original laboratory, including suggestions for possible causes of errors and remedies.
TB Unit On-site Evaluation (TU-OSE) Checklist and Feedback
The observations in TU-OSE Checklist, including observation of five positive and negative slides must be documented (Figure 1). Corrective actions must be discussed by the STLS with LT and checklist should be signed by MO of DMC.

1: Write smear and grade
2: Tick appropriate column
3: Tick if good; write ‘U’ if under-decolourized, ‘O’ if over-decolourized
4: Tick if good; write ‘B’ if too big, ‘S’ if too small
5: Tick if good; write ‘K’ if too thick, ‘N’ if too thin
6: Tick appropriate columnFigure 1: Review of five positive and five negative slides by STLS and instructions to fill observations in TU-OSE Checklist; Source: RNTCP Laboratory Network Guidelines
Action Required based on TU-OSE Checklist
The STLS should:
- Enter the summary of ‘action required’ in the Supervision Register before leaving the DMC
- Submit the summary report of DMCs under him to DTO on a monthly basis
- Maintain separate files for checklists including summary reports of each DMC in respective TU and submitted for review by higher level supervisors including on-site evaluation visits by the IRL to the district.
The DTO should:
- Give monthly feedback to the MO in-charge of the respective DMC
- Send summary of results of checklists for each DMC in the district once every quarter for analysis by the respective CMO/ DMO and IRL.
Checklist IRL OSE and NRL OSE and Feedback
- On-site quarterly evaluation report of DTCs visited by IRL team should be given to concerned State TB Officer (STO), IRL and NRL using an IRL OSE Checklist.
- OSE Checklist for NRL Laboratory Personnel to IRL is prepared using a NRL OSE Checklist.
- The IRLs will submit a consolidated quarterly report to the concerned STO and NRL. In turn, the NRL will submit a consolidated quarterly report to the Central TB Division.
- A comprehensive list of all operational elements to be observed will help to ensure consistency in laboratory evaluations and provide immediate feedback to the technicians to facilitate rapid corrective action, as well as serve as documentation of the visit and record of current conditions and actions needed.
- All potential sources of error should be investigated, including quality of stains and staining procedure, quality of microscopes, and administrative procedures that may contribute to recording errors and corrective actions provided (Figure 2).
- All problems contributing to errors must be resolved.
- Possible causes of errors, and suggested evaluation steps are provided in Annexure K.
- Remedial training must be provided for technicians unable to properly identify AFB in smears.

Figure 2: Documentation of corrective actions in IRL-OSE Checklist )RNTCP Laboratory Network Guidelines)
Action Required for IRL/NRL-OSE Checklist
A state level consolidated summary will be prepared by the respective IRL every quarter from the district summaries for submission to STO and NRL. The DTO/ CMO of the district is to submit an action taken report on the team’s recommendations to the STO within a month of the IRL visit.
Resources
RNTCP Laboratory Network Guidelines.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The IRLs submit a consolidated quarterly report of on-site visits to the concerned State TB Officer and NRL.
True
False
1
The IRLs submit a consolidated quarterly report of on-site visits to the concerned State TB Officer and NRL.
Yes
Yes
Random Blinded ReChecking [RBRC] Process
ContentAnnual slide sample and the monthly sample for Random Blinded Rechecking (RBRC) is determined by the District TB Officer (DTO), assisted by the Intermediate Reference Laboratory (IRL), Statistical Assistant (SA) or Data Entry Operator (DEO) based on Lot Quality Assurance Sampling (LQAS) method.
Under the LQAS method, sample size depends on 3 components:
- Annual Negative Slide Volume (ANSV)
- Slide Positivity Rate (SPR)
- Sensitivity of picking up lower bacili count in microscopy
Process of RBRC (Figure 1)
- The LT at each DMC stores slides for RBRC in slide boxes.
- The laboratory must store slides in a way that allows for easy retrieval of every slide identified for the rechecking sample. Therefore, all slides are to be stored in the provided slide boxes in the same order as they are listed in the laboratory register. Slides are marked as ‘a’ and ‘b’ along with the lab serial number for first spot and early morning specimen.
- The result of the smear examination must not be written on the slide.
- Removal of immersion oil is to be done using tissue paper before storing slides in a slide boxSenior TB Lab Supervisors (STLS) of the district, informing them of the total number of slides to be collected every month from each DMC.
- The STLS then select the required number of slides from the Laboratory Register and the LT records the results as per Annexure B (Figure 2).
Collection of slides for RBRC explained with an example
-
- If the sample size is calculated to be 180 smears per year, 15 slides are to be collected during each monthly visit.
- If the STLS observes that the laboratory processed 82 slides since the last monthly visit, they could collect for example every fifth (82/15 = 5.4 or 5th) slide randomly to obtain the required 15 slides and may begin with any number between 1 to 5, say 3.
- The first random number may be selected by choosing last digit on any available currency note.
- The remaining slides are chosen by adding serially 5 till 15 slides are selected.
- In this example, the 3rd, 8th, 13th, 18th, 23rd, 28th, 33rd, 38th, 43rd, 48th, 53rd, 58th, 63rd, 68th and 73rd slides are selected to obtain 15 slides required for that month.
- Annexure B (Figure 2) is then put into an envelope and sealed. The number of slides packed is written on the top of the envelope.
- Both the slide box and the envelope are marked with the name of the respective DMC, the name of the TB Unit and district, and the month and year.
- The slide box and the sealed envelope are then taken by the STLS for handing over to the DTO.

Figure 1: Process of random blinded rechecking (RBRC) performed by (1) STLS during on-site visit to DMC and (2) at DTC (RNTCP Laboratory Network Guidelines)

Figure 2: Annexure B to document Smear Results Sheet for Blinded Rechecking (RNTCP Laboratory Network Guidelines)
The DTO is responsible for ensuring that the blinding process is strictly followed.
Resources
RNTCP Laboratory Network Guidelines.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Who is responsible for ensuring that the blinding process is strictly followed?
LT
DTO
STS
STLS
2
The DTO is responsible for ensuring that the blinding process is strictly followed.
Yes
Yes
Random Blinded ReChecking [RBRC] Process at DTC
ContentRandom Blinded Rechecking (RBRC) is the process of re-reading a statistically valid sample of routine slides from a designated microscopy centre (DMC) based on lot quality assurance strategy (LQAS) in a blinded manner to assess the laboratory performance.
RBRC Process
- The district TB officer (DTO) sends information to all senior TB lab supervisors (STLS) of the district on the number of slides to be collected every month from each DMC
- The STLS then selects the required number of slides from the TB Laboratory Register and marks the RBRC selected slides in the laboratory register with a circle
- The laboratory technician (LT) fills out Annexure B (Figure 1) for the selected slides
- LT seals the filled Annexure B in an envelope and marks the slide box with the Serial No. of slides, name of the DMC and TB unit (TU), month and year
- The STLS hands over sealed envelopes and the slide box to the DTO

Figure 1: Annexure B for Blinded Rechecking of DMC Slides (RNTCP Laboratory Network Guidelines)
- The DTO with the help of the statistical assistant (SA) removes all the identifying attributes of the selected slides (including the test results). This process is called Blinding.
- Blinded re-examination of selected slides is done by the STLS of another TB Unit (TU) within the respective district. The STLS (controllers) must have demonstrated proficiency with the Ziehl-Neelsen (ZN) staining and reading method (as seen by panel testing done by Intermediate Reference Laboratory (IRL)).
- Smears may be evaluated for specimen quality (sputum versus saliva), appropriate size and thickness, and quality of staining (as per Annexure C, Figure 2).

Figure 2: Worksheet for Blinded Rechecking of DMC Slides as per Annexure C (RNTCP Laboratory Network Guidelines)
- Problems detected by the controller are noted on the form, as this information may be very useful to supervisors responsible for providing feedback to the peripheral technicians, assessing possible reasons for high false positive or false negative results, and implementing plans for retraining and corrective action.
- The DTO with the help of the statistical assistant compares the results provided by the STLS against the original results provided by the LT. This process is called Unblinding.
- The discrepant slides are sent for umpire (second controller) reading.
- All discrepant slides are re-stained and re-examined by the second controller, as there is likelihood of fading of carbol fuchsin. This rechecking of discordant slides by a second controller also acts to evaluate the performance of the first controllers.
Feedback after RBRC
- Regular and timely feedback to the DMC is essential to improve performance
- Feedback and remedial actions are provided at the end of each sampling period i.e., completion of rechecking of the annual sample
- Also, feedback is given on a monthly basis to the respective DMCs using the form in Annexure D (Figure 3) during the monthly on-site evaluation visit by the STLS responsible for the respective DMC
- Feedback includes the return of slides with discordant results to be re-read by the original LT of the respective DMC
- Potential sources of errors are investigated during the on-site evaluation visit
- Appropriate corrective actions and/or remedial training are provided within one month

Figure 3: Quality Assurance Report on Sputum Microscopy as per Annexure D (RNTCP Laboratory Network Guidelines)
Resources
RNTCP Laboratory Network Guidelines
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Who is responsible for the blinded re-examination of selected slides?
STLS of another TU
DTO
STS
LT
1
Blinded re-examination of selected slides is done by an STLS of another TU within the respective district.
Yes
Yes
External Quality Assurance for CBNAAT
ContentExternal Quality Assurance (EQA) ensures that high-quality testing can be carried out efficiently and without interruption. It involves Proficiency Testing (PT) and On-site Evaluation (OSE).
PT is an important component of EQA for Cartridge-based Nucleic Acid Test (CBNAAT) under the National TB Elimination Program (NTEP) and guarantees accurate and reproducible results.
Importance of EQA/ PT for CBNAAT
- Gives assurance to users that the instrument is functioning properly
- Checks to verify that users can correctly interpret and report results
- Verifies that there are no major errors in the process control system and that samples are identified, tested and reported correctly
- Helps to recognize major problems with an instrument or user and take remedial action
Process of EQA for CBNAAT
- EQA of CBNAAT is done using dried tube panels consisting of Mycobacterium tuberculosis (MTB) strains that are RIF resistant/ sensitive/ Non-tuberculous Mycobacteria (NTM)/ negative.
- Coordination of the EQA activity, manufacture and validation of the panels is undertaken by the National TB Institute, Bangalore.
- The process of manufacturing and validating the Dried Tube Specimen (DTS) for EQA panels involves:
- Culturing the mycobacterial strain in the liquid culture system followed by inactivation of the cultures using sample reagents
- Further incubating for 84 days for confirmation of inactivation followed by preparation of DTS panel cultures and their validation.
- Once validated, the DTS panels are dispatched to the CBNAAT sites
Each CBNAAT site receives a set of 5 tubes/ machine.
Ideally, EQA/ PT for CBNAAT is done thrice in a year/ per module/ per site.
Based on the performance of the CBNAAT laboratory, corrective actions are taken by the supervising authority such as Intermediate Reference Laboratory (IRL)/ National Reference Laboratory (NRL). During the on-site visits by the IRL and the NRL, quality indicators for CBNAAT are evaluated and corrective actions are suggested.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Monitoring of CBNAAT Quality Indicators
ContentMonitoring of quality indicators is an essential component of quality assurance for the Cartridge-based Nucleic Acid Amplification Test (CBNAAT).
- Routine monitoring of quality (performance) indicators:
- Critical element of quality assurance for any diagnostic test
- International Organisation of Standardisation (ISO) requirement
- Each testing site should collect and analyze quality indicators monthly.
- Document and investigate any unexplained change in quality indicators, such as:
- Increase in error rates
- Change in Mycobacterium tuberculosis (MTB) positivity rate or Rifampicin (Rif) resistance rate
- Significant change in volume of tests conducted
- Error rates > pre-determined threshold (>5%)
- Test turnaround time
- All unexpected trends should be reviewed by the laboratory manager and linked to corrective actions.
- Standard set of quality indicators should be used for all CBNAAT testing sites.
- System should be in place for centralized reporting of monthly quality indicators.
- Each instrument should be monitored monthly, using the following minimum set of indicators to evaluate proper use:
- Number of tests performed per month
- Number and proportion of MTB detected; Rif-resistance not detected
- Number and proportion of MTB detected; Rif-resistance detected
- Number and proportion of MTB detected, Rif-indeterminate
- Number and proportion of MTB not detected
- Number and proportion of errors
- Number and proportion of invalid results
- Number and proportion of no results
- Median time to result after receipt of the specimen
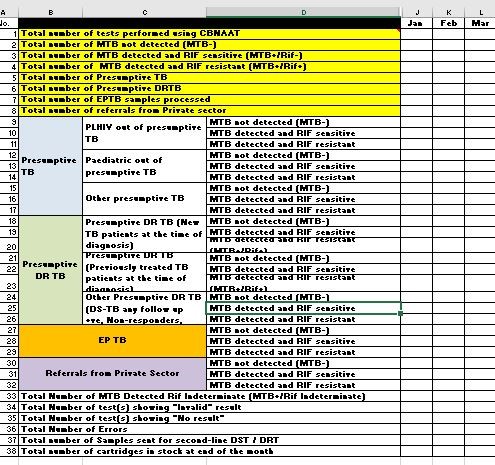
Figure: Monthly Quality Indicators for CBNAAT
Where possible, disaggregated data according to the tested population group (HIV positive, Multi-drug resistance (MDR) risk, extrapulmonary or paediatric TB) is collected.
Quality Indicator Monitoring: Troubleshooting Aid
Identifying the number and type of various errors can help with troubleshooting since certain errors may be associated with processing, instrumental or environmental conditions
The following analyses may be performed:
- The number of errors occurring by user
- The number of errors occurring by instrument module
- The number of tests lost due to power outages or surges
- The number, duration and causes of routine interruptions in the CBNAAT testing service
Video fileVideo : Monitoring of CBNAAT Quality Indicators
Resources
- Routine monitoring of quality (performance) indicators:
External Quality Assurance of TrueNAT
ContentExternal Quality Assurance (EQA) ensures quality of Truenat laboratory is maintained by comparing their results through retesting and panel testing by a higher level laboratory (Intermediate Reference Laboratory (IRL)/ National Reference Laboratory (NRL)).
EQA for Truenat laboratory is done by:
- Onsite supervision: Visits conducted at regular intervals by the IRL/ NRL/ Central TB Division (CTD)
- Proficiency Testing or Panel Testing (PT): Inter-laboratory comparisons conducted by IRL/ NRL to assess the performance of the laboratory supervised by them; re-checking of the standard panel provided by the IRL/ NRL.
- Random Blinded Re-checking (RBRC): Re-examination of randomly selected samples by the IRL/ NRL.
Plan for Truenat EQA
- Truenat EQA visits need to be conducted annually.
- Panel is provided by the National Tuberculosis Institute (NTI), Bangalore, to the participating sites.
- Participating site to conduct panel testing and report results to NTI as per timelines.
- Feedback/ corrective action provided by NTI to participating sites.
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
Monitoring Quality Indicators of Truenat
ContentMonitoring of key quality indicators or performance indicators of Truenat is important to assess the functioning of the instrument, calibration/ service requirements of the instrument, competency of the technician performing the assays and inventory management. Overall quality indicators should assess:
- Total tests done
- Type of samples tested
- Test failure
- Availability of consumables
- Turnaround time
- Specimen rejected
- External Quality Assurance (EQA) results
- Instrument downtime
Quality performance indicators should be reviewed weekly by personnel in charge of Truenat laboratory, and monthly by the Intermediate Reference Laboratory (IRL)/ National Reference Laboratory (NRL)/ Central TB Division (CTD).
Under the National Tb Elimination Programme (NTEP) the following quality indicators are to be reported monthly:
- Total number of tests performed using Truenat (including EP-TB and private sector)
- Total presumptive TB tested
- Total number of presumptive DR TB tested
- Total number of Rif indeterminate, invalid, error results
- Total number of re-tests done and results
- Total number of samples sent for First Line-Line Probe Assay (FL-LPA) and Second Line-Line Probe Assay (SL-LPA)
- Total number of chips (MTB, MTB Rif) in stock
Resources
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance.
- MolBio Diagnostics Pvt. Ltd.
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
STLS: Specimen collection and Transportation
Fullscreen-
STLS: General concepts in specimen collection & transportation
FullscreenNeed for Specimen Collection and Transportation [SCT]
ContentThe National TB Elimination Programme (NTEP) has strengthened sputum collection and transport for laboratory testing by building capacity for decentralised collection.
- The provision for sputum collection and transport is used to establish linkages for giving diagnostic access to patients who cannot reach the health facilities.
- To increase access and coverage of services, designated sputum collection centres are also established for collecting and transporting sputum to the nearby laboratory.
Presumptive TB patients attending Peripheral Health Institutions (PHIs) other than Designated Microscopic Centres (DMCs) are either referred to the nearest DMC for sputum examination or their sputum specimens are collected and transported to the DMC as per guidelines.
- The patient is given these options as per their convenience to minimise the possible delay in diagnosis and initiation of treatment or avoid repeated visits by the patient.
- In case the patient is not able to travel to the DMC, then the spot sample is collected at the nearest health facility/ sputum collection centre/ sputum collection booths and transported to the DMC.
The need for sample collection can be categorized broadly into two categories:
1. When samples are sent to the DMC
- Some PHI/ sub-centres/ health and wellness centres function as sample collection centres.
- Sputum collected from referring health facilities needs to be transported to the nearest DMC.
2. When DMC has to collect and transport samples for testing/ follow-up/ resistance testing to higher laboratories
- If the Nucleic Acid Amplification Testing (NAAT) facility is not available at the health facility, the DMC may also need to collect and send the sample to the nearest linked facility for NAAT testing.
- If NAAT is available at DMC and Mycobacterium tuberculosis (MTB) is detected, the second sample needs to be transported to the Culture and Drug Susceptibility Testing (C&DST) lab. If the NAAT result suggests rifampicin-sensitive, a second sample is sent for First-line Line Probe Assay (FL-LPA) to look for H-mono/ poly resistance.
- Extrapulmonary samples have to be appropriately collected at the PHI/HF and transported for testing to NAAT/ culture facilities.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Specimen collection and transportation system minimises patient inconveniences and diagnostic delays.
True
False
1
Specimen collection and transportation system minimises patient inconveniences and diagnostic delays.
Yes Yes Process of SCT
Content- Good quality sputum collection is of paramount importance in tuberculosis diagnosis.
- Once a person is identified as presumptive TB, s/he is referred to the Designated Microscopy Centre (DMC) for sputum collection.
- For TB diagnosis two sputum samples are collected - one is the supervised ‘spot’ sample collected at the DMC (labelled Specimen A) and the other is the early morning sample collected by patient themselves at his/her home (labelled Specimen B).
- If the patient is coming from a long distance or s/he is unlikely to return to give the second specimen, two spot specimens may be collected with a gap of at least one hour.

Figure: Flowchart for Sputum Collection and Transport
Sputum Collection
- The (NTEP) request form required for the biological specimen examination need to be filled.
- The Lab Technician (LT) should instruct the patient to thoroughly rinse the mouth with clean water and demonstrate to inhale deeply 2-3 times and cough out the sputum from the depth of the chest into a sterile 50 ml sputum container, in a well-ventilated space.
- After collecting the sputum, close the lid of the containers and wipe the surface of the tube with 5% phenol to disinfect and allow it to air dry.
- Label the tubes with patient details, date and time of collection, specimen identification, lab no. using a permanent marker.
Sputum Transport
- The sputum collected should be transported immediately to the Nucleic Acid Amplification Testing (NAAT)/ Culture and Drug Susceptibility Testing (C&DST) laboratory. In case of any unavoidable delays, the sample should be refrigerated.
- The programme mandates triple layer packaging for the transport of the sputum specimens.
- Firstly, seal the joint between the cap and neck of the sputum containers with a parafilm strip (primary receptacle package).
- Wrap the sputum containers individually in absorbent cotton, place them in a zip lock pouch and secure them with a rubber band (secondary receptacle package).
- Fold and place the NTEP request form in another zip lock pouch.
- Place the zip lock pouch with sputum containers in a thermocol box along with two pre-frozen coolant gel packs and the zip lock pouch with the NTEP request form is placed on top.
- The dimensions of the thermocol box used for sputum transport are: thickness - 2.5 cm; Outer dimensions: length - 18.5 cm, breadth - 13 cm, height - 12 cm (without lid), height -14 cm (with lid); Inner dimensions: length - 14.5 cm, breadth - 8 cm, height - 12 cm (without lid), height - 13 cm (with inner part of lid).
- The coolant gel packs should be conditioned in the deep freezer in a temperature between -20 to -15o C for a minimum 48 hours to a maximum 72 hours before use so that they can maintain a temperature between 12-20o C for up to approximately 48 hours in tightly packed thermocol boxes while the average outside temperature is 35o C.
- Seal the thermocol box with duct tape and affix ‘To’ and ‘From’ address, biohazard sticker on the box (tertiary receptacle package).
- Weight of the fully packed consignment box should be up to 400 grams and the thermocol boxes and gel packs should not be reused.
- Transport the box through NTEP identified courier/ speed post service.
Resources
- Training Module (1-4) for Programme Managers and Medical Officers, NTEP, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug-resistant TB in India, 2021.
- Module for Laboratory Technician, CTD, MoHFW, India, 2005.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test After collecting the specimen, the falcon tubes should be wiped and disinfected with which solution? 5% Iodine 5% Glycerine 5% Phenol 5% Sodium 3 After collecting the specimen, the falcon tubes should be wiped and disinfected with 5% phenol solution. Yes Yes NTEP mandates triple layer packaging for the transport of the sputum specimens
True False 1 Triple layer packaging prevents spills and leakages during transportation of sample. Yes Yes Modes of Transportation in SCT
ContentAll efforts must be made to have decentralised local arrangements for transporting the specimens to the TB detection centre (TDC). If a proper transport mechanism for collected specimen is in place, it spares the patients from travelling to the laboratory.
The sputum sample is packaged in triple layers in such a manner that it arrives at the destination in good condition and presents no hazard to the transporter.
Transporter/ personnel transporting the sample should be sensitized by the National TB Elimination Programme (NTEP) staff prior to engagement.
- Sensitisation would be provided on Symptoms of TB disease and its transmission, precautions to be taken to prevent exposure, hand hygiene requirements and spill management.
The different modes of sample transport include:
1. Post: Postal department services available pan-district can be engaged to transport sputum samples.
2. Courier: Local logistics courier companies can also be identified and hired to transport samples.
3. Volunteers/ human carriers: Community volunteers/members of NGOs can be trained as human carriers to collect and transport samples.
District TB Centre or Medical Officer TB Control (MO-TC) should ensure feasibility and financial measures required for .such arrangements for sputum transport.
Systems can be established for transportation of various biological samples (not only TB) from referring centre/peripheral centre to laboratories in a hub and spoke model in a integrated manner.
Resources
- Specimen Transportation - A How-to Guide.
- Health and Safety Guidelines for Staff/ Workers involved in Sputum Transportation, CTD.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Sputum can be transported through post/ courier/ human carriers.
True
False
1
Sputum can be transported through post/ courier/ human carriers.
Yes Yes Specimen Collection and Transportation to a DMC
ContentSputum collection centres collect, package and then transport samples to nearby TB diagnostic centres/ Designated Microscopy Centre (DMC).
Sputum is collected and packaged utilizing the triple-layer packing as per National TB Elimination Programme (NTEP) Guidelines.
Image
The Multi-purpose Health Worker (MPHW) or the Laboratory Technician (LT) at the sputum collection centre are responsible for collecting the right specimen, enrolling the presumptive TB case in Niskshay, generating Nikshay ID and testing ID for the requested test.
Sputum is transported in the sample transport box to the nearest laboratory along with the completely and correctly filled laboratory request form (along with Test ID generated through Nkshay). Sputum can be transported utilizing local volunteers, courier services, etc.
Ideally the sputum needs to be transported without delay. In case, the delay is expected, then the cold chain also needs to be maintained.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test LT at sputum collection centres enrols the patient and generates a test request on Nikshay. True False 1 LT at sputum collection centres enrols the patient and generates a test request on Nikshay. Yes Yes Cold Chain Requirement for the Transport of TB Diagnostic Specimens
ContentA cold chain is a system of transporting and storing TB specimens at optimum temperature while being transported from the peripheral health institutions to the diagnostic labs to reduce the growth of contaminating endogenous respiratory organisms.
Cold chain requirements for transportation of TB diagnostic specimens are (Figure 1):
- A thick thermocol box (one-time use box), which has a thickness of about 2.5 cm. Outer dimensions of the box - Length: 18.5 cm, Breadth: 13 cm, Height: 12 cm. Inner dimensions of the box - Length: 14.5 cm, Breadth: 8 cm, Height: 10 cm.
- Two gel packs to maintain a temperature between 12-20°C for up to approximately 48 hours in tightly packed thermocol boxes (average outside temperature 35°C). Gel packs to be conditioned in the deep freezer (temperature between -20 to -15°C) for a minimum of 48-72 hours before use.

Figure 1: Technical specifications of transport box for sputum specimen transportation in cold chain
Specimen Transport Steps - Cold Chain (Figure 2)
- Place the gel pack into the thermocol box.
- Place the sample tubes (in zip-lock pouches) on the frozen gel packs.
- Keep the pouch containing the Test Request form on top before placing another gel pack on top.
- Close the lid of the box and wrap tightly with brown duct tape to maintain the cold chain.
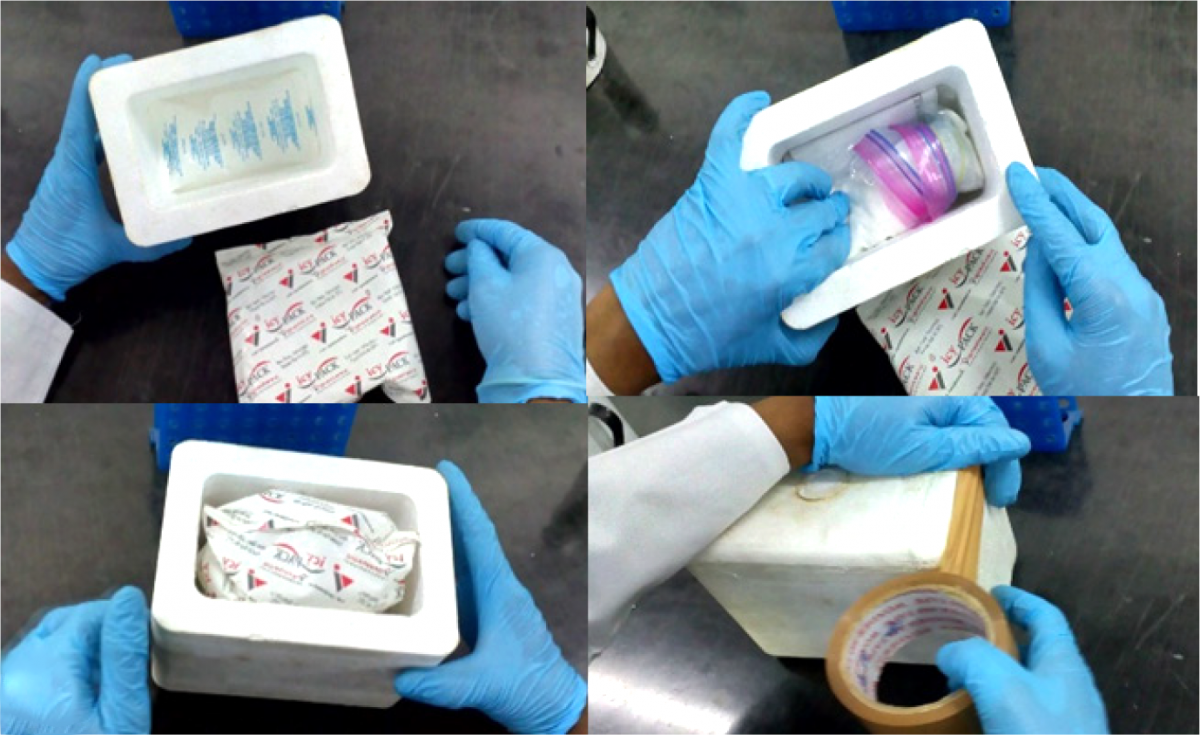
Figure 2: Steps for specimen transportation in cold chain
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Packaging & dispatching sample to a C&DST lab
FullscreenRequirements for Packaging a biological Specimen
ContentPeripheral Laboratories in the NTEP need to send biological samples (such as sputum) to nearby Culture and Drug Susceptibility Testing (CDST) laboratories for advanced testing (eg Drug Resistance Testing). The samples need to be safely packaged and transported such that there is no spillage or contamination.
The items required for safe packaging biological specimens are:
- Falcon tubes
- Three-layer packing materials like thermocol box
- Ice gel pack (pre-frozen at -20oC for 48 hours)
- Request for CDST forms
- Polythene bags
- Tissue paper roll for absorbent packing
- Parafilm tapes
- Brown tape for packing the thermocol box
- Permanent marker pen
- Labels with 'To' and 'From' address and blank labels for sample details
- Biohazard sticker
- Scissors
- Spirit swab
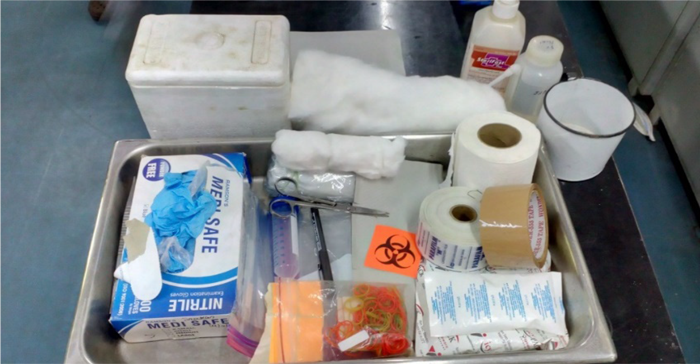
Figure: Items needed for packaging of biological specimens for CDST laboratory; Source: Guidelines for Programmatic Management of Drug Resistant TB in India, 2021
Video fileResources
Specimen Carriers
ContentTechnical specifications for TB diagnosis specimen carriers are as follows:
Thermocol Box:
- Thickness of box - 2.5 cm
- Outer dimensions: Length - 18.5 cm, breadth - 13 cm, height - 12 cm (without lid), height - 14 cm (with lid); Inner dimensions: Length - 14.5 cm, breadth - 8 cm, height - 12 cm (without lid), height - 13 cm (with inner part of lid).
Gel Pack:
- Number of gel packs required: 2
- Weight of fully packed consignment box: 400 grams
- Gel packs maintain a temperature between 12-20ºC for up to approximately 48 hours in tightly packed thermocol boxes (average outside temperature 35ºC)
- Conditioning in the deep freezer (temperature between -20 to -15ºC) for a minimum 48 hours to a maximum 72 hours before use, is required.
This is a one-time use carrier since the thermocol boxes and the gel packs are not reused.

Figure: TB Diagnostic Specimen Carrier - Thermocol Box with Gel Packs; Source: NTEP Guidelines for Programmatic Management of Drug Resistant TB in India, 2021
Resources
- Training Module (1-4) for Program Managers and Medical Officer, NTEP, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug Resistant TB in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
SOP for Packaging Specimens during the Transportation of Biological Specimens for TB Diagnosis
ContentStandard Operating Procedure (SOP) for Packaging Specimen during the transportation of biological specimens for TB diagnosis, also known as Triple Layer Packaging, is as follows:
The Lab Technicians (LTs) at the Designated Microscopy Centres (DMCs) should be trained to carefully pack the sputum samples in the cold box to avoid spillage of the samples. Before packing, personal protection measures such as wearing hand gloves (double gloves preferred), goggles and masks are to be followed by the LTs to prevent contracting the infection.
Table: Steps in Standard Operating Procedure (SOP) for Packaging Specimen during Transportation for TB Diagnosis
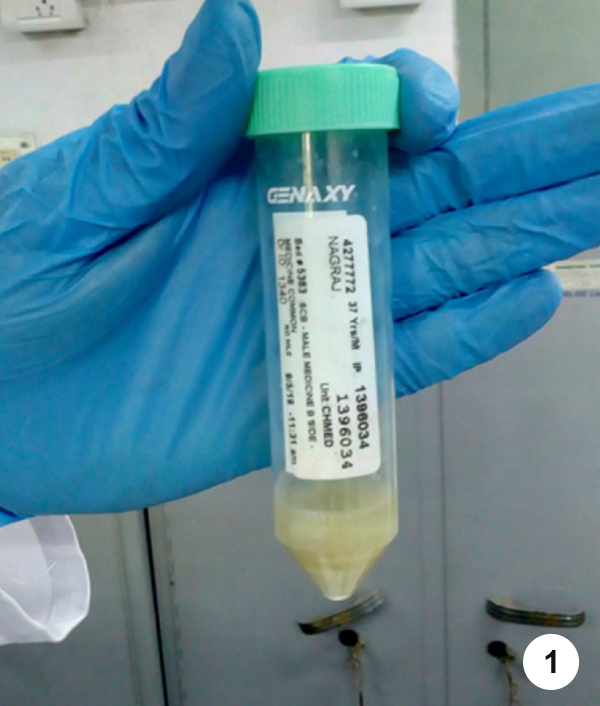
- Step 1. Make sure that the specimen collection tube is tightly closed after the sample has been collected from the patient.

- Step 2. Wipe the outer surface of the 50 ml conical tube with 5% phenol followed by absorbent tissues and allow it to air dry.

- Step 3. Write the patient details on the opaque area (white area) of the specimen collection tube using a permanent marker pen, clearly in capital letters.
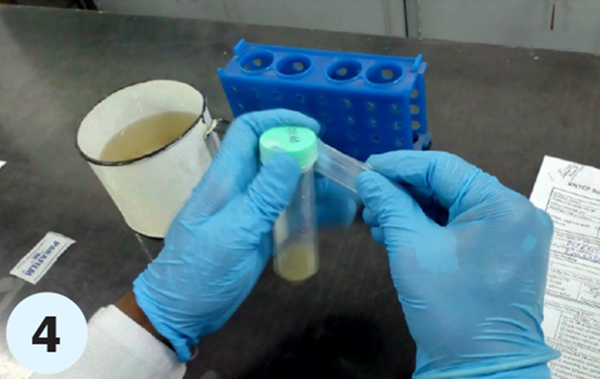
- Step 4. Cut the parafilm strip and wrap one of the strips at the joint between the cap and the neck of the specimen collection tube such that a secured seal is formed. (Primary receptacle/ package

- Step 5. Open the absorbent cotton roll and spread it out on the workbench; separate the cotton into two equal layers. Roll the specimen collection tube containing the sample tightly in the absorbent cotton such that the tube is covered completely.
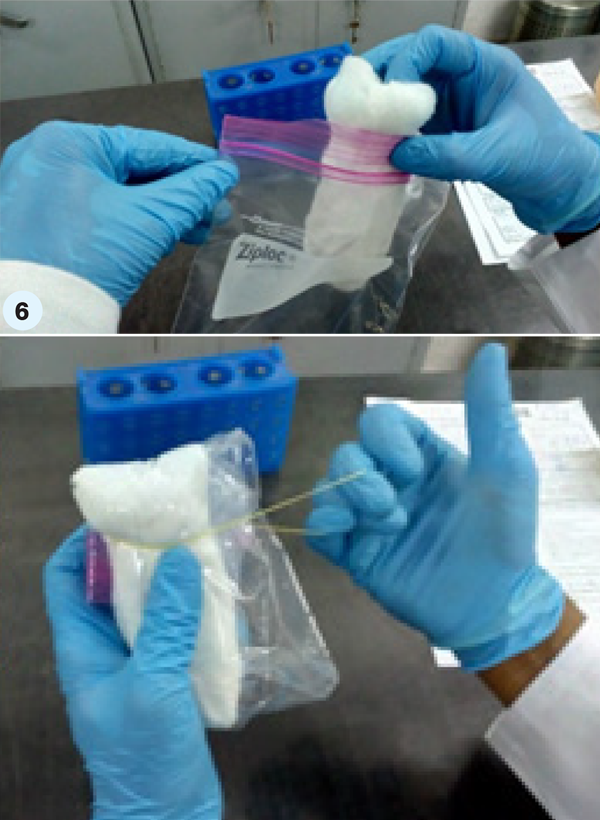
- Step 6. Put this roll containing the specimen collection tube into the ziplock pouch. Roll the whole into a tight bundle, ensuring that there is no air in the pouch. This bundle should be secured with rubber bands. (Secondary receptacle/ package)
- Step 7. Repeat steps 5–7 for the second sample of the patient.
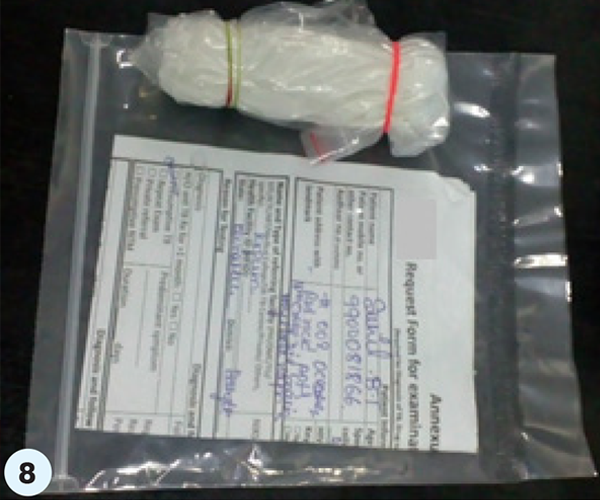
- Step 8. Insert the Test Request form printed from Nikshay into the ziplock pouch after ensuring that the details on the form and the sample tubes match, with the writing facing outside (details visible through the package). Seal the ziplock on the pouch.
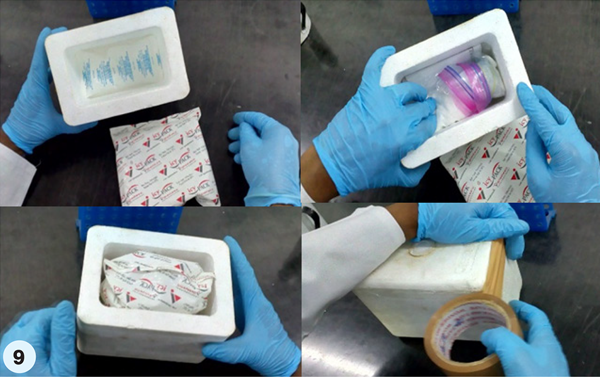
- Step 9. Place the cooled gel packs into the thermocol box, place the sample tubes packed in ziplock pouches on the frozen gel packs (frozen for 48 hours at -40°C) and also keep the pouch containing the Test Request form printed from Nikshay on top. Stick the BIOHAZARD sign over the lid and “To and From” stickers on the exterior of the thermocol box or box used to pack the specimen. Close the lid of the box and wrap it tightly with brown duct tape. (Tertiary receptacle/ package)
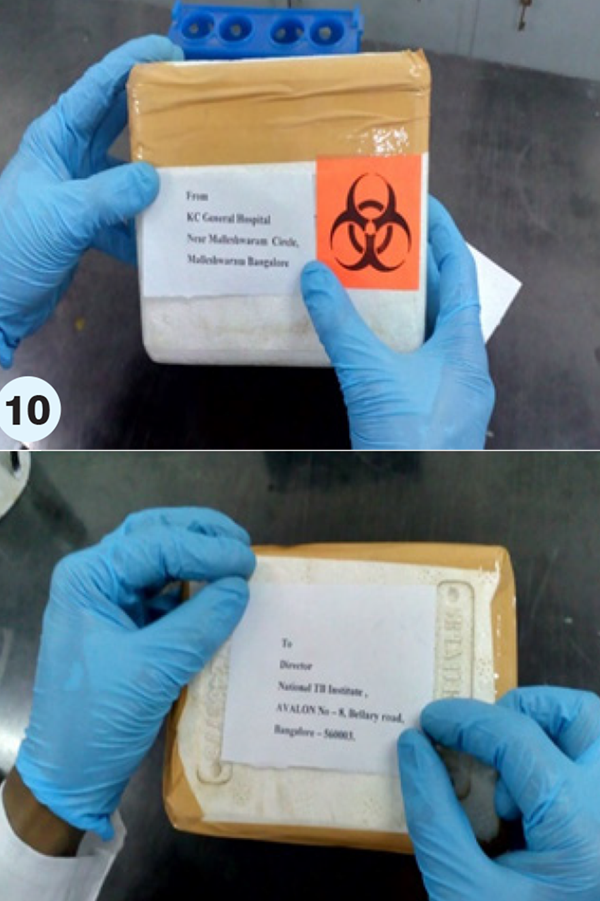
- Step 10. Complete the ‘From’ and ‘To’ addresses on the stickers, using a permanent marker pen.
The LT of the DMC should promptly inform the sample transport agency like a courier/ speed post service, or a human carrier to collect and transport the samples.
Video fileResources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug-resistant TB in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Technical Specifications for Labelling Specimen Transport Carriers
ContentThese are the technical specifications for labelling specimen transport carriers:
- Specimen containers need to be labelled legibly with details such as the patients’ name, date and time of specimen collection, TB detection centre/ District Tuberculosis Centre (DTC), lab no., specimen A or B.

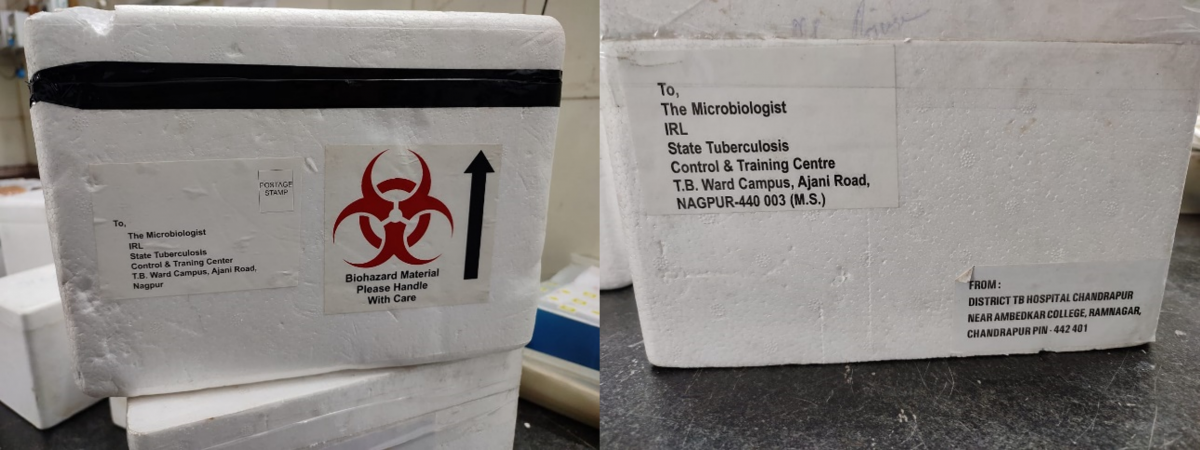
Figure: Details to be filled on the specimen containers

- Dispatch list with details of each specimen transported and the request form for examination of biological specimen for each specimen should be put in an envelope and attached to the outside box.
- As per the national guidelines for biomedical waste management, the containers used for transporting specimen samples to the National TB Elimination Programme (NTEP) - certified laboratory should be labelled with a “BIOHAZARD” sticker.

- Other than the Biohazard sticker it is mandatory to add 'To' and 'From' stickers on the specimen transportation carrier and fill in the necessary details.
- Specimen transport carriers should be labelled legibly with all the necessary details as listed above.
- A specimen may be rejected at the receiving laboratory if the specimen transport carriers are unlabelled or mislabelled.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Dispatching the sample to a C&DST Lab
ContentFor presumptive Drug-resistant TB (DR-TB) patients’, the health facility staff arranges for specimen collection from patient, packs samples as per the Standard Operating Procedure (SOP) for triple layer packaging and dispatches it for transportation in cool chain to the linked Culture and Drug Susceptibility Testing (C&DST) laboratory.
All necessary materials for specimen collection and modality for transportation need to be made available/ arranged at the Designated Microscopy Centre (DMC)/ Peripheral Health Institute (PHI) by the District TB Officer (DTO).
Steps in sample dispatch include:
- Add test details in Nikshay (Figure) to generate test requests (Test ID) for the patient’s episode ID in Nikshay.
- This will enable instant online intimation about the upcoming specimen to the C&DST laboratory.
- Complete test request form for biological specimen by adding:
- Patient information
- Details on name and type of referring facility
- Health establishment ID
- Reason for testing and test requested
- Patient ID and Test ID
- Put the appropriate address of receiving C&DST laboratory and address of health facility form where samples are dispatched on the transportation box.
- Lab Technician (LT) of the health facility should promptly inform the transport agency (courier/ speed post service) or human volunteers to collect and transport the samples.

Figure: Adding Test Details in Nikshay for Diagnosis of DR-TB; Source: Nikshay Diagnostics Training Content.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Guidelines for PMDT in India, 2021.
- Nikshay Zendesk, Nikshay Knowledge Base, Diagnostics.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Test details are added in Nikshay to generate test requests (Test ID) for the patient’s episode ID in Nikshay.
True
False
1
Test details are added in Nikshay to generate test requests (Test ID) for the patient’s episode ID in Nikshay.
Yes
Yes
- Add test details in Nikshay (Figure) to generate test requests (Test ID) for the patient’s episode ID in Nikshay.
-
-
STLS: Infection Prevention and Control [IPC]
Fullscreen-
STLS: General concepts in IPC
FullscreenThe need for IPC
ContentInfection prevention and control (IPC) practices are important in maintaining a safe environment for everyone by reducing the risk of the potential spread of disease.
IPC is a practical, evidence-based approach which prevents patients and health workers from being harmed by avoidable infection. It is relevant to health workers and patients at every single health-care encounter.
Biosafety measures along with Universal Precautions like hand hygiene, personal protective equipment, safe injections, respiratory hygiene and cough etiquette is important in IPC to address the safe handling and containment of infectious microorganisms and hazardous biological materials.
IPC is essential in TB as:
1. specific population groups have a higher risk of acquiring TB infection and progressing to disease once infected; these groups include people living with HIV, health workers and others in settings with a high risk of transmission of M. tuberculosis
2. incident cases of TB among children (aged <15 years) reflect ongoing community transmission
3. primary person-to-person transmission of drug-resistant TB (as opposed to acquired resistance) is the dominant mechanism sustaining the global transmission of drug-resistant TB
4. to prevent TB transmission, interventions are needed that reduce the concentration of infectious particles in the air and the exposure time of susceptible individuals
Resources
1. Guidelines on Airborne Infection Control in Healthcare and Other Settings.
2. WHO guidelines on tuberculosis infection prevention and control 2019 update (https://apps.who.int/iris/bitstream/handle/10665/311259/9789241550512-e…)
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Person-to-person transmission of drug-resistant TB is the dominant mechanism for transmission of drug-resistant TB.
True
False
1
Primary person-to-person transmission of drug-resistant TB (as opposed to acquired resistance) is the dominant mechanism for transmission of drug-resistant TB.
Yes
Yes
Standard Precautions for IPC
Content- Standard precautions are a group of infection control practices to reduce the risk of transmission of pathogens.
- These are based on the principle that all blood, body fluids, secretions, excretions except sweat, non-intact skin, and mucous membranes may contain
transmissible infectious agents. - Standard precautions are applicable to all patients in all healthcare settings and combine the major features of universal precautions, body substance isolation, and airborne precautions.
- Implementation of standard precautions is based on risk assessment in all healthcare activities.
Image
Figure: Elements of Standard Precautions; Source: Guidelines on Airborne Infection Control in Healthcare and Other Settings
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings
- Health-care facility recommendations for standard precaution
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following are features of standard precautions?
Universal precautions Body substance isolation
Airborne precautions All the above 4 Standard precautions combine the major features of universal precautions, body substance isolation, and airborne precautions. Yes Yes Hand Hygiene
ContentHand hygiene is one of the most important elements of infection control. The aim of hand washing is to remove transient micro-organisms, acquired through everyday tasks in the laboratory/ clinical setting, from the surface of the hands.
Good hand hygiene protects both patients and staff.
The World Health Organization (WHO) guidelines on “Hand Hygiene in Healthcare” describe five key situations where hand washing is required:
- Before touching a patient
- Before a clean or aseptic procedure
- After body fluid exposure/risk
- After touching a patient
- After touching patient surroundings
Hand hygiene includes hand washing using soaps or hand rubbing with 70% alcohol-based formulations.
Important Considerations for Hand Hygiene
- Perform hand washing with soap and water if hands are visibly soiled and after using the restroom.
- Availability of running water supply is important for hand washing.
- If resources permit, perform hand rubbing with an alcohol-based preparation.
- Ensure availability of hand hygiene products (clean water, soap, single-use clean towels, alcohol-based hand rub).
- Alcohol-based hand rubs should ideally be available at the point of care.
Technique of Hand Hygiene (Figure)
- Handwashing (40–60 sec): Wet hands and apply soap; rub all surfaces; rinse hands and dry thoroughly with a single-use towel.
- Hand rubbing (20–30 sec): Apply enough product to cover all areas of the hands; rub hands until dry

Figure: Handwashing Technique; Source: WHO Handwashing Poster
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Health-care facility recommendations for standard precaution.
- WHO Handwashing Poster.
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Hand hygiene includes which of the following? Hand washing using soaps Hand rubbing with 70% alcohol-based formulations Sterilising the hands with hot air 1 and 2 4 Hand hygiene includes hand washing using soaps and hand rubbing with 70% alcohol-based formulations. Yes Yes Respiratory Hygiene
ContentRespiratory hygiene is vital to prevent the spread of TB via aerosols and person-to-person transmission.
Respiratory hygiene includes:
-
Covering the nose/mouth with a tissue when coughing/sneezing and appropriate disposal of used tissues
- If tissues are not available, cough or sneeze into the inner elbow (upper sleeve) rather than into the hand
- Keeping contaminated hands away from the mucous membranes of the eyes and nose.
- Carrying out hand hygiene after contact with respiratory secretions and contaminated objects/materials
- Using appropriate Personal Protective Equipment (PPE) during aerosol generating procedures
- Use PPE including gloves, long-sleeved gowns, eye protection (goggles or face shields), and facial mask (or respirators) during aerosol-generating procedures

Figure: Respiratory hygiene (Ministry of Ayush, https://twitter.com/moayush/status/1243852404640153601)
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings
- Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care
- Ministry of Ayush, https://twitter.com/moayush/status/1243852404640153601
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following are critical elements in respiratory hygiene?
Covering the nose/ mouth with a tissue when coughing/ sneezing
Throwing tissues used to wipe nasal secretions on the road
Using appropriate Personal Protective Equipment (PPE) during aerosol-generating procedures
None of the above
Options 1 and 3
Covering the nose/ mouth with a tissue when coughing/ sneezing and appropriate disposal of used tissues, as well as appropriate PPE usage during aerosol-generating procedures, are important elements of respiratory hygiene.
Yes
Yes
-
General Cleaning and TB Lab Surface Decontamination
ContentThe cleanliness and regular disinfection of the TB lab and its surfaces play an essential role in the safety of those working in these labs.Guidelines for Laboratory Cleaning
- All personnel should don appropriate Personal Protective Equipment (PPE) prior to cleaning the facility.
- Laboratory personnel should perform all daily housekeeping routines within the TB laboratories, including trash removal. Cleaning staff should only enter the laboratories under the supervision of the laboratory staff.
- All the cleaning and decontamination procedures in the TB containment laboratory should be performed only by trained laboratory staff.
- Work surfaces are decontaminated when work is finished, at the end of every workday, and immediately after any spill of viable material.
- Large equipment, such as incubators and centrifuges, will have inner and outer surfaces damp-wiped with disinfectant on a routine basis.
- Sinks in the laboratories should be cleaned and flushed with agent appropriate disinfectants
- The floor of the TB containment laboratory should be thoroughly and routinely wiped down with a suitable chemical decontaminant, and workspaces that do not get daily attention should be disinfected
- Solid waste should be decontaminated by autoclaving prior to removal from the facility and disposed off by authorized personnel
Unidirectional Flow of Cleaning
- There should be an effective separation of various sections and activities of the lab to prevent cross-contamination.
- Unidirectional flow of cleaning should be maintained in specific areas.
- Cleaning items, such as mops, buckets and brushes, used in dirty areas of the laboratory should never be used in the cleaner areas.
Good Laboratory Practices to Keep Laboratories Clean and Clutter-free
- Floors and work surfaces should be kept as free of clutter as possible.
- Materials should be stored in closed cupboards, where possible.
- Excess reagents should be boxed, labelled and stored in the storeroom.
- Check spill kit contents on a monthly basis. The fresh disinfectant must be prepared each week.
- Record in the 'Laboratory Cleaning and Maintenance Logbook'.
Resources
IPC practices required at a DMC
ContentDirect sputum microscopy performed at Designated Microscopy Centres (DMC) is a relatively low-risk activity as long as safe work practices are implemented properly.The following work practices are recommended to ensure that microscopy laboratory technicians are not exposed to aerosols from sputum specimens.
1. Administrative Control at DMC
- The layout and design of the DMCs should include natural ventilation, mechanical ventilation (exhaust fan) and unidirectional airflow.
- The sputum collection area should be separated from the laboratory.
- Provisions for biomedical waste management in deep burial pits, sharps pits or appropriate disposal via the health facility biomedical waste management system.
2. Environment Control at DMC
- Doors and windows should be kept open for air exchanges.
- Sputum must be collected in a well-ventilated area with direct sunlight. It should not be collected inside the laboratories, toilets, waiting rooms, reception rooms, or any other enclosed space.
3. Personnel Level Control at DMC
- Laboratory technicians should wear laboratory coats, gloves and masks when handling sputum containers and during smear preparation and staining.
- Smears should be prepared in a well-ventilated environment near an open flame.
- Work benches should be cleaned daily with disinfectants.
- Sputum containers, applicator/ broomsticks, and used slides should be disinfected with 5% Phenol overnight before discarding.
Resources
Question Answer 1 Answer 2 Answer 3 All Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Sputum specimens can be collected in toilets.
True False 2 Sputum must be collected in a well-ventilated area with direct sunlight. It should not be collected inside the laboratories, toilets, waiting rooms, reception rooms, or any other enclosed space. Yes Yes Personal Protective Equipment [PPE] Use in TB Lab Settings
ContentWhat is Personal Protective Equipment (PPE)?PPE refers to physical barriers which are used alone or in combination to protect an individual's mucous membranes, airways, skin and clothing from contact with infectious agents, hazardous material, conditions or processes.
Components of PPE
- Protective clothing: Surgical gowns and laboratory (lab) coats
- Respiratory devices: N95 respirators
- Hand protection: Gloves
- Head protection: Headgear/ hair covers/ caps
- Foot protection: Shoe cover, safety shoes/ closed-toe shoes
- Eye protection: Safety glasses/ goggles, shields
PPE Hazard Assessment
- Evaluation of the PPE requirements for a specific activity or work environment is carried out by the lab director.
- For TB labs it is based on the risk assessment. PPE requirements will thus differ according to whether activities are classified as low risk, medium risk or high risk.
PPE Usage in Different Sections of the TB Laboratory
The table below lists the different PPE requirements for different sections of the TB lab.
Table: PPE usage in different sections of TB labs Section/ RoomPPE used/ preferredSample collection/ reception roomLab coat, gloves Smear microscopy section/ room/ Designated Microscopy Centre (DMC)Lab coat, glovesCartridge-based Nucleic Acid Amplification Test (CBNAAT) sample processing sectionLab coat, gloves, Surgical maskSample opening area(in a higher laboratory) Surgical gown, gloves and N95 respirator Media preparation room Designated lab coat, gloves, hair cover, shoe covers/ closed-toe shoes Culture reading roomLab coat, gloves, N95 respiratorLine Probe Assay (LPA) clean roomsDesignated lab coat, gloves, hair cover, shoe covers/ closed-toe shoesWalk-in cold roomLab coat, insulating gloves, shoe covers/ closed-toe shoesWalk-in incubatorLab coat, respirator and gloves, shoe covers/ closed-toe shoesCorridor inside the labLab coat, shoe cover/ closed-toe shoesDeep freezersLab coat, cryo glovesDisinfection, washing and sterilisation roomLab coat, gloves (heavy duty), insulating gloves, closed-toe shoesResources
- National Guidelines for Infection Prevention and Control in Healthcare Facilities, 2020, MoHFW, GoI.
Resources
Use of a PPE in a DMC
ContentThe use of appropriate Personal Protective Equipment (PPE) in a TB laboratory is determined by risk assessment (according to the procedure and suspected pathogen).
Designated Microscopy Centres (DMCs) are low-risk TB laboratories, hence PPE should be used as follows:
- Laboratory coats should be worn at all times by the Laboratory Technician (LT) while working in the laboratory.
- Gloves and long-sleeved laboratory coats should be used during sample collection, opening sample transport boxes, handling leaky specimen containers, smear preparation and staining smears.
- Masks are not required for use during the preparation of sputum smears in well-ventilated areas.
- LTs and support staff handling biological waste should wear gloves.
- Patients that visit DMC to provide sputum samples should be advised to wear masks.
It is advised that the laboratory should maintain adequate ventilation by keeping the windows open all the time or installing exhaust for the personal protection of the laboratory staff.
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings, MoHFW, 2010.
- Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care, WHO, 2014.
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
LTs and support staff handling biological waste should not wear gloves.
True
False
2
LTs and support staff handling biological waste should wear gloves.
Yes Yes
-
STLS: Airborne Infection Control
FullscreenAirborne Infection Control [AIC]
ContentMycobacterium tuberculosis is transmitted in airborne particles called droplet nuclei that are expelled when a person with pulmonary TB coughs, sneezes, shouts, or sings. People nearby may breathe in these bacteria and become infected.
Airborne infection control is essential to prevent the spread of TB within a health facility and other settings.
Hierarchy of Controls to Reduce Risk of Transmission of TB (see the Figure)

Figure: Hierarchy of controls to reduce risk of transmission of TB
Environmental factors that influence transmission of M. tuberculosis are elaborated in the table below.
Table: Environmental factors that influence the transmission of M. tuberculosis; Source: Tuberculosis Infection Control Factor Description Concentration of infectious bacilli The more bacilli in the air, the more probable that M. tuberculosis will be transmitted Space Exposure in small, enclosed spaces Ventilation Inadequate local or general ventilation that results in insufficient dilution or removal of infectious droplet nuclei Air circulation Recirculation of air containing infectious droplet nuclei Specimen handling Improper specimen handling procedures that generate infectious droplet nuclei Air pressure Positive air pressure in an infectious patient's room that causes M. tuberculosis organisms to flow to other areas Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control.
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The hierarchy of controls to reduce the risk of transmission of TB includes which of the following?
Environmental controls
Administrative controls
Personal protective equipment
All of the above
4
The hierarchy of controls to reduce the risk of transmission of TB includes administrative controls, environmental controls and the use of personal protective equipment.
Ventilation as an AIC Measure
ContentVentilation is defined as the supply/ distribution/ exchange or removal of air from spaces by mechanical or natural means.
Airflow is a natural process whenever there is change in temperature or pressure. Air keeps moving displacing the room air, and the time to replace the entire in-room air depends on the size of the room, the openings, and the presence of additional/mechanical force. This air-flow, also called ventilation, will allow the entry of outside air or clean recirculated air to remove extra heat, humidity and infectious aerosols from occupied spaces to meet health and comfort requirements.
When fresh air enters a room, it dilutes the concentration of particles in room air including aerosols responsible for the transmission of TB that can otherwise remain suspended in the air for significant periods of time.
Thus, ventilation is recognized as an important factor influencing the transmission of airborne diseases.
Types of Ventilation at Designated Microscopy Centres (DMCs)
1. Natural Ventilation (Figure below)
- Natural ventilation at DMCs is achieved by designing a laboratory layout that supports the unrestricted flow of natural air.
- Doors and windows should be kept open to bring in fresh air from outside.
- Opening windows and doors on opposite walls will also allow for cross ventilation.
- The placement of furniture, equipment, supplies etc. at DMCs should not block or restrict the opening of doors and windows.

Figure: Natural ventilation achieved by opening doors and windows or using mechanical ventilation using fans and an exhaust fan for air mixing and directional flow (A); the flow of natural air should not be restricted by blocking doors and windows (B); Cross ventilation is not adequate if there is only one entry point for outside air (C); Source: Tuberculosis and HIV Co-Management and Tuberculosis And Airborne Infection Control.
2. Mechanical Ventilation: When the movement of air is driven by a mechanical device, it is called mechanical ventilation.
- DMCs are equipped with fans and exhaust fans as the simplest means of mechanical ventilation for air circulation and directional flow of air. Exhaust fans fitted in windows/ ventilators exchange air from inside the laboratory to the outdoors.
- Ceiling fans/ tabletop fans/ pedestal fans have rotating blades to circulate air inside the room. Tabletop and pedestal fans can be positioned in the room to allow the directional flow of air.
3. Hybrid/ Mixed-mode Ventilation
- In hybrid/ mixed-mode ventilation exhaust and/or fans are used in DMCs in combination with natural ventilation to obtain adequate air dilution when sufficient airflow cannot be achieved by natural ventilation alone.
The table below compares the advantages and disadvantages of the different modes of ventilation.
Table: Summary of Advantages and Disadvantages of Different Types of Ventilation; Source: Guidelines on Airborne Infection Control in Healthcare and Other Settings.
Mechanical Ventilation
Natural Ventilation
Hybrid (mixed-mode) Ventilation
Advantages
Suitable for all climates and weather
Suitable for warm and temperate climates
Suitable for most climates and weather
More controlled and comfortable environment
Lower capital, operational, maintenance costs for simple implementations
Energy-saving relative to mechanical ventilation
Occupants have limited control to affect ventilation
Capable of achieving very high ventilation rates
More flexible
Disadvantages
Expensive to install and maintain
Easily affected by outdoor climate and occupants’ behaviour
May be more costly or difficult to design
Can fail to deliver required ventilation rates through faulty design, maintenance, or operation
May be difficult to plan, design, and predict performance
Noise from equipment
Reduced comfort level of occupants in extreme weather
Cannot achieve directional control of airflow, if required
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control, CDC.
- Tuberculosis and HIV Co-Management.
- Tuberculosis and Airborne Infection Control.
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In mixed-mode ventilation, exhaust and/or fans are used in combination with natural ventilation.
True
False
1
In mixed-mode ventilation, exhaust and/or fans are used in combination with natural ventilation.
Yes
Yes
Administrative measures for AIC at a Health Facility
ContentThe administrative measures at a health care facility play an important role in preventing the spread of TB in health care settings. It includes Administrative controls for outpatient and inpatient settings
Administrative measures at Outpatient(OPD) settings
1. Screen for respiratory symptoms as early as possible upon patient’s arrival at the health care facility thereby reducing the overall stay of such patients in the healthcare facility- screening at registration counter itself by asking simple questions related to chronic respiratory symptoms, and those suspected to have TB can be prioritized for further management
- screening when patients are in waiting area- by volunteers/health staff
2. Provide patient education and counseling on cough hygiene and sputum disposal
- paramedical staff or volunteers should educate and reinforce cough etiquette while the patient is in the waiting area
- educate patients on availability of bins with disinfectants for disposal of sputum
- display of posters on cough hygiene and sputum disposal in the waiting areas
3. Segregate patients with respiratory symptoms
- having separate waiting area for chest symptomatics within the overall outpatient area
- implement a patient flow control mechanism so that screened chest symptomatics are diverted to special area rather than the common waiting area
- well ventilated waiting areas to reduce overall risk of airborne transmission
4. Fast-track patients with respiratory symptoms
- fast-track patients for clinical and laboratory evaluation
- fast track chest radiography and sputum examination with priority slips/referrals
Administrative measures at Inpatient (IPD) setting
1. Minimize hospitalization of TB patients- whenever possible, manage patients entirely as outpatients thereby avoiding hospitalization and the risk of exposing other patients and staff
2. Establish separate rooms, wards, or areas within wards for TB patients
- patients with TB should be physically separated in different rooms/wards from other patients so that others are not exposed to the infectious droplet nuclei
- separation of TB patients from vulnerable and immune-compromised patients is essential
3. Educate and counsel inpatients on cough hygiene and provide adequate sputum disposal
- educate and display posters on cough hygiene and safe disposal of sputum in bins with disinfectants
- provide masks to all admitted patients and educate on proper use of masks
4. Establish safe radiology procedures for TB patients
- schedule inpatient chest radiography for non-busy times
- provide priority service to minimize the length of time spent in the department
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control.
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What of these is/are the administrative measures for airborne infection control at a health facility?
Prompt/ fast-track screening
Educating, training, and counselling
Availability of masks
All of the above
4
Administrative measures for airborne infection control at health facilities include prompt/ fast-track screening and diagnosis, education, training, and counselling, and availability of masks.
Yes
Yes
-
-
STLS: TB Treatment and care
Fullscreen-
STLS: Concepts in TB Treatment
FullscreenGoals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Strategies for TB Treatment
ContentUnder the National TB Elimination Programme (NTEP), strategies adopted in the treatment of TB are based on the available scientific and operational researches. These strategies are combined to ensure better treatment outcomes for the TB patients. The main strategies include:
Domiciliary Treatment
- This is a strategy that allows for the treatment of TB in a patient’s home.
- Domiciliary chemotherapy proved to be as effective as sanatoria treatment (which was the historical way of treating TB) and achieved higher cure rates.
- The patients having the social benefits of being at home.
Short Course Chemotherapy (SCC)
- Chemotherapy of TB underwent revolutionary changes in the 70s owing to the availability of two well-tolerated and highly effective drugs – rifampicin and pyrazinamide.
- These drugs allowed for SCC and made it possible to simplify treatment and reduce its duration without reducing the therapeutic effect.
- Now with SCC regimens, it is possible to treat and cure TB patients in 6 months.
- When given daily, these regimens are effective, achieve high cure rates, prevent the emergence of drug resistance and minimize relapses.
- The shorter duration also contributes to improvement in treatment adherence.
Directly Observed Treatment (DOT)
DOT is a method whereby a trained healthcare worker or another trained designated person (treatment supporter) watches a patient swallow each dose of anti-TB drugs and document it.
- DOT can reduce the development of drug resistance, treatment failure, or relapse after the end of treatment.
- Many patients who do not receive directly observed treatment stop taking drugs once they feel better.
- Hence, by providing DOT, the NTEP ensures that patients receive the right drugs, in the right doses, at the right intervals and for the right duration.
The modern treatment strategy is based on standardized short-course chemotherapy regimens largely administered on a domiciliary basis, utilising the DOTS strategy and proper case management to ensure completion of treatment and cure.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Treatment of Tuberculosis Disease, CDC, 2006.
- Guide on Tuberculosis Control for Primary Health Care Providers, WHO, 2015.
- Treatment of Tuberculosis: Guidelines for National Programmes, WHO, 2003.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these treatment strategies are adopted by NTEP?
Domiciliary treatment
Use of short-course chemotherapy
Directly observed treatment
All of the above
4
Strategies utilized by NTEP in TB treatment are domiciliary, short-course chemotherapeutic short-course regimens that are directly observed.
Pharmacological Basis of treatment
ContentTuberculosis treatment and its different regimens have scientific backgrounds for their formulations. To understand this, we need to know about the mode of action of each anti-TB drug first.
Mode of Action of Anti-TB Drugs
Anti-TB drugs have the following three actions:
- Early bactericidal activity: Killing of actively growing bacilli (in the phase of rapid multiplication and uninhibited metabolic activity).
- Sterilizing activity of persisting bacilli, i.e., metabolically inhibited organisms in a quasi-dormant state.
- Ability to prevent the emergence of drug resistance.
The ranking of first-line drugs with respect to their type of activity is indicated in Table 1 below.
Table 1: Ranking of first-line anti-TB drugs used in the treatment of drug-sensitive TB, based on the mode of action and activity
First-line Drugs Early Bactericidal Sterilizing Prevention of emergence of drug resistance Isoniazid (H) ++++ ++ ++++ Rifampicin (R) +++ ++++ +++ Pyrazinamide (Z) ++ +++ + Ethambutol (E) + Nil ++ Thus, each drug has unique characteristics and drug combinations will make the regimen more effective.
Need for Long Duration of Treatment of TB
- Anti-TB drugs mostly kill actively multiplying tubercle bacilli.
- When bacilli have low metabolic activity, i.e., when bacterial growth has almost come to a standstill and the organisms are “dormant”, they are not killed by otherwise bactericidal drugs. Such organisms are referred to as persisters*.
- Though they may survive in the presence of drugs, behaving as if they were drug-resistant, they are in fact susceptible to the drugs.
- Thus, if for some reason these organisms regain their ability to multiply freely, they would be killed by the very drugs that had not harmed them before.
- When dormant bacilli again become metabolically active and start multiplying during effective chemotherapy, they are soon killed.
- Once chemotherapy has been completed, the revived bacilli may continue to multiply and thus cause relapse.
- This explains why conventional chemotherapy needs to be of long duration.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the role of the intensive phase of anti-TB treatment? To reduce adverse drug reactions in patients To achieve rapid killing of actively multiplying bacillary population
To prevent the emergence of drug-resistance Options 2 and 3 4 The role of IP is to achieve rapid killing of actively multiplying bacillary population and eliminate naturally occurring drug-resistant mutants and prevent the further emergence of drug resistance. Yes Yes Which of the following drugs is bacteriostatic? Isoniazid Ethambutol Pyrazinamide Rifampicin 2 Ethambutol is an effective bacteriostatic drug, helpful in preventing the emergence of resistance to other companion drugs. Yes Yes Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentIt is extremely important for any type of TB patient to be initiated on the right treatment at the earliest in order to have better treatment outcomes. Therefore as soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen.
Steps in TB Treatment Initiation
Image
Figure: Flowchart-Treatment Initiation
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, India, 2021.
- Training Modules (1-4) for Programme Managers and Medical Officers, CTD, MoHFW, India.
Assessment
Question
Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. True False 1 The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. Yes Yes As soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen
True False 1 Soon after identification pre treatment counselling is given to patient and caregivers followed by pre treatment evaluation and treatment initiation. Yes Yes Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Adverse Drug Reactions with anti-TB Drugs
FullscreenAdverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Pharmacovigilance in NTEP
ContentPharmacovigilance is defined by the World Health Organisation (WHO) as the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problem.
- It is a fundamental public health surveillance activity to ensure patient safety measures in healthcare.
- Good pharmacovigilance will identify the risks within the shortest possible time after medicines have been marketed and help establish or identify risk factors.
Importance of Pharmacovigilance
Pharmacovigilance allows for intelligent, evidence-based prescribing with the potential for preventing many Adverse Drug Reactions (ADRs). Pharmacovigilance will help in:
- Improving patient care by assessing both the harms and benefits received from drugs (anti-tubercular treatment).
- Strengthening patient safety, safeguarding the patient’s interests and ensuring adherence to prescribed drug regimens.
- Preventing antimicrobial resistance.
Pharmacovigilance ultimately helps each patient in receiving optimum therapy at a lower cost to the health system.
Conducting Pharmacovigilance under the National TB Elimination Programme (NTEP)
The Pharmacovigilance Programme of India (PvPI) was set up by the Ministry of Health and Family Welfare, Govt. of India, in July 2010. PvPI is India’s national programme for surveillance of ADR-related information.
NTEP in collaboration with PvPI, and with support from WHO India, developed the comprehensive active Drug Safety Monitoring and Management (aDSM) system for ADR monitoring. Pharmacovigilance is prioritised in Drug-resistant TB (DR-TB) centres for drug-resistant cases.
Adverse events reporting for pharmacovigilance is done as follows:
- DR-TB centres are linked with ADR Monitoring Centres (AMC) established in medical colleges to initiate reporting of ADR in a systematic manner.
- Serious adverse events are reported to AMCs and Central TB Division (CTD) within 24 hours. This is done via a standardized suspected ADR reporting form (Annexure-11) which is filled by the treating doctor.
- The data is entered in Nikshay on a regular basis by statistical assistants at the nodal DR-TB centre and senior DR-TB TB-HIV supervisors at the district DR-TB centre.
- From Nikshay, the information is directly communicated to PvPI through a connecting bridge called Vigiflow.
- The ADR data submitted to Vigifloware is analysed by PvPI and shared with CTD on a regular basis.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Ready Reckoner for Medical Officer - Adverse Drug Reactions Associated with Anti-TB Drugs Identification and Management, 2019.
- Practical Handbook on the Pharmacovigilance of Medicines used in the Treatment of Tuberculosis, WHO, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is true concerning pharmacovigilance in NTEP?
PvPI is India’s national programme for surveillance of ADR-related information.
ADR-related information flows between Nikshay and PvPI via Vigiflow.
Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
All of the above
4
PvPI is India’s national programme for surveillance of ADR-related information, which flows between Nikshay and PvPI via Vigiflow. Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
Yes Yes
-
STLS: Documentation of Treatment
FullscreenTB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
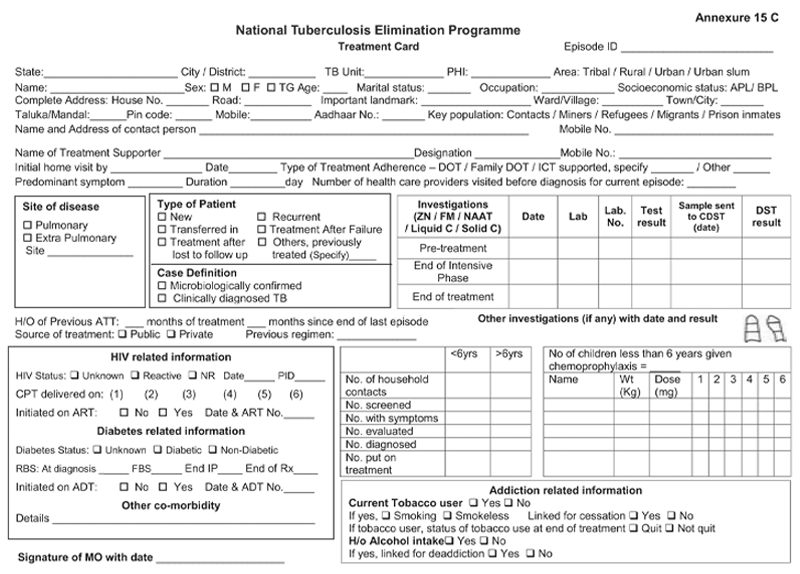
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
NTEP TB ID Card
ContentIn the National TB Elimination Programme (NTEP), the ‘NTEP TB identity card’ is provided for their identification and record of clinical follow-ups.
The identity card is completed for each patient who has a Tuberculosis (TB) Treatment Card, and it is kept with the patient. Information from the TB Treatment Card is used to complete the identity card.
There are 3 parts in the NTEP TB identity card and details in each part is delineated in Table 1.
Table 1: Parts of the NTEP TB identity card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PART
DETAILS CONTAINED IN THE SECTION
The First and Second Part
Patient information
Name and address of the TB unit/ district
Treatment details of the patient including:
- Disease classification
- Type of patient
- Treatment provider
- Case definition
- Weight bands
- Dosage
- Sputum results
- Culture results
- Results of follow-up smear examinations
- Results of follow-up cultures
- Information on the date of treatment initiation
- Treatment outcome
The Back Part
Appointment dates for visits to NTEP facilities
Contact details of NTEP staff in case of side events/queries
The information contained in this card will help to continue treatment in case the patient is transferred or admitted to any other health facility any time during the treatment period. The TB identity card is shown in Figure 1.
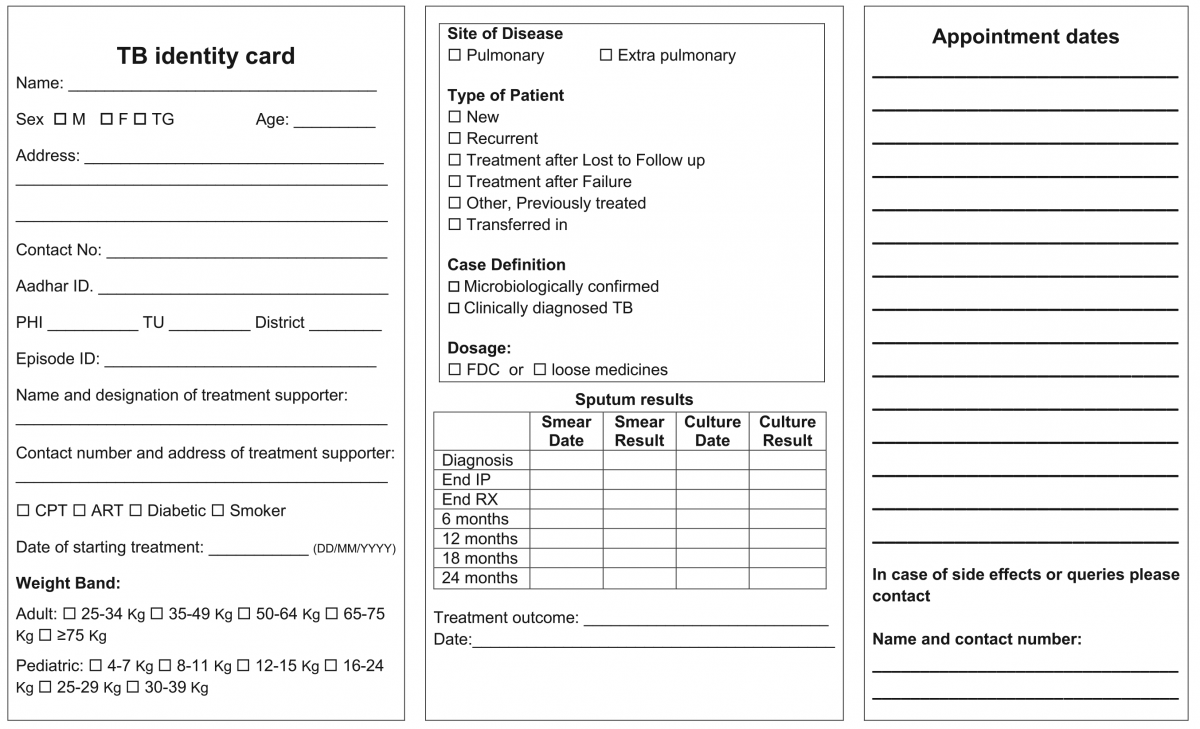
Figure 1: NTEP TB Identity Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020

Figure 2: Sample of a patient’s TB identity card


Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
-
STLS: Extra Pulmonary TB (EPTB)
FullscreenManagement of EPTB
ContentThe management principles of Extrapulmonary Tuberculosis (EPTB) are shown in the figure below.

Figure: Ten principles about what every EPTB patient in India needs as a basic standard of care
Abbr: CBNAAT:Cartridge-based Nucleic Acid AMplification Test; PTB: Pulmonary TB; NTEP: National TB Elimination Programme
Diagnosis of EP-TB
- All efforts need to be made to get a microbiological confirmation whenever a sample is available.
- Clinical diagnosis can be made by treating physician based on the clinical features, lab investigations, imaging studies and by ruling out other causes
Treatment Regimen and Duration for EPTB
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE). However, the duration of the continuation phase in EPTB may be extended in special situations such as TB Meningitis, bone and spine TB etc.
Role of Surgery in EPTB Cases
- Surgery is sometimes required for the diagnosis of EPTB. It is reserved for management of late complications of the disease.
Monitoring Treatment Response
- Response to treatment in EPTB may be best assessed clinically. Clinical follow-up is the most important criterion for the follow-up of EPTB patients. The clinician can assess the patient’s condition by checking weight gain and a decrease/ increase in presenting clinical symptoms.
- Investigations such as Acid-fast Bacilli (AFB) microscopy, chest X-ray, liver function tests, serum creatinine, and USG-abdomen can be used to monitor the treatment status.
The treatment support and other monitoring activities remain the same as for pulmonary TB.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Index TB Guidelines on Extra-pulmonary Tuberculosis for India, Central TB Division, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the standard treatment duration for most EPTB cases?
2 weeks
1 month
6 months
3 years
3
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE).
Yes Yes In which cases can the treatment duration exceed 6 months in EPTB?
TB meningitis
TB of the bone and joint
Depending on the clinician’s decision
All of the above
4
EPTB treatment duration can be extended beyond 6 months in TB meningitis, TB of bone and joint (including TB otitis media), and if recommended by the clinician.
Yes
Yes
-
STLS: Drug Sensitive TB (DS-TB)
FullscreenCategorization of DSTB Treatment Regimen
ContentDaily Regimen is prescribed for Drug Sensitive TB patients (DSTB), where the patient needs to consume the FDC formulation daily.
Daily Regimen comprises the first line Anti TB drugs based on
- Age: Adult/ Pediatric
- Weight of the patient: Weight Bands
Age: Based on age, patients are categorized into
- Adults: The patient's age should be greater than 19 years
- Paediatrics: Patient's age up to 19 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosages are based on TB patients’ weight.
- A weight band category is defined for Adults and Pediatric patients separately, and FDC are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
DS-TB Treatment – Patient Flow
ContentCommunity Health Volunteers(CHVs) have to refer the presumptive cases identified based on the r symptom screening to the nearest NTEP health facility for further investigation. Once Diagnosed with TB, the TB patients are initiated on the first-line TB treatment. Patients are also offered NAAT within a maximum of 15 days to rule out any drug resistance. If no drug resistance is detected, then the patient continues on the first-line TB treatment. TB patients are then clinically evaluated every month to check the progress of TB treatment.
The treatment duration of TB is divided into two phases - The Intensive Phase(IP) and the Continuation Phase(CP). Post-treatment completion, patients are then evaluated at intervals of 6,12,18 and 24 Months to ensure a relapse-free TB cure for the patient.
Figure: DSTB Treatment Flow
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
-
STLS: Drug Resistant TB (DR-TB)
FullscreenDrug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Screening for DR-TB
ContentAll patients diagnosed with TB should have universal access to rapid DST for at least Rifampicin and further DST for at least Fluoroquinolones among all TB patients with rifampicin resistance, i.e. UDST.
UDST tests are offered preferably before treatment initiation to a maximum within 15 days from diagnosis. Based on the UDST test result, if Rifampicin resistance is detected, the patient is shifted to DR-TB Treatment Regimen. If Rifampicin resistance is not detected, then first-line anti TB treatment is continued, and the patient is screened further on their follow-ups. If tested positive in sputum examination during any patient follow up, then sputum is sent for further drug resistance testing, and the patient is referred to PHI for follow-up.
Figure: Screening of patient for initiating DRTB Treatment from DSTB Treatment
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
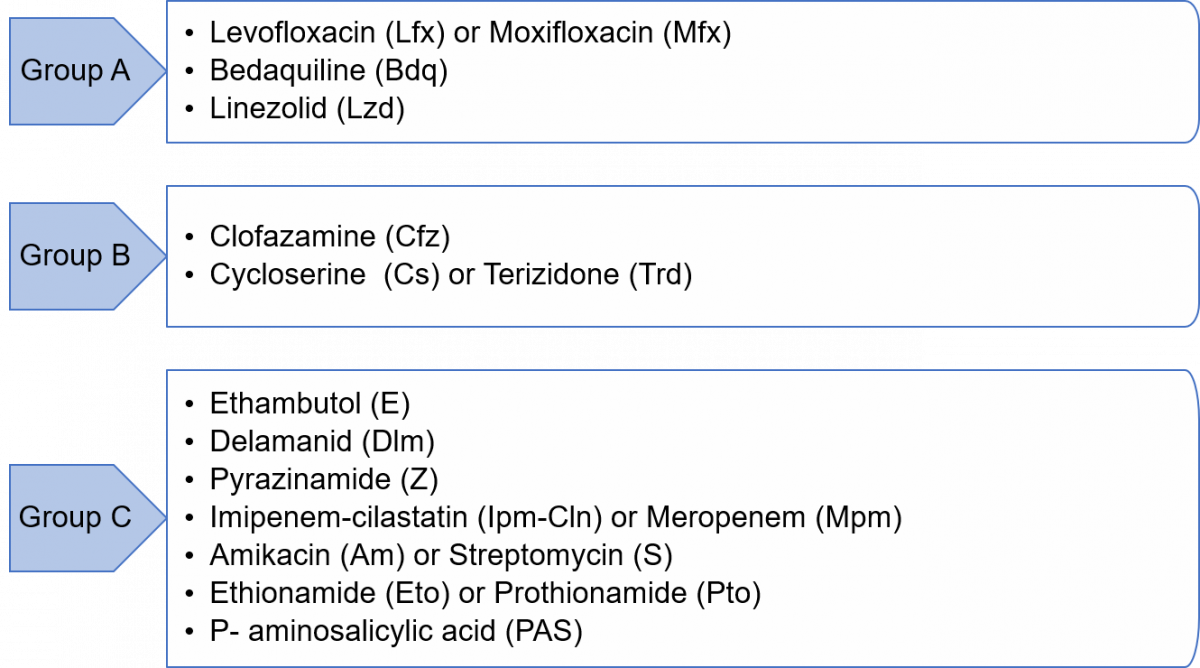
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
-
STLS: Follow up of TB patients
FullscreenFollow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
Management of Patients with Treatment Interruptions
ContentTreatment interruption is defined as a patient-initiated episode in which the patient discontinues TB treatment. All efforts must be made to ensure that TB patients do not interrupt treatment or are not lost to follow-up. Action should be taken to promptly retrieve patients who fail to come for their daily dose by the treatment supporter
The management of treatment interruptions is made based on the following criteria:
i. Type of case: Whether new, relapse or failure
ii. Duration of treatment taken: Less than one month/ more than one month. This helps in assessing the risk of the presence of drug resistance.
iii. Duration of Interruption: Less than one month/ more than a month.
If treatment interruption is more than one month, the outcome is declared as ‘lost to follow up’.
If a patient returns to the health facility after interrupting treatment for more than one month, the patient sample needs to be subjected to Drug Susceptibility Testing (DST) to determine resistance/ sensitivity status to anti-TB drugs.
In case the interruption is for less than one month, the same treatment regimen is completed to complete all doses.
Modes of Retrieval
TB treatment is supervised by a trained treatment supporter (a health worker, family member or community volunteer). The residential address is verified for all TB patients by home visits. However, in case of treatment interruption, patient retrieval action is required.
Retrieval can be done by the following modes:
1. Retrieval of patients interrupting treatment within 24 hours of discontinuation is done by the Treatment Supporter (TS) or Accredited Social Health Activist (ASHA)/ Auxilliary Nurse Midwife (ANM)/ Multipurpose Worker (MPW). The reason for interruptions should be reviewed carefully and efforts made to counsel and bring the patient back for treatment.
2. If the TS is not successful in retrieving such patients, it should be reported to the next higher level of supervisors, like Senior Treatment Supervisor (STS), and they should take all efforts to counsel and retrieve the patient.
3. If the patient interrupts treatment on more than one occasion, the Medical Officer of the Peripheral Health Institute (MO-PHI) should visit the patient’s home. The MO-PHI should give intensive counselling to the patient and may provide additional support to continue the treatment without interruption.
4. Innovative use of information and communication technologies for treatment adherence monitoring through 99 DOTS, Medication Event Reminder Monitor (MERM), etc. are also beneficial in finding missed doses and initiating retrieval action by the health staff.
Resources
1. Training Modules (1-4) for Programme Managers and Medical Officers.
2. Guidelines for PMDT in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. True False 1 If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. Yes Yes
-
STLS: Adherence monitoring
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
-
STLS: Treatment Support
FullscreenTreatment Support
ContentA person affected by TB requires support throughout the course of treatment and beyond that. The support to a TB patient is essential to ensure that s/he completes the treatment without affecting her/his quality of life (QoL). Keeping the patient as the central figure in the continuum of care, and ensuring social and personal circumstances are supportive (not only meeting immediate requirements of medical treatment) is the key to treatment support.

Figure: Key Components of Treatment Support
Resources
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, 2017.
A Patient-centred Approach to TB Care, WHO, 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
DOT is the only treatment support provided to TB patients.
True
False
2
Ensuring social and personal circumstances are supportive for treatment adherence and not just medical requirement is the key to treatment support.
Treatment Support Plan
ContentIn order to achieve TB treatment success, a good treatment support plan for the patients is essential. The National TB Elimination Programme (NTEP) recommends developing a treatment support plan for each patient at the time of treatment initiation. A holistic Treatment Support Plan (TSP) must include the following:
1) Treatment Supporter (TS) for each patient
- A Treatment Supporter (TS) who is acceptable and accessible to the patient and accountable to the health system (healthcare worker/ community volunteer/ private practitioner/ family member) identified in mutual consultation with the patient and provider during pre-treatment evaluation.
- The assigned TS should be able to receive training on drug administration, adherence monitoring, Adverse Drug Reaction (ADR) referrals etc., and perform these functions.
2) Periodic review of patient’s treatment
- Treatment Initiation counselling and monthly or need-based (in high TB burden areas) follow-up counselling to all TB patients and their family members must be included through staff who have expertise in the same, to address both bio-medical and psycho-social issues that could impact treatment.
- The TSP must also include a protocol for the field monitoring staff to capture each instance of treatment interruption and Adverse Drug Reactions, so that they can be effectively addressed before the patient turns lost to follow-up.
3) Psychosocial Support to TB patients and their families
- Counselling to the patients experiencing stigma, discrimination, marital/family discords, substance users etc. by the trained staff, and appropriate referrals for psychiatric ,de-addiction support etc. should be offered whenever required.
- The focus should be on observing, identifying and capturing above mentioned factors during treatment initiation as well as in each follow up visit.
- Home visit follow ups with consent from the patients must also be included in the TSP which may allow for better understanding and management of psycho-social issues.
- As an extension of TSP, community engagement activities which includes key persons such as politicians, religious leaders, self-help groups, TB champions etc by the TB staff is recommended to raise awareness and sensitise the communities about TB and also articulate a whole-of-society approach to ending TB.
4) Referral linkages for needy TB patients - to central and state government’s various social welfare and protection schemes and additional nutrition support services
- With the aim to eliminate catastrophic expenditure due to TB, the Government of India (GoI) has insisted on linking TB patients and households to the applicable government social welfare and protection schemes.
- The treatment supporters and the health systems staff who are in regular contact with the patients (Senior Treatment Supervisors, TB Health Visitors, District Programme Supervisors) should be trained in referral linkages so as to enable further support to the patients and their family members to avail the benefits under schemes.
- The GoI has rolled out a Direct Beneficiary Transfer (DBT) mechanism to support TB patients' nutrition (Ni-kshay Poshan Yojana) and travel during treatment whereas several state governments have also initiated certain state-specific schemes for TB patients across the country.
- Further as a part of patients treatment support, the GoI has initiated the ‘Nikshay Mitra’ campaign under the ‘Pradhan Mantri TB Mukth Bharat Abhiyan’ where in persons/companies/societies can adopt an entire block/ward to provide nutrition support to TB patients for a specific treatment period.
5) Treatment Completion Counselling
The TSP must include an end of treatment counselling for all patients, on the importance of post treatment follow ups and holistic self-care approach for leading an overall healthy life and also the ability to focus on life after TB treatment completion.
Resource- Training Modules (1-4) for Programme Managers & Medical Officers, NTEP, 2020.
- National Strategic Plan for Tuberculosis Elimination 2017-2025, RNTCP, 2017.
- Pradhan Mantri TB Mukt Bharat Abhiyaan - Guidance Document, CTD, India, 2022.
Assessment
Question Answer 1 Answer 2 Answer3 Answer 4 Correct Answer Correct explanation Only health workers can become treatment supporters for a TB patient. True False 2 Factors like acceptability, accessibility to the patient, and accountability to the health are taken into consideration when a treatment supporter is identified, and family members can also be treatment supporters and provided training by a health worker. Referral linkages for needy TB patients - to central and state government’s various social welfare and protection schemes and additional nutrition support services is part of holistic Treatment Support Plan (TSP)
True False 1 With the aim to eliminate catastrophic expenditure due to TB, the Government of India (GoI) has insisted on linking TB patients and households to the applicable government social welfare and protection schemes. Treatment supporter to TB Patient
ContentA Treatment Supporter can be any person such as a Medical Officer, MPWs, community volunteers working with the program etc. Even a patient’s relative or family member can be a Treatment Supporter.
As per NTEP guidelines, salaried NTEP/General Health System staff may also be assigned as treatment supporters for a patient. However, they will not be eligible for any honorarium.
A patient can only be linked to one treatment supporter at a time in Nikshay.
Assigning a TS
ContentAt treatment initiation a suitable Treatment Supporter has to be identified and assigned to the Patient.
How to identify a Treatment supporter for a patient
- The Treatment Supporter has to be acceptable and accessible to the patient and accountable to the health system.
- Should be identified in mutual consultation with the patient and provider, during pre-treatment evaluation.
- The Treatment Supporter can either be a healthcare worker, community worker/ volunteer, private practitioner or family member.
- Should be able to receive training on drug administration, adherence monitoring, ADR referrals etc., and perform these functions.
Assigning a Treatment Supporter to a Patient
Once the Treatment Supporter is identified, the patient records (Ni-kshay & treatment card) have to be updated by assigning the treatment supporter (prior registration in Ni-kshay is a pre-requisite) to the patient. See the steps below to assign a Treatment Supporter to the episode of a patient.
Treatment Supporters are eligible to receive the Treatment Supporters Honorarium as a Direct Benefit Transfer. However, to receive the DBT he/she should not be a salaried government employee.
NOTE:
- Only one Treatment Supporter can be assigned to an episode with status "OnTreatment" of the patient
- Treatment Supporters can be assigned by both the current PHI/ TU user.
- If required, a Treatment Supporter can be removed/ replaced by another Treatment Supporter anytime during the treatment.
Image
Figure: Steps to Assign a Treatment Supporter in Ni-kshay
Image
Figure: Screenshot Assigning a Treatment Supporter in Ni-kshay
Resources
- Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, Central TB Division, Ministry of Health & Family Welfare, India, 2021.
- Training Modules (5-9) for Programme Managers and Medical Officers, Central TB Division, Ministry of Health & Family Welfare, India, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test When should a treatment supporter be identified assigned to a patient episode ? While declaring treatment outcomes Any time while the patient is on treatment At treatment initiation When the patient is transferred 2 Treatment Supporters are to be identified and assigned to a patient at the time of treatment initiation.
Treatment Supporters can be assigned or re-assigned anytime during treatment, but this is in-case it has not been assigned before
Yes Yes A TB-HV acting as a Treatment Supporter can receive the Treatment Supporters Honorarium. TRUE FALSE 2 TB HV is a Salaried Government Employee and hence cannot receive the Treatment Supporters Honorarium. Yes Yes To assign a Treatment Supporter to a patient, which of the following are True? The Treatment Supporter needs to be registered on Ni-kshay The Treatment Supporter should be acceptable to the patient Should be able to record and monitor adherence, ADR, administer drugs, refer to the nearest Health Facility All of the above 4 Treatment Supporter needs to fulfill all the mentioned criteria. Role of TS
Treatment Support Groups
ContentTreatment Support Groups play an important role in providing treatment support to TB patients. It has been envisioned as a non-statutory body of socially responsible citizens and volunteers to provide social support to TB patients. This group goes beyond just providing treatment-related support as it also helps the community in accessing information, free and quality services and linkage to social welfare programmes without compromising confidentiality and respecting the dignity of the patient.
A good treatment support group creates a conducive environment for TB patients to access complete care without experiencing stigma and incurring out-of-pocket expenditures.

Figure: Schematic representation of the concept of treatment support groups.
Treatment Support Group (TSG): Example from Kerala
The initiative in the Pathanamthitta district of Kerala demonstrated that treatment support groups helped in minimising the loss-to-follow-up cases and better treatment outcomes. The group supported the patients in accessing information, free and quality services and social welfare programmes, thereby empowering the patients to complete the treatment successfully.
Resources
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, 2017.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation What is a treatment support group? A group of treatment supporters in the community A group of TB patients in the community A non-statutory body of citizens and volunteers to provide social support to TB patients All of the above 3 A treatment support group is a non-statutory body of citizens and volunteers to provide social support to TB patients. Nutritional Support
ContentNutrition constitutes an important part of TB Treatment. Undernutrition increases the risk of Tuberculosis (TB), and in turn, TB can lead to malnutrition. It has been demonstrated that undernutrition is a risk factor for progression from TB infection to active TB disease, and undernutrition at the time of diagnosis of active TB is a predictor of increased risk of death and TB relapse. There is, as yet, little evidence showing that additional nutrition support improves TB-specific outcomes, but low body mass index, as well as lack of adequate weight gain during TB treatment, are associated with an increased risk of TB relapse and death.
The following table illustrates the effect of undernutrition on outcomes in TB.
Effects on disease
- Increased severity of disease
- Increased risk of death
Effects on treatment
- Delayed sputum conversion
- Risk factor for drug-induced hepatotoxicity
- Malabsorption of rifampicin
- Reversion of positive cultures in Multidrug-resistant (MDR) -TB
Effects on long-term outcomes
- Increased rate of relapse
Effects on contacts
- Increased incidence in undernourished contacts
The basic recommendations to address the nutritional needs of TB patients are discussed below.
- Conducting an initial nutrition assessment of TB patients with further monitoring
- Providing ongoing counselling for patients on their nutritional status; Diet for TB patients starting treatment should include: cereals (maize, rice, sorghum, millets, etc.), pulses (peas, beans, lentils, etc.), oil, sugar, salt, animal products (canned fish, beef and cheese, dried fish), and dried skimmed milk
- Managing severe acute malnutrition according to national guidelines and WHO recommendations
- Managing moderate undernutrition for TB patients who fail to regain normal Body Mass Index (BMI) after two months of TB treatment or appear to lose weight during TB treatment and evaluating for proper treatment adherence and other comorbidities. If indicated, these patients should be provided with locally available nutrient-rich or fortified supplementary foods.
- Special categories of TB patients, such as:
- Children who are less than 5 years of age should be managed as any other children with moderate undernutrition.
- Pregnant women with active TB and patients with MDR-TB should be provided with locally available nutrient-rich or fortified supplementary foods.
6. Micronutrient supplementation for all pregnant women as well as lactating women with active TB. These women should be provided with iron and folic acid and other vitamin and minerals to complement their maternal micronutrient needs. In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
To achieve the above objectives, the guidelines for nutrition for TB patients are available and a mobile application (N-TB) is available for decision-making on nutritional support for TB patients.
Improving nutritional status at a population level is important for TB prevention which should be part of broader actions on social determinants. All efforts should be made to link TB patients for nutritional support which can be done through the existing public distribution system, local self-government or Non-governmental Organisations (NGOs)or donor agencies or through the corporate sector under Corporate Social Responsibility (CSR).
Resources
- Guideline: Nutritional Care and Support for Patients with Tuberculosis, WHO, 2013.
- Guidance Document: Nutritional Care and Support for Patients with Tuberculosis in India, MoHFW, WHO, CTD, 2017.
- Training Modules (1-4) For Programme Managers & Medical Officer NTEP, CTD, WHO, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, MoHFW, WHO, 2021.
Assessment
Question 1
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of Pre-Test
Part of Post-Test
Undernutrition doesn’t affect the outcomes of TB.
True
False
2
Undernutrition affects the outcomes of TB in terms of treatment.
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Support for deaddiction
ContentSubstance use has been one of the major reasons for non-adherence to TB treatment and therefore, the National TB Elimination Programme (NTEP) has implemented several initiatives for control and de-addiction of substance use in association with various other health programmes like the National Tobacco Control Programme (NTCP), Drug De-Addiction Programme (DDAP), etc.
NTEP has also included referral services to de-addiction facilities for TB patients as a part of the ‘Standards for TB Care in India (STCI)'.
Deaddiction Services and Linkages
- Brief substance use counselling during the pre-treatment, treatment initiation and regular follow-up counselling sessions by the trained NTEP staff.
- Referral to National Tobacco Quitline provides telephonic counselling via the toll-free number in English and Hindi languages 8 a.m. to 8 p.m. between Tuesday to Sunday.
- Referral to mCessation Programme provides evidence-based behavioural change Short Text Messages (SMSs) in English and Hindi languages on mobile phones, which include health information on tobacco use hazards, tips on quitting, and encouragement for those attempting to do so.
- Referral to nearest Tobacco cessation clinics/ centres in the government facilities.
- Referral under the Drug De-Addiction Programme (DDAP) wherein affordable, easily accessible and evidence-based treatment for all substance use disorders are provided through the government health care facilities of the Ministry of Health and Family Welfare, viz., All India Institute of Medical Sciences (AIIMS), New Delhi; Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh; National Institute of Mental Health and Neuro-Sciences (NIMHANS), Bengaluru; Dr Ram Manohar Lohia (RML) Hospital, New Delhi; AIIMS, Bhubaneswar; and Central Institute of Psychiatry (CIP), Ranchi.
Resources
- National Strategic Plan 2017-2025 for TB Elimination in India, MoHFW, India, 2017.
- National Framework for Joint TB-tobacco Collaborative Activities, MoHFW, India, 2017.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What service does the National Tobacco Quitline provide?
Telephonic counselling
Face-to-face counselling
None of the above
Both 1 & 2
1
National Tobacco Quitline: Telephonic counselling via the toll-free number in English and Hindi languages.
Yes
Yes
Support for Rehabitilation
Travel support for TB Patient
ContentEliminating the catastrophic expenditure on TB patients and their families has been an important goal of the World Health Organisation's (WHO’s) END TB strategy.
The National TB Elimination Programme (NTEP) has also attempted the same through various partnerships and one of the action plans under this strategy was to provide transport allowance to cover the TB treatment-related travel costs of the TB patients as well as their attendants.
Travel cost for Drug-resistant TB (DR-TB) patients
- Travel costs are reimbursed for DR-TB patients travelling to District or Nodal DR-TB Centre for initiation/ follow-ups/ adverse reaction management during the treatment, along with one accompanying person/ attendant.
- The reimbursement is as per actual cost per visit through public transport with a limit of up to Rs. 400 per visit within the district and up to Rs. 1000 per visit for outside district travel.
Travel cost for TB Patients in tribal/ hilly/ difficult areas
- TB Patients from tribal /hilly/difficult areas are provided with an aggregate amount of Rs. 750 as transport allowance to cover patients and the attendants' travel costs.
- Rs. 750 as a one-time payment at the time of notification.
Travel cost for Presumptive TB patients to visit District TB Centres (DTC)/ collection centres for testing
- Presumptive TB patients travelling to DTC/ collection centre are reimbursed as per actual cost with public transport.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
- Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme. Central TB Division, Ministry of Health & Family Welfare, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How much amount is provided as transport allowance to tribal/ hilly area patients and their attendants during their TB treatment
Rs.250
Rs.500
Rs.750
Rs.1000
3
Rs. 750 is provided as transport allowance to Tribal/ hilly area patients and their attendants during their TB treatment.
Yes
Yes
Linkages to Social Welfare Schemes
ContentThe government of India introduced Direct Benefit Transfer (DBT) to ensure that the benefits and subsidies are reaching the beneficiaries directly and to fasten the process. Through the process, money is directly transferred to the beneficiaries' bank account keeping the intermediary agencies and stakeholders only to manage the process of payment.
National TB Elimination Programme (NTEP) transfers all benefits to patients using the two systems:
- Nikshay
- Public Finance Management System (PFMS)
DBT Schemes available in the NTEP
Nikshay Poshan Yojana (NPY)
Objective: To provide nutritional support to TB patients at the time of notification and subsequently during the course of treatment.
Beneficiary: All unique TB patients notified on or after 1st April 2018 (including all existing TB patients under treatment for at least one month from this date).
Benefit Amount: Rs. 500 for a treatment month paid in instalments of up to Rs. 1000 as an advance.
Transport Support for TB patients in Notified Tribal Areas
Objective: To provide financial support as transport allowance for TB patients belonging to notified tribal areas (in addition to the nutritional support provided under NPY).
Beneficiary: All notified TB patients from notified tribal areas.
Benefit Amount: Rs. 750 as a one-time payment at the time of notification.
Incentives for Private Sector Providers and Informants
Objective: To provide financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by a private provider.
Beneficiary: Private providers (private practitioner, hospital, laboratory and chemist) who notify TB patients to NTEP on Nikshay.
Incentive Amount: Rs. 500 as a one-time payment on notification and Rs. 500 to a private practitioner or hospital for updating the patient’s treatment outcome.
Treatment Supporters’ Honorarium
Objective: To provide an honorarium to the treatment supporters for supporting TB patients.
Beneficiary: Community Treatment Supporters who support patients during treatment, leading to a successful outcome (cured or treatment completed).
Incentive Amount: Rs. 1,000 as a one-time payment on the update of outcome for drug-sensitive TB patients and Rs. 2,000 on completion of Intensive Phase (IP) and Rs. 3,000 on completion of Continuation Phase (CP) of treatment for drug-resistant TB patients.
Criteria/ Pre-requisites for Availing the Benefits in NTEP
- All benefits are processed for the respective beneficiary base on the rules and eligibility criteria defined above except for the treatment supporter, which needs to be manually uploaded by the TB Unit (TU) level staff.
- Beneficiary ID in Nikshay will be assigned to all patients which are unique. The benefits processed will be tracked under this ID. All beneficiaries need to register their bank details in Nikshay to enable DBT.
Treatment Supporter
A trained treatment supporter, who can be a health worker or community volunteer, will assist the patient to adhere to the drugs, provide counselling support, nutritional support, screen for adverse reactions, psycho-social support, comorbidity management and follow-up laboratory investigations.
The Treatment Support Honorarium is available as per the following eligibility:
- The treatment Supporter must be registered in Nikshay and designated as the primary Treatment Supporter.
- The linked patient must complete treatment or has to be cured.
- The treatment Supporter should not be a salaried government employee.
Resources
Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, CTD, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Only patients and treatment supporters seeking treatment in the public sector are eligible for DBT benefits.
True
False
2
Private providers are eligible for financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by them.
Free drugs and free treatment
ContentIn the National Sample Survey Office (NSSO) 68th round 2011-2012, India was reported to have the highest out-of-pocket expense on healthcare, of which over 67% was spent on drugs. Recognising the importance of essential drugs being available and accessible to the general public, the Ministry of Health & Family Welfare, Govt. of India, implemented the Free Drugs Service Initiative (FDSI) under the National Health Mission (NHM) in 2015.
Objectives
- To ensure that a set of essential drugs is made available free of cost to all those who access public health care facilities.
- To reduce the Out-of-Pocket Expenses (OOPE) of patients to support their treatment and adherence to medication.
Under this initiative, provision for obtaining free of cost essential medicines is made available through public health facilities under the National Health Mission at Primary Health Centres (PHCs), Community Health Centres (CHCs), Sub Divisional Hospitals (SDH) and District Hospitals (DHs).
Under this scheme, National TB Elimination Programme (NTEP) recommended Fixed-Dose Combination (FDC) anti-TB medicines are also available for both paediatric and adult TB patients. While most of these medicines are procured centrally, few loose drugs, especially for prophylaxis, are allowed to be procured at the state or district level at times when central supply is short.
NHM has dedicated funding for free drugs, and various levels, including Peripheral Health Institutions (PHI), are allotted preset budgets under this scheme. PHIs are supposed to procure essential drugs which are not supplied by the government-owned "General Medical Stores" from this budget. Although most of the drugs are readily provided to the PHIs, some subsidiary drugs and supplements, which are required in TB care, can be made available under this scheme. For example drugs required to treat minor adverse drug reactions, vitamins, protein supplements, expectorants, antitussives, etc.
Resources
-
Operational Guidelines - Free Drugs Service Initiative, MoHFW, GoI.
-
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, CTD, 2017.
-
Essential Medicine List for SHC & PHC Level, Ayushman Bharat - Health and Wellness Centre, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct explanation
To reduce the Out-of-Pocket Expenses (OOPE) of patients.
True
False
1
Free drug service initiative under NHM aims to reduce the Out-of-Pocket Expenses (OOPE) of patients.
PMJAY
Content
Figure: Components of Ayushman Bharat Yojana
Pradhan Mantri Jan Arogya Yojana (PM-JAY) is one of the two key components of the Ayushman Bharat Yojana launched by the Government of India as part of the National Health Policy 2017. It is one significant step toward achieving Universal Health Coverage (UHC) and Sustainable Development Goal - 3 (SDG3): Good health and well-being.
Aim
To provide health protection cover to poor and vulnerable families against financial risk arising from catastrophic health episodes.
Provisions
- Financial protection (Swasthya Suraksha) to 10.74 crore poor, deprived rural families and identified occupational categories of urban workers’ families as per the latest Socio-Economic Caste Census (SECC) data (approx. 50 crore beneficiaries). It will offer a benefit cover of Rs. 5,00,000 per family per year (on a family floater basis).
- Cover medical and hospitalisation expenses for almost all secondary care and most of the tertiary care procedures. PM-JAY has defined 1,350 medical packages covering surgery, medical and daycare treatments, including medicines, diagnostics and transport.
- To ensure that nobody is left out (especially girl child, women, children and the elderly), there will be no cap on family size and age.
- Cashless & paperless at public hospitals and empanelled private hospitals.
- Beneficiaries are not required to pay any charges for hospitalisation expenses.
- Benefit also includes pre and post-hospitalisation expenses.
- The scheme is entitlement based; the beneficiary is decided based on the family being figured in the SECC database.
Benefits for the Health Care System of the Country
- Helps to achieve UHC and SDG.
- Ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially the not-for-profit providers.
- Significantly reduces out-of-pocket expenditure for hospitalisation. Mitigates financial risk arising out of catastrophic health episodes and consequent impoverishment for poor and vulnerable families.
- Acts as a steward, align the growth of the private sector with public health goals.
- Promotes the use of evidence-based health care and cost control for improved health outcomes.
- Strengthens public health care systems through the infusion of insurance revenues.
- Enables the creation of new health infrastructure in rural, remote and under-served areas.
- Increases health expenditure by the government as a percentage of Gross Domestic Product (GDP).
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
PM-JAY benefits can be redeemed only from government hospitals.
True
False
2
PM-JAY provides cashless & paperless benefits at public hospitals and empanelled private hospitals. It ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially not-for-profit providers.
Yes
Yes
-
STLS: TB & Comorbidities and special situations
FullscreenPregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Silicosis in TB Patients
ContentSilicosis is a progressive and disabling interstitial lung disease caused by inhalation and deposition in the lungs of particles of free silica.
Mutual Risk of TB and Silicosis
- TB is a clinical complication of silicosis, called silico-tuberculosis. Silica-exposed workers with or without silicosis are at increased risk for TB. There is also an increased risk of extrapulmonary TB in individuals exposed to silica.
- The risk of a patient with silicosis developing TB is 2.8 – 3.9 times higher than a healthy individual.
- The risk of TB relapse in patients with silicosis is approximately 1.5 times higher than in patients without silicosis.
The presence of silica particles in the lung and silicosis may:
- Facilitate initiation of TB infection and progression to active TB
- Exacerbate the course and outcome of TB, including prognosis and survival
Diagnosis
The diagnosis of silicosis is made based on a history of exposure to silica accompanied by a clinical and radiological profile consistent with the disease.
Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), patients with silicosis are first screened according to the four-symptom complex to rule out/in active TB and tested for TB accordingly.
If active TB is ruled out >> Refer for Tuberculin Skin Test (TST)/ Interferon Gamma Release Assay (IGRA) >> Positive test >> Evaluate with Chest X-ray (CXR) >> Commence TB Preventive Therapy (TPT) irrespective of CXR results.
CXR often indicates TB in silicosis patients earlier than the clinical symptoms, and regular radiographic screening is required for early TB detection. Radiographic comparison of serial films is done with particular attention to:
- Rapid appearance of new opacities, symmetric nodules or consolidation and the finding of pleural effusion or excavations.
- Cavitation is the strongest indicator of probable silico-tuberculosis.
Other diagnostic tools that can help in diagnosis are:
- Chest Computed Tomography (CT) scan
- Bronchoscopy with bronchoalveolar lavage in conjunction with transbronchial biopsy
- Spirometry
Treatment and Follow-up
To keep the disease from getting worse, all silicosis patients need to eliminate any more exposure to silica. Supportive measures include the use of cough medicines, bronchodilators, oxygen therapy and pulmonary rehabilitation.
TB treatment in patients with silicosis is challenging, perhaps due to impairment of macrophage function by free silica and/or poor drug penetration into fibrotic nodules. Usual anti-TB drugs with directly observed therapy are recommended but for an extended duration of at least 8 months, to reduce the chances of relapse.
Follow-up of patients with silicosis and TB follow the same schedule as is in prevailing guidelines.
Prevention
TB prevention in silicosis patients is essential and includes:
- Active surveillance of vulnerable groups including workers
- Adoption of measures to reduce exposure to silica dust
- Patients with silicosis are eligible for TPT after ruling out active TB
NTEP is in the process of engaging with the Ministry of Labour and Mining to identify high priority districts with stone crushing units/ mining industry. Specific guidelines will be developed to support persons with an occupational risk for TB and provide access, diagnosis and treatment services from the programme.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Silico-tuberculosis, Silicosis and Other Respiratory Morbidities Among Sandstone Mine-workers in Rajasthan - A Cross-sectional Study, Saranya Rajavel et al., 2020.
- Mini-review: Silico-tuberculosis; Massimiliano Lanzafame et al, 2021.
- Immunity to the Dual Threat of Silica Exposure and Mycobacterium tuberculosis, Petr Konečný et al., 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about silicosis and TB is/are incorrect?
TB is a clinical complication of silicosis, called silico-tuberculosis.
Silica-exposed workers with or without silicosis are at increased risk for TB and EPTB.
TB in patients with silicosis is easily diagnosed clinically as the patient coughs up silica particles.
TB treatment in patients with silicosis is often of extended duration to prevent relapse.
3
Clinical diagnosis of active TB superimposed on silicosis is often difficult, particularly in the initial phases, when clinical manifestations may not be indicative and radiological alterations can be indistinguishable from those due to the pre-existing silicosis.
Yes Yes Cancer in TB patients
ContentRelationship between Cancer and Tuberculosis (TB)
TB and malignancy may be related in the following four ways:
- TB as a marker for occult cancer: Occult cancer may lead to locally-reduced infection barriers and/or generalised immunosuppression, rendering a cancer patient susceptible to TB infection/ reactivation.
- TB as a risk factor for cancer: TB may increase the risk of cancer locally and systemically through chronic inflammation, fibrosis and production of carcinogenic molecules.
- Shared risk factors for TB and some cancers: Shared risk factors such as smoking, alcoholism, Chronic Obstructive Pulmonary Disease (COPD) and immunosuppression, including HIV, may lead to both TB and cancer, affecting both prevalent and subsequent cancer risk.
- Treatment of cancer-fueling TB: Many cancers are treated with immunosuppressants or steroids. These drugs might induce immunosuppression in the patients undergoing treatment for cancer and hence, a flare-up of TB.
Mutual Risk of Cancer and TB
- TB patients are 2-11 times more likely than non-TB patients to develop lung cancer, according to studies.
- After cancer diagnosis, the incidence of TB also increases, both in the short term and long-term.
- All types of cancer increase the risk of the development of active TB, but with varying degrees. Haematologic cancer patients had the highest rates of active TB, followed by head and neck cancers, lung cancer and breast cancer patients.
There is intrinsic immunosuppression due to the cancer itself, immunosuppressive effects of chemotherapy, or other host factors (e.g., smoking, malnutrition) that may increase the susceptibility to both cancer and TB. Thus, there is increased incidence of TB in cancer patients, and vice-versa.
Diagnosis of TB in Cancer Patients: Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), cancer patients are first screened according to the four-symptom complex to rule out/in active TB and all presumptive TB cases need to undergo testing for TB.
Co-existence of TB and cancer poses a diagnostic challenge since clinical and radiological presentations between TB and cancers are similar, hence the need for bidirectional screening. E.g., if biopsy specimens reveal infiltration by malignant cells, still send sample for microbiological confirmation of M. tuberculosis. Thus, allowing for accurate diagnosis and initiation of anti-TB treatment instead of attributing clinical deterioration to chemotherapy complications and progression of underlying malignancy.
Diagnosis of lung cancer in TB patients is usually done in consultation with a clinical specialist and can include examination of induced sputum specimens for malignant cells, as well as use of other diagnostic tools such as Computed Tomography (CT) scans, bronchoscopy, Positron Emission Tomography (PET) scans, Magnetic Resonance Imaging (MRI), histopathology and the use of biological markers.
Treatment
TB treatment in cancer patients uses the standard DS-TB/DR-TB regimens and course, except that the treating physician should assess the drug interactions between anti-TB and anti-cancer drugs. For cancer treatment, drugs may have to be modified to accommodate anti-TB treatment and to aid better prognosis of the TB outcome. However, all decisions must be taken by a competent specialist after examining the individual case.
Curative resection, chemotherapy and radiation therapy are the mainstay treatment options for cancer in TB patients. Co-existence of TB in cancer patients necessitates anti-TB treatment with extended duration, if required. Follow-up during and after treatment also follows prevailing guidelines.
Prevention
Under the NTEP, TB prevention in cancer patients is essential and includes:
- Regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-Tumour Necrosis Factor (TNF) medicines.
- Education and referral of patients who do not have TB symptoms for TB infection testing/assessment of their eligibility for TPT.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis and Risk of Cancer: A Danish Nationwide Cohort Study, D. F. Simonsen et al., International Journal of Tuberculosis and Lung Diseases, The Union, 2014.
- Increased Risk of Active Tuberculosis after Cancer Diagnosis, Dennis F. Simonsen et al., Journal of Infection, 2017.
- Pulmonary Tuberculosis as Differential Diagnosis of Lung Cancer; MLB Bhatt et al., South Asian Journal of Cancer, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about cancer and TB is/are incorrect?
Under NTEP, regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-TNF medicines is done.
TB increases the risk of developing cancer, but cancer patients do not usually get TB.
Sputum smear microscopy is important when diagnosing TB in cancer patients.
All of the above
2
There is mutual risk between cancer and TB. TB increases the risk of developing cancer, and cancer patients are more likely to develop TB.
Yes Yes COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
-
STLS: TB Preventive Treatment
FullscreenTB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes Target groups for TPT
ContentThe NTEP has prioritized the target population for TPT based on elevated risk of progression from infection to TB disease or increased likelihood of exposure to TB disease.
The target populations have been divided into two groups:
- Household contacts of bacteriologically confirmed pulmonary TB patients notified in Nikshay from public and private sector.
Target Population
Strategy
- People living with HIV (+ ART)
- Adults and children >12 months
- Infants <12 months with HIV in contact with active TB
- HHC below 5 years of pulmonary* TB patients
TPT to all after ruling out active TB disease - HHC 5 years and above of pulmonary* TB patients#
TPT among TBI positive# after ruling out TB disease #Chest X Ray (CXR) and TBI testing would be offered wherever available, but TPT must not be deferred in their absence
*Bacteriologically confirmed pulmonary TB patients to be prioritized for enumeration of the target population for TPT
- Expanded to other risk groups
Target Population
Strategy
Individuals who are:
- on immunosuppressive therapy
- having silicosis
- on anti-TNF treatment
- on dialysis
- preparing for organ or hematologic transplantation
TPT after ruling out TB disease among TBI positive Cascade of Care for TPT
ContentIn the cascade of care approach, all target populations (People Living with HIV (PLHIV), Household Contacts (HHCs) and other such groups) who are at risk of developing TB disease are systematically reached out, screened for TB disease and after ruling out active TB disease, provided TB Preventive Treatment (TPT) as a part of the continuum of care.
The cascade of care approach among TPT target populations is shown in Figure 1.
Image
Figure 1: Cascade of TB Preventive Treatment; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment, p3.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is the correct TPT cascade of care? Offer upfront CBNAAT to all at-risk populations, then offer TPT based on the results. Identify at-risk populations, then offer TPT to all the people that have been identified. Identify target populations at risk of developing TB, screen them, rule-out active TB disease, and provide TPT to eligible populations. None of the above 3 The TPT cascade of care is: Identify target populations at risk of developing TB disease, screen them for TB disease, rule-out active TB disease, and provide TPT to eligible populations. Approaches for TPT implementation
ContentThere are two programmatic approaches for Tuberculosis Preventive Therapy (TPT) implementation:
1. Test-and-treat approach – This approach aims to detect TB infection among key groups for implementing TPT.
- After ruling out active TB, the beneficiary is tested for TB infection.
- TPT is offered only to those with a positive test (Interferon Gamma Release Assay (IGRA)/ Tuberculin Skin Test (TST)/ Cutaneous TB (C-TB))
2. Treat-only approach – For certain groups, like People Living with HIV (PLHIV) and House Hold Contacts (HHC) < 5 years old, detecting TB infection is not required. Hence, this approach is given.
- After ruling out active TB, TPT is offered without testing for TB infection.
Test and treat approach*
- HHC of sputum positive Pulmonary TB >/= 5 years old
- Individuals on:
- Immunosuppressive therapy
- Having silicosis
- On anti-TumourTNF treatment
- On dialysis
- Preparing for solid organ or haematopoietic stem cell transplantation
Treat-only approach
- HHC of sputum positive Pulmonary TB (PTB) < 5 years old
- PLHIV#
*All efforts should be made to make IGRA available. However, TPT should not be withheld in case of non-availability of IGRA.
#PLHIV < 1 year old are offered TPT only if they are a household contact of an active TB case.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following category of TPT beneficiaries is offered TPT without IGRA testing?
Household contacts of sputum positive PTB >/= 5 years old
PLHIV
Patient on dialysis
Silicosis patient
2
PLHIV and HHC of sputum positive PTB < 5 years old are offered TPT without testing for IGRA. This is called Treat-only approach.
Yes
Yes
Counselling for IGRA/TST
ContentInterferon Gamma Release Assay (IGRA) and Tuberculin Skin Tests (TST) are performed on individuals who are ruled out for active TB disease.
However, positive and negative tests in IGRA and TST do not necessarily mean the patient does or does not have Tuberculosis Infection (TBI) as the possibility of false positives and false negatives cannot be ruled out in these tests.
Importance of Counselling in IGRA/ TST
- All patients who undergo IGRA/ TST are already aware that they do not have an active TB disease and hence counselling is important to help them make informed decisions about undergoing IGRA/ TST for detecting TBI.
- Additionally, at the time of receiving positive IGRA/ TST results, they may be symptom-free or otherwise healthy. In such cases, resistance/denial to receive a prophylactic treatment like TB Preventive Therapy (TPT) is higher as its treatment course duration also is relatively longer.
- Counselling in IGRA/ TST is of utmost importance when the respective person belongs to the high-risk population and needs to be necessarily initiated on TPT and thus needs to be counselled for the same.
Components of Counselling in IGRA/ TST
- Information on TBI
- Need for undergoing IGRA/ TST
- Importance of initiating TPT post-IGRA/ TST tests
- If initiated on treatment, then schedule of medication
- Medication adherence support
- Follow-up
- Importance of completing the TPT course, adverse events
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India, CTD, MoHFW, India, 2021.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, CTD, MoHFW, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Counselling for IGRA/ TST should necessarily include which of the following?
Counselling on DR-TB
Counselling on TB Infection (TBI)
Counselling on DBT
None of the above
2
Counselling for IGRA/ TST should necessarily include ‘Counselling on TB infection (TBI)’.
Yes
Yes
Counselling for TPT
ContentCounselling is of paramount importance for TB Preventive Treatment (TPT) initiation and completion as most of the target population screened and found eligible would know that they do not have TB disease, would be symptom-free or otherwise healthy and would not feel the need to take any treatment, especially Household Contacts (HHC).
Stakeholders Involved in Counselling for TPT (Figure below)

Figure: Stakeholders involved in counselling for TPT
Abbr: HWCs: Health and Wellness Centres; PHC: Primary Health Centre; ICTC: Integrated Counselling and Testing Centres; ART: Anti-retroviral Therapy; PLHIV: People Living with HIV
Components of Counselling for TPT
While counselling the person and family members, the treating doctors/ staff must follow the steps outlined in the table below for an effective counselling session.
Component
Actions to be taken
Confidentiality
Ensure confidentiality when seeking a person’s commitment to complete the course before initiating TPT.
Information
Provide information on:
- TB infection
- Need for TPT and protective benefits to the individual, household and wider community
- TPT is available free of charge under National Tuberculosis Elimination Programme (NTEP)
- TPT regimen prescribed, including duration, schedule of medication collection, and directions on how to take the medications
- Potential side-effects and adverse events involved and what to do in the event of various side-effects. People treated with rifamycins should be alerted in advance about the pink discolouration of secretions due to this medicine
- Importance of completing the full course of TPT
- Reasons and schedule of regular clinical and laboratory follow-up for treatment and monitoring
- Signs and symptoms of TB and advise on steps if they develop them
Medication adherence support
Agree on the best way to support treatment adherence, including the most suitable location for drug intake and the need for a treatment supporter, if required.
Family support
Involve family members and caregivers in health education when possible.
Openness
Invite clarification questions and provide clear and simple answers.
Information, Education and Communication materials
- Provide information materials in the local language and at the appropriate literacy level of the person concerned.
- Reinforce supportive educational messages at each contact during treatment.
Call support (in case of emergencies)
Provide a telephone number of the HCW staff/ TB Health Visitors and Senior Treatment Supervisors concerned to call for other queries or a need to contact health services for advice.
The National TB Elimination Programme (NTEP) national call centre (NIKSHAY SAMPARK – Toll-free number 1800116666) may be provided to index TB patients, those initiated on TPT and family members to serve as a resource for information, counselling and troubleshooting as required to enable TPT initiation, follow-up monitoring and completion.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following people are involved when counselling for TPT?
Index TB patients
Caregivers
Family members
All of the above
4
When counselling persons eligible for TPT, it is best to involve the index TB patients, their families and caregivers.
Yes Yes Monitoring adherence to TPT
ContentTo achieve high treatment completion rates and the desired epidemiological impact of the TB Preventive Treatment (TPT), monitoring TPT treatment adherence, including management of missed doses and Adverse Drug Reactions (ADRs), is of paramount importance under the National TB Elimination Programme (NTEP).
Significance of Monitoring Adherence to TPT
Adherence to the TPT course and treatment completion are important determinants of clinical benefit, both at the individual and population levels as:
- Irregular or inadequate treatment reduces the protective efficacy of the TPT regimen.
- Poor adherence or early cessation of TPT can potentially increase the risk of the individual developing TB, including drug-resistant TB.
- Efficacy of TPT is greatest if at least 80% of the doses are taken within the duration of the regimen. The total number of doses taken is also a key determinant of the extent of TB prevention.

Figure: Strategies to Promote Adherence
Prevent TB India App and Integration with Nikshay as a Monitoring Tool
- Currently, under the NTEP, the person’s lifecycle approach and TB treatment episode level are recorded in Nikshay.
- TPT information management is integrated with this existing Nikshay approach. This includes information on screening, testing, eligibility assessment, TPT initiation, adherence monitoring and follow-up till treatment completion.
- The NTEP has adapted the World Health Organisation (WHO) Prevent TB India app and hosted it on Nikshay as an interim solution till the Nikshay TPT module is developed and fully functional.
- Health workers or treatment supporters will make entries directly into the app.
- The TPT monitoring dashboard can be accessed by various levels of supervisors using their respective Nikshay login ids using a link provided in the Nikshay Reports section on TPT Reports.
- A web-based comprehensive dashboard for Prevent TB initiative is also available at https://ltbi.nikshay.in/ltbi-generic-new/#/
Table: Roles of Stakeholders in Monitoring Adherence to TPT Role
Stakeholder
Treatment support and adherence monitoring including entry of daily doses taken in the Prevent TB India app/ Nikshay TPT module.
Community volunteers (TB survivors/ champions, Accredited Social Health Activists (ASHAs) and Anganwadi Workers)
- Regularly undertake home visits or tele/ video calls to monitor TPT adherence.
- Identify treatment interruptions at the earliest (Dashboards of Prevent TB India app/ Nikshay TPT module may be checked every week along with pill counting).
- HWCs/ sub-centre/ urban health posts (Community Health Officers (CHOs), Auxillary Nurse Midwives (ANMs), multipurpose workers and other field staff)
- Primary Health Centres (PHCs)/ Urban PHCs/ Private clinic (Medical Officers (MO), staff nurse)
- Adherence support and clinical monitoring through the concerned PHC/ sub-centre.
- Supportive supervision and handholding support to field level facilities and frontline workers, ASHAs and community volunteers on digital recording, using Prevent TB India app and monitoring TPT and follow-up examinations.
TB Unit (MO, Laboratory Technicians (LTs), staff nurse, pharmacist, counsellor (if available), Senior Treatment Supervisors (STS), Senior TB Laboroary Supervisors (STLS), TB Health Visitors (TBHV))
Ensuring adherence support for People Living with HIV (PLHIV) on TPT through mechanisms such as outreach workers, PLHIV networks, peer support groups, etc.
Anti Retroviral Therapy (ART) centre/ Link ART centre (MO, pharmacist, (institutional) staff nurse, counsellor, care coordinator)
Monitor and support adherence to TPT.
Tertiary care/ Medical colleges/ Corporate hospitals/ District hospitals/ Dialysis/ Cancer facilities (doctors, staff nurses)
Review data updating in Prevent TB India app/ Nikshay TPT module wherever available, check the quality of data regularly and provide feedback to TPT treatment supporters and for retrieval of TPT interrupters.
Supervisory staff at all health facilities including the State/ District TB cell (State TB Officers (STO), District TB Officers (DTO), State/ District Programme Coordinators)
Resources:
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment.
- Prevent TB Dashboard.
- Prevent TB India Mobile App.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which tools are used to monitor TPT adherence under the NTEP?
Video calls
Counting empty blisters
Directly asking the patient
Options 1 and 2
4
TPT adherence monitoring tools include direct observation of drug intake, 99DOTS/ MERM, counting empty blisters, tele/ video calls and refill monitoring.
Which of the following apps are currently used by NTEP to monitor TPT adherence?
TB Aarogya Sathi
Prevent TB India App
TPT app for NTEP
None of the above
2
NTEP has adapted the WHO Prevent TB India app and hosted it on Nikshay to monitor the entire TPT care cascade, including TPT adherence.
-
-
STLS: Public Health Action
Fullscreen-
STLS: Public health actions for TB
FullscreenPublic Health Actions
ContentPublic Health Action is conducted under the NTEP programme to support and prevent further health complications among TB patients after diagnosis.
Figure: Various activities under Public Health Action
Contact Tracing and Investigation
ContentContact tracing is a process to identify people who are at a high risk of developing TB due to their contact with a known TB case.
The aim of contact tracing is to find other people with TB disease and those infected with TB
All close contacts, especially household contacts of a Pulmonary TB patient, should be screened for TB.
In paediatric TB patients, reverse contact tracing for the search of any active TB case in the child's household must be undertaken.
Particular attention should be paid to contacts with the highest susceptibility to TB infection.
Figure: Contacts to be Prioritized for contact TB screening
TB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Socio economic factors affecting TB patients
ContentSocio-economic factors affecting TB patients are:
1. General socioeconomic conditions of the society, culture and environment. This includes:
-
Gross Domestic Product (GDP)
-
Immigration
-
Urbanisation
-
Incidence of TB in the country
-
Labour policy
-
Access to healthcare
2. Socioeconomic position of the individual. This includes:
-
Income
-
Education
-
Occupation
-
Social class/ caste
-
Indigenous/ tribal population
-
Gender
3. Living and working conditions. This includes:
-
Housing conditions (overcrowding and poor ventilation especially in night shelters, de-addiction centres, old age homes, prisons)
-
Employment conditions - Occupation with risk of developing TB (mines, coal industry, sand blasting industries, weaving & glass industries, stone-crushers, cotton mill workers, tea garden workers, rice mill workers, etc.,)
-
Homelessness
-
Hard to reach areas
-
Urban slums
3. Psychosocial risk factors, such as:
-
Social exclusion
-
Depression
4. Individual lifestyle risk factors, such as:
-
Smoking
-
Alcohol abuse
-
Tobbaco use
-
Drug abuse
-
Nutrition (malnutrition)
-
Co-morbidities like diabetes mellitus, malignancies, patients on dialysis and on long term immunosuppressant therapy HIV, past history of TB
Resources
- NTEP Training Modules (1 to 4) for Programme Managers & Medical Officers, CTD, 2020.
- Social Determinants of Tuberculosis Context Framework and the Way Forward to Ending TB in India, IPH, India, 2020.
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Socio-economic factors affecting TB patients are:
-
Housing
-
Income
-
Access to healthcare
-
Alcohol abuse
1,2
2,3,4
1,2,3,4
1,2,4
3
TB is one of the few diseases which reflects and expresses social inequalities. Living conditions, economic conditions, lifestyle, and access, affordability, and availability of healthcare are factors which affect TB patients.
-
Stigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Palliative Care in TB patients
ContentPalliative care is specialised medical care for people living with a serious illness.
- This type of care is focused on providing relief from the symptoms and stress of the illness.
- The goal is to improve the quality of life for both the patient and the family.
- Palliative care is based on the needs of the patient, not on the patient’s prognosis.
Need for Palliative Care for TB Patients
TB is, and should be, a curable disease; however, each year an increasing number of patients acquire or develop drug-resistant TB (DR-TB), which has a much lower cure rate.
While the expectations are to have increasing numbers of treatment success rates, DR-TB remains a life-threatening condition with high mortality.
The life-threatening nature of DR-TB and the burden of disease management in terms of symptoms, adverse treatment effects, adherence, stigma and subsequent discrimination and social isolation, clearly show the need for care that addresses physical, social and emotional suffering by patients.
Thus, the need for palliative care is being increasingly recognised as an important part of the continuum of care for DR-TB patients.
Challenges in Palliative Care
At present, there is a scarcity of trained health workers and local community-based palliative care resources in the settings that are most in need. Although clinical expertise in palliative care for patients who die in respiratory distress has developed considerably, individuals with DR-TB are yet to see the benefits.
Services under Palliative Care for TB
- Addressing pain and symptom control (including respiratory insufficiency)
- Nutritional support
- Medical intervention after treatment cessation
- Ensuring the appropriate place of care, preventive care, infection control and end-of-life care
Supportive Measures in Palliative Care
Image
Resources
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Palliative care is based on a patient’s prognosis.
True
False
2
Palliative care is based on the needs of the patient, not on the patient’s prognosis.
YES
YES
Patients' charter for TB care
ContentThe Patients’ Charter for Tuberculosis Care (the Charter) outlines the rights and responsibilities of people with TB. It empowers people affected by TB and their communities through this knowledge. Initiated and developed by persons affected by TB from around the world, the Charter makes the relationship with healthcare providers a mutually beneficial one.
The Charter sets out ways in which people affected by TB, the community, health providers (both private and public), and governments can work as partners in a positive and open relationship with a view to improve TB care and enhance the effectiveness of the healthcare process.
It allows for all parties to be held more accountable to each other, fostering mutual interaction and a positive partnership.
Principles of the Patients’ Charter for TB Care
- The charter practices the principle of Greater Involvement of People with TB (GIPT).
- This affirms that the empowerment of people with the disease is the catalyst for effective collaboration with health providers and authorities and is essential to victory in the fight to end TB.
Parts of the Patients’ Charter for TB Care
There are two main parts in the patients’ charter for TB care which cover:
- Patients’ rights
- Patients’ responsibilities
These parts are further delineated in Tables 1 and 2 below.
Table 1: Patient's Rights According to the Patient's Charter for TB Care Rights Explanation of rights: You, as the patient, have the right to: Care - Free and equitable TB quality care meeting the International Standards of Tuberculosis Care (ISTC)
- Benefit from community-care programmes
Dignity - Be treated with respect and dignity
- Social support of the family, community and national programmes
Information - Information about available care services — be informed about condition and treatment, know drug names, dosage and side-effects
- Access your medical records in the local language
- Have peer support and voluntary counselling
Choice - A second medical opinion, with access to medical records
- Refuse surgery if drug treatment is at all possible
- Refuse to participate in research studies
Confidence - Have your privacy, culture and religious beliefs respected
- Keep your health conditions confidential
- Care in facilities that practice effective infection control
Justice - File a complaint about care, and have a response
- Appeal unjust decisions to a higher authority
- Vote for accountable local and national patient representatives
Organization - Join or organise peer support groups, clubs and Non-governmental Organisations (NGOs)
- Participate in policy-making in TB programmes
Security - Job security, from diagnosis through to cure
- Food coupons or supplements, if required
- Access to quality-assured drugs and diagnostics
Table 2: Patients' Responsibilities According to the Patients' Charter for TB Care Responsibilities Explanation of responsibilities: You, the patient, have the responsibility to: Share information - Inform healthcare staff all about your condition
- Tell staff about your contacts with family, friends, etc.
- Inform family and friends and share your TB knowledge
Contribute to community health - Encourage others to be tested for TB if they show symptoms
- Be considerate of care providers and other patients
- Assist family and neighbours to complete treatment
Follow treatment - Follow the prescribed plan of treatment
- Tell staff of any difficulties with treatment
Solidarity - Show solidarity with all other patients
- Empower yourself and your community
- Join the fight against TB in your country
Resources
- The Patients’ Charter for Tuberculosis Care, The Global Plan to Stop TB 2006-2015.
- Capacity-building of Affected Communities for Accelerated Response to Drug-resistant Tuberculosis in the South-east Asia Region, WHO, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test According to the Patients' Charter for TB Care, it is not the patient’s responsibility to support other patients. True False 2 According to the Patients' Charter for TB Care, patients have a responsibility to support other patients, show solidarity and empower their communities. Yes Yes
-
-
STLS: Supply Chain Management
Fullscreen-
STLS: Supply Chain Management in NTEP
FullscreenSupply Chain Management
ContentSupply Chain Management (SCM) is the handing of flow of goods and material from point of origin to point of consumption, with the objective to ensure that the supplies are present for utilization without any interruption. It covers everything from procurement and sourcing of raw materials to delivery of final product to the consumer, along with the related logistics. It will also include the related information systems that enable monitoring and exchange of information.
Effective SCM ensures the following:
- Continuous availability of quality-assured medicines/ products at the right time and at all healthcare levels.
- Minimizes wastage by preventing expiry of drugs at all levels, maintenance of adequate stock levels and accurate records.
- Maximizes patient care by coordination in all departments and by minimizing human errors/ medication errors.
- Economically viable by minimizing monetary loss (e.g., through pilferage) and optimizing cost via bulk purchasing or according to consumption needs.
Robust supply chain management systems have two main components:
- Physical flow: Involved the movement and storage of supplies
- Information flow: Allows the various stakeholders to coordinate and control the flow of supplies
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant TB, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements are correct about supply chain management?
It is useful to ensure a continuous supply of good quality medicines.
It is an essential activity that must be undertaken by health programmes.
It helps reduce the cost burden on the healthcare system.
All of the above
4
Effective SCM is an essential activity that ensures a continuous supply of good quality medicines and cost optimization.
Principles of Supply Chain Management
ContentTo ensure successful implementation, sustainability and quality services under the National TB Elimination Programme (NTEP), some guiding principles in Supply Chain Management (SCM) and drug logistics are to be ensured. These are showcased in the figure below.

Figure: Principles of SCM under NTEP
Important Points
- Timely procurement, uninterrupted supply and maintenance of stock and in-time distribution of anti-TB drugs and other consumables are essential for quality services.
- Monitoring of drug supply from the central to peripheral health institute level through web-based real-time software, Nikshay-Aushadhi, is crucial to avoid under-stocking (and delays in treatment initiation) and over-stocking (resulting in wastages).
- Maintaining appropriate storage and stacking norms i.e., different batches of drugs with different dates of manufacture and expiry are stored separately so as to facilitate First-expiry-first-out (FEFO) principles, viz., drug batches with the most recent expiry are issued first.
Under FEFO, the storekeeper at the drug store is responsible for:
- Installing appropriate tools to periodically monitor controls over the expiry position of drugs.
- Exercising prudence in the case of short-expiry drugs, wherein distribution is on a rational basis that considers the utilization pattern. This includes the following:
- The storekeeper marks ‘Expiry Dates’ in Bold Letters 3” to 4” in size, on the drug cartons with a marker pen, for easy identification and control of drugs immediately on their arrival.
- Routine monitoring of the stock position of all drugs.
- Maintaining proper records.
- Analyzing shelf-life analysis of drug stocks at all levels regularly.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant TB, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is FEFO?
FEFO is the division that manages drug receipts under NTEP.
FEFO is a supply chain principle that is used to forecast consumables that are required by the programme.
FEFO means First-expiry-first-out and it is a principle to be followed when issuing drugs/ consumables.
None of the above
3
FEFO means First-expiry-first-out and it is a principle to be followed when issuing drugs/ consumables.
Drug distribution flow
ContentUnder the National TB Elimination Programme (NTEP), the anti-TB drugs are procured at the centre level by the Central TB Division (CTD), Ministry of Health and Family Welfare (MoHFW), and supplied to the central warehouses.
From the central level warehouses, the drugs are supplied to different State Drug Stores (SDS) and further distributed to District Drug Stores (DDS) and sub-district level (TB Unit (TU) Store and Peripheral Health Institute (PHI)).
This movement of drug flow is monitored in real-time through Ni-kshay Aushadhi.

Figure: Flowchart Showing the Overview of Distribution of Drugs
Abbr: CMSS: Central Medical Services Society; GDF: Global Drug Facility; CTD: Central TB Division; GMSD: Government Medical Store Depot; SDS: State Drug Store; DDS: District Drug Store; TU: TB Unit; PHC: Primary Health Centre; PHI: Peripheral Health Institute.
Resources
Process flow for SCM
ContentRegular, accurate information on consumption, drug stock and supplies at the Peripheral Health Institute (PHI), Tuberculosis Units (TUs), districts and state levels are essential for timely drug stock indenting and distribution at all levels.
The anti-TB drugs are mostly procured centrally, except for very few drugs, and supplied according to a stocking norm to various level stocking units, based on indenting.
These indentings are further dependent on the certain levels of stocks predefined for each level.
The overall idea is to ensure a working and a buffer stock at each level for ensuring uninterrupted drug delivery to the beneficiaries.
Drug Distribution Process
Image
Figure: Drug Distribution Process
Abbr: CTD: Central TB Division; GMSD: Government Medical Supplies Depot; CMSS: Central Medical Services Society; SDS: State Drug Store; DDS: District Drug Store; TU: TB Unit; PHC: Public Health Centre; PHI: Peripheral Health Institute.
Indenting
Indenting is a process in which the requisition for stocks is submitted by the sub-store to the parent store or to the supplier in order to initiate the process of drug supply from the parent store to the sub-store.
The stock management up to the TU level, including transfer to PHI, is handled by Ni-kshay Aushadhi software, while PHI to the patient is handled by Ni-kshay.
Offline Indenting
- The PHIs submit their drug request to the TU through offline indenting modes such as email, phone, etc.
- On receipt of the offline indent, the respective TU releases drugs to the PHI through the TU login in Ni-kshay Aushadhi using "Dispatch without drug request” under the Issue/ Dispatch module.
Online Indenting
- Online indenting is the term used when the indent request is placed through the Ni-kshay Aushadhi software.
- The supply of drugs from the central to the state level and further to districts and TUs is facilitated through online indenting.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How is the online indenting process done?
Through Phone
Through e-mail
Through Physical visit
Through Ni-kshay Aushadhi
4
Online indenting is the term used when the indent request is placed through the Ni-kshay Aushadhi software.
Yes
Yes
Procurement- Definition
ContentProcurement refers to the process by which governments and state-owned enterprises purchase goods and services from the private sector.
Procurement” means acquisition by way of purchase, lease, license or otherwise, either using public funds or any other source of funds (e.g. grant, loans, gifts, private investment etc.) of goods, works or services or any combination thereof.
Resources
1. Manual for procurement of goods; Ministry of Finance, GoI 2017.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What does procurement include? Buying and process of buying Tendering Acquiring goods from an external source All of the above 4 Procurement refers to the process by which governments and state-owned enterprises purchase goods and services from the private sector. Yes Yes Types of Procurement Processes
ContentFigure: Different types of Procurements
Overview and Process of Procurement
Content
Figure: Procurement Process
Resources
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Procurement process involves Need assessment Bid Invitation
Bid Evaluation
Contract execution& Disposal of scrap
All of the above
Procurement process involves Need assessment
Bid Invitation
Bid Evaluation
Contract execution& Disposal of scrap
Yes
Yes
z
What is GeM
ContentGeM stands for Government e-Market Place. It is the digital eCommerce portal for the procurement and selling of goods and services by the Government of India.

Fig 1: Logo of GeM
Source:https://gem.gov.in
- Government e-Marketplace (GeM) facilitates online procurement of common-use goods & services required by various government departments/organisations / public sector units (PSUs).
- GeM aims to enhance transparency, efficiency and speed in public procurement.
- It provides the tools of e-bidding, reverses e-auction and demand aggregation to facilitate the government users to achieve the best value for their money.
Significance
GeM is a completely paperless, cashless and system driven e-marketplace that enables procurement of common-use goods and services with minimal human interface.
It aims at:
- Instituting a unified procurement policy to encourage behavioural change and drive reform
- Establishing a lean, dynamic organisation capable of continuous innovation and market-driven decision making
- Building an easy-to-use, fully automated platform to ensure transparency and efficiency in procurement
- Demonstrating commitment to delivering value by ensuring the right quality at the right price
- Creating a sustainable ecosystem covering all stakeholders and driving inclusive development in India
Resources
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What are the advantages of GeM? Paperless procurement processes Cashless procurement processes 1& 2 None 3 GeM is a completely paperless, cashless and system-driven eMarketplace that enables procurement of common-use goods and services with minimal human interface.
Yes Yes Processes in GeM
ContentDepending upon the total value of procurement, the GeM platform provides three primary buying modes:

Direct purchase:
Direct purchase enables buyers to buy products of value up to INR 25,000 that meet the requisite quality, specifications, and delivery period without comparison (except automobiles) through any available sellers on GeM.
Direct purchase with L1
The Direct Purchase with L1 is used for mid-value (INR 25,000 to 50,000) transactions and allows the buyer to directly procure from the L1 seller after comparing all available sellers on the platform that meet the requisite quality, specification and delivery period as specified by the buyer. The comparison must be made between goods/services of at least three different manufacturers/Original Equipment Manufacturers (OEMs) and three different sellers.
E-Bid/ Reverse Auction
The E-bid/Reverse Auction mode allows buyers to conduct an electronic bid for the goods and services on the platform. The creation of bid documents as well as system-driven evaluation, are driven through well-defined and standardized technical parameters. The GeM platform shall provide buyers with the option to customize the bid, as per their requirements by way of objective selections.
Proprietary Article Certificate (PAC) Buying
The GeM platform allows buyers to procure on a proprietary basis by using the PAC filter provided on the GeM platform, which allows the selection of a specific model/makes from a particular seller that is available on the platform.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who hosts the GeM portal Ministry of Health and Family welfare Central TB Division Directorate General of Supplies and Goods Ministry of commerce 3 GeM portal is hosted by the Directorate General of Supplies and Goods. YES YES Direct Procurement through GeM
ContentDirect purchase enables a buyer to buy services of value up to Rs. 25,000, which meets the requisite quality, specifications and delivery period without comparison(except automobiles), through any of the available sellers on the Government e-Marketplace (GeM) portal.
Steps include:
1.Login to the GeM portal as a buyer

2. Click on Market--> Services

3. Select the service required

4. Check 'Service Level Agreement'

5. Select consignee location and number of resources. Fill in contract dates.

6. Fill in delivery details

7. Can view different service providers

8. Apply filters

9.'Add to Cart' the required one

10. Review cart and proceed

11. Preview Formula

12.

13. Click on 'Direct Purchase' to proceed

14. Click 'Confirm'

15. Enter the 'Reason for Choosing the Seller'

16.

17. Enter 'Financial Details'

18.

19.

20.

21.

22.

Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which service/s are eligible for direct procurement through GeM? Services of value above Rs 1 lakh Services of value up to Rs. 25,000
None of the above
All of the above
2
Direct Purchase enables a buyer to buy services of value up to Rs. 25,000 (except automobiles) through any of the available sellers on GeM.
Floating Tender through GeM
ContentA tender is an invitation to bid for a project or accept a formal offer. Tender is a process on its own; bidding is just a step towards applying for the tender and getting it.
The process of floating a tender through the Government e-Marketplace (GeM) portal has the following steps:
Step 1: Login to the GeM portal using your credentials

Figure 1: Logging into GeM portal
Source: GeM portal
Step 2: Search for the desired product
On logging in, a “Search” option is available at the top section of the same. Click on the “Categories” section of the site and select the product or click on the “search” option and enter the product's name.

Figure 2: Options to search for the desired product
Source: GeM portal
Step 3: Choose the desired product
After searching, product/products will come under the L1 category. If you want to buy items which are made in India, click on the “Made in India” section. However, before you can bid on something, you will need to compare the same with others. This enables you to find the best offering available under the amount of money you are willing to spend.
For this, click on the “Compare” option first. Various other similar options come up on the screen. Compare them side by side.

Figure 3: Comparing products and selecting the desired one
Source: GeM portal
Step 4: Bid on the product
Once the comparison procedure is done, tap on the “Add to Cart” option available under the product. A new window will open; tap on the “Proceed to Checkout” option. Select the “Bidding” option.

Figure 4: Proceed to checkout
Source: GeM portal

Figure 5: Select the‘ Bidding’ option
Source: GeM portal
Step 5: Entering bid details and finalizing
On selecting the “Bidding" option, the bid details page opens. Fill in all details and create the bid.

Figure 6: Bid details page
Source: GeM portal

Figure 7: Create a bid
Source: GeM portal
Review the terms and conditions and click “Finalize Bid”.

Figure 8: Finalizing bid
Source: GeM portal
The bid is generated and details are displayed.

Figure 9: Successful bid creation
Source: GeM portal
On clicking the bid number, you can anytime review the bid- cancel or extend it.

Figure 10: Review of bid
Source: GeM portal
Resources
GeM portal https://gem.gov.in/
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
GeM portal has the option to select ‘Made in India’ products. True False
1
If you want to buy items which are made in India, click on the “Made in India” section.
Yes
Yes
Buffer Stocks
Storage norms
ContentTo preserve the quality of medicines, good storage practices should be in place at all levels, which requires that staff are appropriately trained and storage conditions adequate.
General Guidelines on Storage of Drugs
Mechanisms to improve TB stock management in central or peripheral drug stores are:
- Stock rotation follows a First-expiry, First-out (FEFO) approach.
- The cleanliness of the area is ensured.
- The environment of the warehouse protects medicines from factors that could inhibit their effectiveness or use, such as sunlight, heat, cold, moisture, pests and theft.
- The stock area is divided into zones for easy location of different products.
- There is a designated area for second-line TB medicines.
Storage Guidelines under the National TB Elimination Programme (NTEP)
Under NTEP, space requirements change at the state, district and peripheral levels according to the NTEP stocking norms, but all other requirements remain the same as shown in the table below. The State TB Officer (STO)/ District TB Officer (DTO) must ensure that the pharmacist/ storekeeper adheres to the following guidelines on the proper storage of drugs.
Table: Guidelines for the Storage of Anti-TB Drugs in NTEP Drug Stores
Space Requirements at the State Drog Store (SDS)
- For every ten lakh population, provision should be made for the storage of about 45 cartons (of 20 boxes each), of Patient-wise Boxes (PWBs) for new cases (PC-1) and PWBs for retreatment cases (PC-2) taken together.
- This is approximately equivalent to 6 months requirement of drugs. For this volume of drugs, the minimum space requirement may be approximated as 50 cubic feet.
- For loose drugs, space provision would be 10% of space allocated to PC-1 and PC-2 PWB cartons. These could alternatively be stored in cupboards/ almirahs where volumes are low and should be kept under lock and key. Do not stack drug cartons on the floor or on top of one another.
Room Requirements
- The store should preferably comprise one large room. Where multiple rooms exist, these should be contiguous or proximate to each other.
- The ceiling must have a height of at least 5 metres.
- There should be a lockable door and at least one window with a grill and wire meshing.
- Properly lit with extra light points for plugging in the required office equipment.
- An even-level, ‘pukka’ floor.
Stacking Requirements
- Ensure that different drug/ consumable items are clearly segregated and stacked on separate racks.
- Different batches of drugs with different dates of manufacture and expiry are stored separately to facilitate FEFO principles (drug batches with the most recent expiry are issued first)
- Mark ‘Expiry Dates’ in Bold Letters 3” to 4” in size, on the drug cartons with a marker pen, for easy identification and control of drugs immediately on their arrival.
- Separate and dispose of damaged or expired products without delay as soon as approval of the same has been received, according to the biomedical waste guidelines.
Temperature and Humidity Control
- To keep humidity levels below the maximum 60% recommended for storage of drugs ensure appropriate ventilation and air circulation, and do not open cartons/ drug boxes unless necessary.
- Hydro thermometers are to be installed up to TB Unit (TU) drug store levels to monitor humidity and temperature regularly.
- Overhead exhaust fan required.
- Plastered walls and ceiling with whitewash without any kind of seepage in the room.
- The store should be clean, dry and well-ventilated.
- Ceiling and sidewalls should preferably be insulated, ensuring that the ambient temperature during peak summer does not result in damage to anti-TB drugs. The ambient temperature may be taken as 15-25°C or depending on climatic conditions, up to 30°C.
- PWBs/ cartons should be placed on shelves ensuring that there is sufficient space between shelves and walls of the storeroom.
- A regular power supply should be available for air conditioning.
Protection from Sunlight
- Shade the windows or use curtains if they are in direct sunlight.
- Keep products in cartons/ drug boxes.
- Do not store or pack products in sunlight.
- Maintain trees around the premises of the drug store to help provide shade and cooling. Check their condition regularly to prevent any untoward incidents.
Fire Safety
Ensure that the fire safety equipment is available and accessible, and that personnel are trained to use it.
Others
- Store medical supplies separately, away from rodents, insecticides, chemicals, old files, office supplies and other materials.
- Stores should not have any odour or indications of contamination and should be sanitised periodically including pest control measures.
Resources
- NTEP Training Modules (5-9) for Programme Managers & Medical Officers, 2020.
- Standard Operating Procedures Manual for State Drug Stores, NTEP, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Concerning storage of anti-TB drugs, which of the following is correct?
Stock rotation follows a First-expiry, First-out (FEFO) approach.
Store drugs away from direct sunlight.
Hydro thermometers are to be installed up to TU drug store levels to monitor humidity and temperature regularly.
All of the above
4
Appropriate anti-TB drug storage conditions include keeping drugs away from direct sunlight, maintaining appropriate temperature and humidity and following a FEFO approach.
Yes Yes Ni-kshay Aushadhi
ContentNi-kshay Aushadhi is a web-based portal that deals with the management of stocks (anti-TB drugs, consumables and other commodities) across all the stocking points across the National TB Elimination Programme (NTEP), i.e., Government Medical Store Depot (GMSD), Central Medical Services Society (CMSS) warehouses, State Drug Stores (SDS), District Drug Stores (DDS), TB Units (TUs) including Peripheral Health Institutes (PHIs).
Ni-kshay Aushadhi also helps in real-time management of stock position, providing expiry details of commodities, routine/ Additional Drug Request (ADR) Requirements, and patient-wise consumption of drugs at all levels.
Table 1: Nikshay Aushadhi Stakeholders
User Services Central TB Division (CTD)
1. Quantification
2. Purchase Order (PO) generation
3. Quality control
4. State warehouse Drug Transfer Advice (DTA)
5. Monitoring of nation-wide stock & expiry
CMSS warehouse
1. Quantification
2. Purchase request generation
3. Advance shipment details
4. Supplier delivery details
5. Release Order (RO) to SDS
6. Acknowledge desk
7. Transfer of drugs to other warehouses
GMSD
1. Quantification
2. Acknowledge desk
3. Advance shipment details
4. Transfer of drugs to other warehouses
Supplier
1. View Purchase Order (PO) and delivery schedule
2. Enter dispatch details
3. View receipt
4. Demand vs issue
SDS/ DDS/ Drug-resistant TB Centre (DR-TBC)/ TU
1. Routine/ ADR & dispatch to sub-stores
2. Acknowledge desk
3. Transfer of drugs to other warehouses
4. Issue voucher DTA
5. Box preparation, box modification, unpacking and box completion
6. Local purchase
PHI
1. Routine/ ADR
2. Acknowledge the receipt of drugs
3. Issue to patient
4. Return from patient
The Ni-kshay Aushadhi can be used for the following purposes:
- Quantification and forecasting
- Monitoring and distribution
- Data management and analysis
- Recording and reporting of the drugs related data
- Training and capacity building
- Quantification of drugs
- Issue/ dispatch
- Return of drugs
- Drug request management - Routine/ ADR
- Stock management (like drug inventory, Physical Stock Verification (PSV))
- Packaging/ repackaging
- Receive from store/ Acknowledge desk
- Quality control management
Image
Figure: Supply chain management in NTEP through Ni-kshay Aushadhi; Source: Ni-kshay Aushadhi Manual
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page ID Part of Pre-Test Part of Post-Test Ni-kshay Aushadhi can be used for the quantification and forecasting of drug stocks. True False 1 The Ni-kshay Aushadhi can be used for the following purposes:
- Quantification and forecasting
- Monitoring and distribution
- Data management and analysis
- Recording and reporting of the drugs-related data
- Training and capacity building
- Quantification of drugs
- Issue/ dispatch
- Return of drugs
- Drug request management - Routine/ ADR
- Stock management (like drug inventory, PSV)
- Packaging/ Repackaging
- Receive from store/ Acknowledge desk
- Quality control management
- Miscellaneous
Yes Yes Indenting
Receipt of Drugs/consumables
ContentThe process of receipt of drugs is completed through the Ni-kshay Aushadhi application. Once a consignment is dispatched to the receiving unit, the system will display following three options:
- Acknowledge Desk - For acknowledgment of drugs received against CTD-RO/ Issue Voucher
- DTA Receipt - For acknowledgment of drugs received against CTD-DTA: This process is to be used to record receipt of drugs which are received against DTAs issued by CTD/ issued by parent store to correct stock imbalances in sub-stores.
- Received from Third Party :This process is to be used when a store receives any drug or commodity from third party as donation.
- Receipt of 'complete' or 'partial' quantity of drugs can be acknowledged in Ni-kshay Aushadhi, as the case may be. When the user selects a particular consignment and clicks on the ‘Acknowledge’ option, the system shows a list of issued drugs/ items with the following details: Drug Name, Batch Number, Expiry Date, Requested Quantity, Issued Quantity, To be Acknowledged Quantity, Received Quantity, Damaged Quantity, Shortage Quantity.
- In instances where the quantity received is lesser than the issued quantity, the user should enter the same in the ‘Received qty’ column. As the request is partially acknowledged, the system will display it in the orange/ pink colour on the ‘acknowledge desk’. As and when the remaining quantity is received, the user can acknowledge the same by selecting the previous partially acknowledged record and entering the remaining quantity that has been received.
Resources
-
Standard Operating Procedure Manual-Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
-
Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
-
Receive and Acknowledge, Ni-kshay Aushadhi User Manual, CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The partially acknowledged ‘receipt’ will be shown in which colour in the ‘acknowledge desk’ on Ni-kshay Aushadhi? Yellow/ Blue Orange/ Pink Black/ White Green/ Red 2 The partially acknowledged ‘receipt’ will be shown in orange/ pink colour in the ‘acknowledge desk’ on Ni-kshay Aushadhi. Yes Yes Distribution to PHI
-
STLS: Maintaining Supplies of Lab consumables at TDC
FullscreenLaboratory consumables
ContentThe National TB Elimination Programme (NTEP) laboratory network is composed of National Reference Laboratories (NRLs) at the national level, at the state level Intermediate Reference Laboratories (IRLs) and Culture & Drug Susceptibility Testing (C&DST) laboratories and at the peripheral level Designated Microscopy Centres (DMCs).
Each of these laboratories is responsible for performing various functions at its own levels.

Figure: Flowchart of Laboratory Consumables
Table: Laboratory Consumables
Laboratory Consumables
Description
- Cartridge-based Nucleic Acid Amplification Tests (CBNAAT) machines and Cartridges
- The CBNAAT machines and cartridges are procured by Central TB Division (CTD) and supplied to state/ district/ CBNAAT sites based on their requirement.
- Cartridges are supplied based on the stock availability, consumption and expected case load.
- Recording, reporting and monitoring of cartridges are done through Ni-kshay Aushadhi.
- Binocular Microscope (BM) and LED Fluorescence microscopy (LED-FM)
- The procurement of both items is undertaken by CTD and then delivered to the states/ districts.
- All LED-FM/ BMs should be covered by annual maintenance contracts by states/districts, at the end of their warranty periods.
- NTEP guideline recommends 1 BM for every Designated Microscopy Centre (DMC) and LED FMs only for the high case load facilities with >25 slides per day.
- Along with public sector DMCs, NTEP may also supply BMs to DMCs established in other sectors like ESIS, Public Sector Undertakings, Medical College, etc., if required.
- Sputum containers
Calculation of requirement of sputum containers:
For diagnosis:
- During the first week of each quarter, the number of new pulmonary smear-positive cases registered and treated during the last quarter in the district should be determined and this number should be multiplied by 10.
- 10 is the average number of symptomatic required to be examined for detecting one case of new pulmonary smear-positive tuberculosis and it includes all types of patients.
- Since two sputum specimens are taken for each symptomatic patient, further multiply the number obtained above by 2.
- The final number derived would be the required no. of slides for diagnosis.
For follow-up:
- Two follow-up specimens are taken for the majority of patients (one at the end of the intensive phase and the other at the end of treatment), therefore one sputum container is needed for each follow-up.
- On the last working day of the quarter, count the number of sputum containers in stock and subtract from the required number as calculated above.
- Allow sufficient reserve stock for three months, add 10% to account for wastage of sputum containers, and account for the sputum containers in stock.
- Slides
- One slide is used to examine one specimen in a sputum container. Therefore, order a slightly higher number of slides, than the required no. of sputum containers to account for unavoidable breakage of slides.
- Order for both sputum containers and slides should be placed during the first week of the quarter.
- The supplies will be procured by the state/ district and supplied to all the peripheral health institutions in the district.
Resources
- Training Module (1-4) for Programme Managers and Medical Officers, NTEP, MoHFW, 2020.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD.
- Module for Laboratory Technicians, CTD, MoHFW, India, 2005.
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Identify the correct statement from the options given below.
The CBNAAT machines and cartridges are procured at the district level as per the requirement.
The CBNAAT machines and cartridges are procured centrally and supplied to state/ district/ CBNAAT sites based on their requirement.
The CBNAAT machines and cartridges are procured at the Designated Microscopy Centre level as per the requirement.
The CBNAAT machines and cartridges are procured at the Tuberculosis Unit level as per the requirement.
2
The CBNAAT machines and cartridges are procured centrally and supplied to state/ district/ CBNAAT sites based on their requirement.
Yes
Yes
Consumables required at a DMC
Content- Designated Microscopy Centres (DMCs) are the most peripheral laboratory under the National TB Elimination Programme (NTEP) network.
- Any person identified to be a presumptive TB patient is first referred to the nearest DMC for sputum examination or their sputum specimens are collected and transported to the DMC. Therefore, it is very important for the DMCs to maintain an adequate stock of reagents and other consumables.
- The Medical Officer (MO) of DMC is responsible for determining the number of reagents and other materials the DMC needs every month.
- The Senior Tuberculosis Laboratory Supervisor (STLS) ensures these supplies are distributed in a timely manner, as and when required.
- The Lab Technician (LT) is responsible for exhausting the old supplies before the new ones.
The consumables required at the DMC can be broadly categorised as:
- Consumables required for sputum collection
- Consumables required for slide preparation
- Consumables required for smear examination
- Consumables stationery
- Other
Table: List of Items with Technical Specifications of Laboratory Consumables Required for DMCs Sl. No. Name of the item Technical Specifications - For Sputum collection
Sputum containers Cups made of Special Medical Grade Polypropylene, thin plastic, translucent, diameter - 4 cm, capacity - 30 ml, the screwable cap should also be made of Special Medical Grade Polypropylene and should be airtight and leak-proof. Absorbent cotton 500 gms/roll Phenolic compound 5% phenol/ 40% phenolic compound (proprietary Phenyl) diluted to 5% Adhesive labels for sputum containers Sputum specimen transport box Insulated box, made of plastic 10” x 10” x 10”, thickness 1” with lid, handle and nylon belt 1” width 2.5 feet length, nylon strap of 1” width 2 feet length with velcro to strap the lid of the box from side to side. - For slide preparation
Slides for Microscopes Glass slides plain, size = 76mm x 26mm x 1.3mm, clean, scratch-free with smooth edges, uniform refractive index, pack of 50. Broomstick 10 cms in length and thick enough to make good smears. Diamond marker pencil 6" (15.24 cm.) holder with artificial diamond (hard stone) embedded at one end with a screw cap, to mark on microscope glass slides. Grease marking pencil Marking pencil MPS, blue or red coloured, 8" length, to write on glassware/ metal surfaces. Staining racks For drying the slides. Slide boxes for storing slides Glass (or metal) rods For holding slides during the staining process. Forceps, Chitel forceps Stainless steel for slides, 15 cm. Scissors 25 cm, stainless steel Ziehl Neelsen stain Auramine O fluorescent dye for Fluorescence Microscopy (FM) Wherever FM is being done Whatman filter paper No 1 3 ) For smear examination Binocular Microscope With 10x, 40x and oil immersion objective (100x) eyepieces (10x) and spare bulbs and fuses. Immersion oil Filter paper To drain the oil from the slides. Fine Silk and Lint cloth Lens paper For wiping the oil immersion lens after examination of each slide 4) Consumables - Stationery Request form for examination of biological specimen for sputum examination TB Laboratory Register Referral/ Transfer form for treatment Stock register – laboratory Marker pen 5 ) Other Plastic tumblers/ mugs Time (stop-watch) Spirit lamp or Bunsen burner Silica gel Hygroscopic agent to maintain the microscope in a moisture-free environment (to be placed in the cabinet for Binocular Microscope). Alcohol (absolute) Ethanol Cotton, full sleeves Aprons Disposable gloves 6 and 8 inches Methylated spirit Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- Guidelines for Quality Assurance of Smear Microscopy for Diagnosing Tuberculosis, RNTCP Lab Network, CTD, MoHFW, India, 2005.
- Module for Laboratory Technicians, CTD, MoHFW, India, 2005.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Sputum containers and their screwable cap used for sputum collection at the DMC should be made of Special Medical Grade Polypropylene and should be air-tight. True False 1 Sputum containers and their screwable cap used for sputum collection at the DMC should be made of Special Medical Grade Polypropylene and should be air-tight and leakproof. Yes Yes Who ensures that supplies are distributed in a timely manner at DMCs? Treatment Supporter Medical Officer Senior Tuberculosis Laboratory Supervisor (STLS) Lab Technician (LT) 3 The Senior Tuberculosis Laboratory Supervisor (STLS) ensures these supplies are distributed in a timely manner, as and when required.
Yes Yes Consumables required at CBNAAT Lab
ContentThe consumables required at a Cartridge-based Nucleic Acid Amplification Testing (CBNAAT) laboratory include the following:
CBNAAT/ GeneXpert Dx System consisting of CBNAAT machine preloaded with assay software, Computer and the Barcode reader
- CBNAAT assay kit (Figure) consisting of:
- CBNAAT cartridges: Kit contains 10 or 50 individually packed cartridges.
- CBNAAT reagent: 8 ml volume pack per cartridge. The sample reagent solution is clear but may range from colourless to golden yellow.
- Sterile pipette: Individually packed, disposable transfer pipettes, one per each test, with a single mark for the minimum volume of sample transfer to each cartridge.
- CD containing the Assay Definition File.
Figure: Contents of CBNAAT Assay Kit; Source: GLI Training Package for CBNAAT.
- Sputum containers
- Personal protective equipment:
- Laboratory coats
- Disposable gloves
- Disinfectants
- 1% Sodium hypochlorite solution
- 5% Phenol
- 70% Ethanol
-
Power stabiliser (UPS) for uninterrupted power supply to perform CBNAAT assay.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What are the components of the CBNAAT assay kit? CBNAAT cartridges CBNAAT reagent Sterile pipette All the 3 4 CBNAAT assay kit includes CBNAAT cartridges, CBNAAT reagent and sterile pipette. Yes Yes - CBNAAT assay kit (Figure) consisting of:
Consumables Required at a Truenat Lab
ContentConsumables required for Truenat test provided by the manufacturer include:
Trueprep AUTO MTB Sample Pre-treatment Pack for sample processing
- Liquefaction buffer
- Lysis buffer
- Disposable transfer pipette (graduated) - 1ml
Trueprep AUTO v2 Universal Cartridge Based Sample Prep Kit for DNA extraction
- The Reagent Pack contains the following reagents
- Wash Buffer A
- Wash Buffer B
- Elution Buffer
- Priming Waste
- The Cartridge Pack contains the following
- Cartridge
- Elute collection tube
- Elute collection tube label
- Disposable transfer pipette
- Disposable Transfer Pipettes (graduated) - 3 ml
- Reagent Reset Card
Truenat MTB Chip-based Real-Time PCR test for Mycobacterium tuberculosis
- Truenat MTB micro-PCR chip
- Microtube with freeze-dried PCR reagents
- DNase & RNase free pipette tip
Truenat MTB-RIF Dx Chip-based Real-Time PCR Test for Rifampicin Resistant Mycobacterium tuberculosis
- Truenat MTB-RIF Dx micro-PCR chip
- Microtube with freeze-dried PCR reagents
- DNase & RNase free pipette tip
Other Consumables
- Gloves
- Masks
- Sodium hypochlorite
Resources
- MolBio Diagnostics Product Details
- Practical Guide to Implementation of Truenat™ Tests for the Detection of TB and Rifampicin Resistance
Kindly provide your valuable feedback on the page to the link provided HERE
Stock Register at a DMC
Content- Designated Microscopy Centres (DMCs) are the most peripheral laboratory under the National TB Elimination Programme (NTEP) network. Therefore, it is very important for the DMCs to maintain an adequate stock of all consumables.
- A paper-based stock register is maintained at the DMC and submitted as a part of the ‘Monthly report on programme management, logistics and microscopy’.
- All the DMCs as well as Peripheral Health Institute (PHI) that are a DMC need to fill the second part of this monthly report format for reporting the status of laboratory consumables and equipment (Figure below).

Figure: Monthly report format for reporting status of laboratory consumables and equipment, to be filled by PHI that is DMC.
- The stock register for consumables at the DMC has the provision to enter the information about the stock of consumables that are available at the DMC on the first day of the month, stock received and consumed during the month and stock remaining on the last day of the month along with the requested quantity of new stock.
- The Lab Technician (LT) of the DMC is responsible for exhausting the old supplies before the new ones.
- The Medical Officer (MO) of the DMC is responsible for determining the stocks and the Senior Tuberculosis Lab Supervisor (STLS) should ensure these supplies are distributed in a timely manner, as and when required.
Table: Calculation of Stocks Required at the DMC
Sputum containers For diagnosis:
- During the first week of each quarter, the number of new smear-positive cases registered and treated during the last quarter should be determined and this number should be multiplied by 10.
- Ten is the average number of symptomatic required to be examined for detecting one case of new pulmonary smear-positive tuberculosis.
- Since two sputum specimens are taken for each symptomatic patient, further multiply the number obtained above by 2.
For follow-up:
- Two follow-up specimens are taken for the majority of patients - one at the end of the intensive phase and the other at the end of treatment. One sputum container is needed for each follow-up.
- Once the number of sputum containers required has been calculated, allow sufficient reserve stock for three months, add 10% to account for wastage of sputum containers, and account for the sputum containers in stock.
- On the last working day of the quarter, count the number of sputum containers in stock and subtract from that needed for diagnosis and follow-up examinations as calculated above.
Slides - Once the number of sputum containers needed for the next quarter is determined, order a slightly higher number of slides than the required no. of sputum containers to account for unavoidable breakage of slides.
Reagents - Reagents are supplied to the DMCs on monthly basis by the District TB Centre (DTC).
- The stock register should have the mention of expiry dates of the reagents and the first expiring reagents must be exhausted first based on the First Expiry First Out (FEFO) principle.
- The reagents should not be used beyond three months from the date of preparation.
CBNAAT/ Truenat Machines and Cartridges/ Chips
- These are procured centrally and supplied to state/ district/ sites based on their requirement.
- Recording, reporting and monitoring of cartridges/ chips is done through Nikshay-Aushadhi and they are supplied based on the stock availability, consumption and expected case load.
Binocular Microscopes (BM) and LED Fluorescence Microscopes (FM) - 1 BM is required for every DMC.
- The no. of BM in place and no. of BM in working condition should be reported in the stock register.
- LED FM is supplied to the high case load facilities where the workload is more than 25 slides per day.
Tuberculosis Laboratory Register - Each TB lab register allows for the registration of at least 2000 patients.
- For each lakh population, 75 smear-positive patients are projected, requiring the examination of 750 patients (thrice each). Additional follow-up examinations will bring the number of registers needed to approximately one lab register/ lakh.
- If there are blank pages in the register at the end of a year, it can be used the following year. However, every year should be started on a new page.
Laboratory Form for Sputum Examination - For diagnosis, approximately 10 laboratory forms for sputum examination are needed. (10 is the average number of symptomatic for each case of pulmonary smear-positive tuberculosis identified).
- For follow-up, approximately 0.2 laboratory forms for sputum examination are needed for each pulmonary tuberculosis case. (1 out of 10 examined will be smear-positive, each needs two forms for follow-up. When calculated, out of 10 it will be 0.2)
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, CTD, MoHFW, GoI, 2020.
- Module for STS Part 2: Ensuring Proper Registration and Reporting. CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many TB Laboratory Register/s is/are required in one year for each DMC? 1 2 3 4 1 Each Tuberculosis Laboratory Register allows for the registration of at least 2000 patients. For each lakh, 75 smear-positive patients are projected, requiring the examination of 750 patients (thrice each). Additional follow-up examinations will bring the number of registers needed to approximately one lab register/ DMC. Yes Yes For follow-up, approximately 0.2 laboratory forms for sputum examination are needed for each pulmonary tuberculosis case.
True False 1 For diagnosis, approximately 10 laboratory forms for sputum examination are needed. 10 is the average number of symptomatic for each case of pulmonary smear-positive tuberculosis identified. 1 out of 10 examined will be smear-positive, each needs two forms for follow-up. When calculated, out of 10 it will be 0.2
Yes
Yes
Assessment of stocks at DMC
ContentStock is critical in assuring that the network of Designated Microscopy Centres (DMC) has all of the necessary supplies, equipment, and commodities to conduct testing. It assures that TB control and patient management are not interrupted by stockouts.
Assessment of stocks at DMC is carried out by estimating the number of presumptive TB cases diagnosed and treated during the last quarter.
There is a standard checklist for the assessment of stock at DMC with the help of this checklist assessment is carried out.
Sl. No
Items
Item Adequate/ Acceptable
Problems Identified
Adequate stock and supply of:
1. Slides Y / N 2.
Lens tissue
Y / N
3.
Filter paper
Y / N
4.
Spirit lamp or bunsen burner
Y / N
5.
Immersion oil
Y / N
6.
Disinfectants
Y / N
7.
Smearing/ staining equipment (staining racks, loops, sticks, etc.)
Y / N
8.
Slide boxes
Y / N
9.
External Quality Assurance (EQA) forms
Y / N
Staining reagents/ equipment:
Within expiry date
1.
1% Carbol fuchsin
Y / N
2.
0.1% Methylene Blue
Y / N
3.
25% Sulphuric acid
Y / N
4.
Distilled water
Y / N
5
Equipment for preparation of stains/ reagents such as balance (for weighing reagents) and measuring cylinder, etc.
Y / N
Assessment is carried out by National Reference Laboratory (NRL)/ Intermediate Reference Laboratory (IRL)/ Central Internal Evaluation (CIE) team yearly once during their Onsite Evaluation (OSE) External Quality Assurance (EQA) visit by the Senior TB Laboratory Supervisor (STLS).
The DMC laboratory technician and the concerned Medical Officer (MO) in charge of the institution have to take adequate measures to address the problems identified.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Who does the assessment of stock at DMC?
National Reference Laboratory during their annual EQA OSE visit
Intermediate Reference Laboratory during their annual EQA OSE visit
Central Internal Evaluation team
STLS during their monthly OSE visit
All of the above
Assessment of stock at DMC done by NRL, IRL, CIE Team and also by STLS.
-
-
STLS: Supervision, Monitoring & Evaluation
Fullscreen-
STLS: Supportive supervision
FullscreenConcept and objectives of supervision
ContentConcept of Supervision
- Supervision is a systematic, ongoing process for increasing the efficiency of health personnel by developing their knowledge, perfecting their skills, improving their attitudes towards their work and increasing their motivation.
- It is one of the most important management functions in an organisation.
- Supervision is also defined as an act of a superior person overseeing the work of the personnel working under him or her. This overseeing means directing, investigating, guiding, helping and advising the subordinates in their performance with the purpose of achieving the established objectives.
- Therefore, it is an extension of training which provides constant observation, monitoring, evaluation and guidance to workers, with the aim of enabling them to perform their activities effectively and efficiently while maintaining the required standards.
Basic Tenets of a Good Supportive Supervisory Process
- Supervision is carried out in direct contact with health personnel.
- It is a two-way communication between supervisors and those being supervised.
- Supervisors are always accountable for the performance of the subordinates under her/his span of control.
- It should not be a fault-finding exercise but a collaborative effort to identify problems and find solutions. Supervisors are to help the workers improve, develop and reinforce knowledge and skills according to their individual learning needs.
- Supportive supervision is provided to health personnel at all levels since they need ongoing support for solving problems and to overcome difficulties.
- Health personnel also need constructive feedback on their performance and continuous encouragement in their work.
- Supportive supervision assists workers to perform in the best possible way to yield the best results in terms of realisation of the organisational goals.
Supportive supervision ensures smooth implementation and continuous programme improvement.
Objectives of Supervision
- To ensure equitable provision of high-quality healthcare services to all sections of society.
- To build capacity of the health staff to implement programme procedures correctly.
- To increase the involvement and commitment of staff at different levels, and to help staff develop their highest potential.
- To plan services cooperatively and to develop coordination to avoid overlapping.
- To develop standards of service and methods of evaluation of personnel and services.
- To assist in problem-solving of the matters concerning personnel, administrative and operational services.
- To provide timely and actionable feedback.
- To assess human resources and their training needs.
- To ensure logistic management as per guidelines.
- To ensure accurate and valid data recording and reporting in Nikshay and other recording systems.
- To interpret policies, objectives and needs of the organisation and to suggest ways and means to improve them.
Resources
- NTEP Training Modules (5-9) for Programme Managers & Medical Officers, 2020.
- Supervision and Monitoring Strategy, RNTCP, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following are the basic principles of supervision?
It is an ongoing process.
It involves a co-ownership between supervisors and those supervised.
It is a fault-finding exercise designed to point out the weaknesses in healthcare personnel.
Options 1 and 2
4
Supervision is an ongoing, two-way communication between supervisors and those being supervised. It should not be a fault-finding exercise but a collaborative effort to identify problems and find solutions.
Yes yes Supervisory checklist at TU level
ContentAt the Tuberculosis Unit (TU), the presiding supervisory team uses a standardized checklist mandated by the National TB Elimination Programme (NTEP) during their periodic supervisory visits. The report and copies of the checklist may be shared with appropriate authorities within 1 week of completing the supervisory visit.
These appropriate authorities include the Central TB Division, Ministry of Health and Family Welfare (MoHFW) and respective district and state authorities, who will in turn initiate remedial measures in a timely and appropriate manner.
The TB Unit/ Designated Microscopy Centre (DMC)/ Peripheral Health Institute (PHI) Health Facility Checklist is shown in the table below.
Table: Checklist for Supportive Supervisory and Monitoring Visits under NTEP for TB Unit/ DMC/ PHI - Health Facilities Name of the TB Unit/ DMC/ PHI:
Name of District and State:
Date of Visit:
Facilities Visited:
1 Interact with the Medical Officer (MO) to know their involvement in TB case detection. Look at the Outpatient Department (OPD) register to know what % of adult OPD patients are being referred for sputum microscopy. % 2 % of MOs trained in NTEP on the management of TB cases. (Assess their knowledge on NTEP, Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ Truenat services, newer Drug-resistant TB (DR-TB) drug regimen, Nikshay Poshan Yojana, etc.) % 3 Is the MO regularly undertaking supervisory visits? (Observe the field visits undertaken by the MOs in the supervisory register) Y/N 4 Information, Education and Communication (IEC)/ Advocacy, Communication and Social Mobilisation (ACSM) activities undertaken by the MO? (Enquire about the ACSM activities like school health programs, village health sanitation and nutrition meetings, community orientation meetings etc. undertaken, and observe for visible IEC wallpapers/ banners etc. in the PHI and its vicinity) Adequate/ Not adequate Designated Microscopy Centres 5 Are the sputum samples being tested as soon as they are received? (Observe for the presence of Laboratory Technician (LT) availability on all days, availability of Binocular/ Fluorescence Microscope(BM/ FM), the average time taken from the time of sample receipt to smear result reported (lab turnaround time) Y/N 6 Is the LT trained in performing smear microscopy? (Assess their knowledge of the smear microscopy procedure) Y/N 7 Lab turnaround time - Average time taken from the time of sample receipt to smear result reported (in days) 8 Are chest symptomatics offered chest X-ray? (either directly or linked with an X-ray centre - % of chest symptomatic offered) Y/N 9 Is there provision for collection and transport of samples of key populations/ TB notified patients to the CBNAAT/ Truenat lab available? (Review the transport mechanism available) Y/N 10 Are presumptive TB patients offered HIV testing? (% offered HIV testing – Check in the Lab register) Y/N 11 Are there adequate supplies of reagents, slides and other consumables for the next month? (Check for the reagents availability, quantity and labelling of expiry date) Y/N 12 Does the DMC have continuous water and electricity supply? Y/N Treatment Services 13 Are all diagnosed patients notified in the TB notification register? (Cross check the lab register with the TB notification register and look for the Nikshay id) Y/N 14 Are all notified patients initiated on treatment? (Including those referred/ transferred out) Y/N 15 Average time taken for treatment initiation from the time of diagnosis? (Calculate for 30 recent patients including those transferred/ referred out) (in days) 16 Are TB-notified patients offered HIV testing? (% offered HIV testing – Check in the TB notification register/ Nikshay) Y/N 17 Are TB-notified patients offered Diabetes Mellitus (DM) testing? (% offered DM testing – Check in the TB notification register/ Nikshay) Y/N 18 Are TB notified patients screened for Tobacco usage? (% screened for tobacco usage – Check in the TB notification register/ Nikshay) Y/N 19 Nikshay Poshan Yojana - % of TB notified patients who have been offered Nikshay Poshan Yojana (Patients currently in the PHI for the last 1 year may be taken) % Treatment Supporters 20 Does the treatment supporter require training/ sensitisation? (Assess knowledge in Directly Observed Therapy Short-course (DOTS), treatment card maintenance, patient services, Nikshay Poshan Yojana) Y/N 21 Is the treatment supporter monitoring daily drug intake by the patient (either directly/ digital adherence)? (Check the treatment card – cross-match with drugs issued and pills taken) Y/N 22 % of honorarium received? (Ask whether the treatment supporter has received the honorarium for all eligible patients who have completed their treatment) % Field Supervisors (Senior Treatment Supervisor (STS)/ TB Health Visitor (TBHV)/ General Health System (GHS) Staff) 23 Is an individual vehicle available for field visits? Y/N 24 % of TB notified patients currently on treatment in whom home visits have been undertaken? (Cross check with the treatment card/ Lat. long. coordinates captured in Nikshay/ patient interaction) % 25 % of TB notified patients currently on treatment linked to a treatment supporter? % 26 % of children identified in whom chemoprophylaxis with Isoniazid has been given? % 27 Has the staff received the salary & POL to date? If No, record the issues therein? Y/N 28 % of private notified patients in whom public health actions have been provided? % Senior TB Lab Supervisors (STLS)/ GHS staff 29 Is the STLS reviewing slides preserved by the LT during the On-site Evaluation (OSE)? Y/N 30 Are the reports of TU-OSE done by the STLS available in the DMC? (Check for the copy of at least the last month) Y/N 31 Is corrective action as suggested in the TU-OSE report being carried out by the DMC? (Current status may be used as an assessment of the corrective actions taken) Y/N 32 Assess 2 slides to check if they match with the OSE report? Matches/ Does Not match Drug Store 33 Is the stock register maintained as per guidelines? Y/N 34 Are the drug stocks adequate as per the suggested norms? Adequate/ inadequate 35 Are the stocks matching with Nikshay Aushadhi? Y/N 36 Is bio-medical waste from the DMC disposed of as per Bio-Medical Waste (management and handling) Rules 2016 Comments and Recommendations: (Use an extra sheet, if required) 1 2 3 4 Name and signature of the visiting team members with their designation: Resources
- NTEP Training Modules (5-9) for Programme Managers & Medical Officers, 2020.
- Supervision and Monitoring Strategy, RNTCP, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The TB Unit/ Designated Microscopy Centre (DMC)/ Peripheral Health Institute (PHI) Health Facility Checklist covers which of the following thematic areas?
Advocacy, Communication and Social Mobilisation
Direct Benefit Transfer
Stock availability
All of the above
4
The TU level checklist covers ACSM, DBT and stock availability as well as other parameters at the TU level.
Yes Yes Supervision by MO-TC at TU level
ContentThe Medical Officer-TB Control (MO-TC) at the TB Unit (TU) has the overall responsibility for the management of the National TB Elimination Programme (NTEP) at the sub-district level and is assisted by the Senior Treatment Supervisor (STS) and the Senior TB Lab Supervisor (STLS).
The MO-TC is responsible for supervising the work of the TU and of the STS and STLS, in addition to his/her other responsibilities. These visits are conducted on a systematic basis and the protocol to be followed during these visits is shown in the figure below.

Figure: Supervisory Protocols for the MO-TC
Abbr: NGO: Non-government Organisation
Checklist for the MO-TC at the TU
- Ensure that all private-sector patients are captured in the Nikshay portal by notification and that public health actions are taken on all TB patients notified irrespective of private or public.
- Ensure that the treatment supporters are adequately trained and updated on the latest guidelines.
- Ensure that the treatment supporters and the private providers are allotted proper Nikshay credentials and that the troubleshooting mechanism works promptly.
- Organise sputum smear examination at all DMCs of the sub-district.
- Ensure proper treatment categorisation of diagnosed patients by supporting other MOs of the sub-district.
- Ensure that Directly Observed Treatment (DOT) is taking place as per guidelines at all treatment observation centres.
- Ensure a regular supply of drugs and other logistics and ensure their uninterrupted availability in all Peripheral Health Institutes (PHIs) in the sub-district.
- Ensure periodic updating of treatment by the corresponding treatment provider/ supporter.
- Ensure that all the reports pertaining to programme management from the TU are submitted to the district on time.
- Ensure that all beneficiaries are given Direct Benefit Transfer (DBT) as per the guidelines.
- Ensure that the External Quality Assurance (EQA) of the DMCs under the TU is properly conducted every month.
- Ensure that the STS and the STLS do proper field visits, carry out the supervision and monitoring as per the checklist and give feedback on a periodical basis.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Technical and Operational Guidelines for Tuberculosis Control, Chapter 9, RNTCP, 2019.
- Module for Senior Treatment Supervisors, RNTCP, 2005.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How often should an MO-TC visit a DMC in their area?
Every month
Twice a month
Every quarter
Every day
1
The Medical Officer-TB Control (MO-TC) should cover all Designated Microscopy Centres (DMCs) every month.
Yes
Yes
Supervision by DTO at TU level
ContentThe District TB Officer (DTO) at the District TB Centre (DTC) has the overall responsibility for the physical and financial management of the National TB Elimination Programme (NTEP) at the district level as per the guidelines.
The DTO is also responsible for the involvement of other sectors in NTEP to ensure better compliance and is assisted by a Medical Officer (MO), statistical assistant and other paramedical staff. For each district, there should be a full-time DTO, who is trained in NTEP.
The Senior Treatment Supervisor (STS) and Senior TB Lab Supervisor (STLS) at the Tuberculosis Unit (TU) level are under the administrative supervision of the DTO/ Medical Officer -TB Control (MO-TC).
The DTO conducts supervisory visits by himself/ herself, or in a team of MO-TC/ STLS/ STS. These visits are conducted on a systematic basis and the protocol to be followed during these visits is shown in the figure below.

Figure: Supervisory Protocols for the DTO
Abbr: NTEP: National TB Elimination Programme; NGO: Non-government Organisation
The following are the major points to be covered by the DTO under supervision:
- All the MO-TCs, the NTEP staff (STS, STLS, TB Health Volunteers (TBHVs), DR-TB-HIV coordinators, PPM coordinators, etc.) are conducting supervisory visits and giving proper feedback on a periodical basis.
- Early diagnosis and treatment initiation are being carried out in the district by all stakeholders.
- Private Practitioners are sensitised adequately and they are notifying all cases of TB in Nikshay.
- Treatment provided by the Public provider is as per the program guidelines and Private practitioners are as per the standards for TB care in India.
- Public health actions are undertaken in all TB cases notified in Nikshay.
- Direct Benefit Transfer (DBT) is being provided to all beneficiaries as prescribed under NTEP.
- Nikshay recordings are updated and factual.
- External quality assurance is being carried out as per the NTEP protocol.
- Drugs and supplies are supplied uninterruptedly and as per the stocking norms at various levels.
- Microscopes and the other diagnostic equipment including the Nucleic Acid Amplification Test (NAAT) devices are adequately calibrated, and the annual maintenance is being carried out as per protocol.
- All MOs and the staff carrying out TB services in the district are adequately trained.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Technical and Operational Guidelines for Tuberculosis Control, Chapter 9, RNTCP, 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How often should a DTO visit a TB unit in their area?
Every month
Twice a month
Every quarter
Every day
1
The District TB Officer (DTO) should cover all TB units every month.
Yes
Yes
Role of STLS at a DMC
ContentThe Senior TB Laboratory Supervisor (STLS) is the person responsible for monitoring the day-to-day activities of all the microscopy centres and nucleic acid amplification test (NAAT) sites and is thus essential to the success of the National TB Elimination Programme (NTEP). They also ensure the quality of TB diagnostic services.
Roles of STLS at the DMC
- Program management
The STLS is responsible for ensuring that microscopy services in the district are well organized and the locations of the designated microscopy centres (DMCs) are known to all the medical officers in all peripheral health institutions (MO-PHI).
The STLS also ensures that there are:
- Uninterrupted staffing of DMCs, including coverage for laboratory technicians (LTs) that might be on leave, so that there is regular and uninterrupted availability of smear examination at the DMC.
- Uninterrupted supply of reagents and logistics required for the microscopy.
- Quality assurance and accuracy guarantee for the microscopic activities carried out.
- Regular training and continuing education of LTs.
The STLS reports to the district TB officer (DTO) in collaboration with the senior treatment supervisor (STS) regarding implementation, quality control (QC), supervision and management of laboratory supplies.
- Monitor documentation related to microscopy
STLS ensures that all documentation related to sputum smear examinations is accurate and reports of examinations are given to the treating physician promptly. This includes:
- Each LT has a TB lab register which is filled completely and accurately.
- LTs understand the importance of limiting administrative errors (for example, keeping the sputum specimens with the proper lab forms for sputum examination and slides) and accurately recording the results of sputum smear examinations.
- LTs keep examined slides for review and on-site evaluation (OSE) visit by the STLS.
- There is an accurate recording of the results of the sputum smear examination.
STLS must explain to LTs that patients are diagnosed and placed on appropriate treatment regimens based on the smear results.
- Ensure appropriate number and schedule of sputum examinations
- Presumptive TB persons should have their sputum examined the correct number of times for tubercle bacilli, at least 2 sputum samples should be examined.
- Follow-up cases should have 2 sputum samples examined and should be done according to the follow-up schedule.
- Perform laboratory QC
This is done via OSE visits. The visit includes a comprehensive assessment of the laboratory safety including infection control measures; conditions of the equipment, adequacy of supplies as well as the technical components of acid-fast bacilli (AFB) smear microscopy employing a simple “Yes” and “No” checklist.
- The STLS visits every DMC under their supervision at least once every 4 weeks, and more often if possible.
- During these visits, at least 5 positive and 5 negative slides must be re-checked by the STLS.
- Staff at the DMC is supervised, evaluated and trained during these visits.
- The STLS maintains a diary, recording the details of these field visits.
At the end of each QC visit, detailed feedback is given by the STLS for continuous internal quality improvements. The STLS also ensures that centres maintain proper storage and transport of sputum specimens, the safety of lab staff and the maintenance of microscopes.
5. Waste disposal checks: STLS ensures that contaminated material is disposed of safely to ensure infection control. Sputum containers with sputum must either be incinerated, disinfected and autoclaved, or burnt in a pit and the burnt material buried.
6. Maintain an adequate supply of all materials necessary for microscopic examination
The STLS ensures that LTs have an adequate supply of reagents, sputum containers, slides and other materials including boxes for storing slides. This includes:
- Calculating the required volume of material (slides, sputum containers, etc.) required.
- Ordering supplies during the first week of the quarter to ensure uninterrupted supply at all DMCs.
- Distribution of sputum containers to all sputum collection centres/ DMCs in the area.
- Estimating and ensuring maintenance of adequate reserve stock at DMCs.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- Module for Senior Tuberculosis Laboratory Supervisors, NTEP, 1999.
- Module for Laboratory Technicians, NTEP, 2005.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the role of the STLS in the DMC?
Conduct an on-site evaluation visit.
Make sure that LTs fill the TB lab register properly.
Ensure adequate supply of lab material, like slides, at the DMC.
All of the above
4
The STLS conducts an on-site evaluation visit at the DMC, ensures proper documentation of smear results and ensures an adequate supply of lab materials at the DMC.
Yes
Yes
How often should the STLS visit the DMC?
Every 2 weeks
Every month
Every quarter
Every 6 months
2
The STLS visits every DMC under their supervision at least once every 4 weeks, and more often if possible.
Yes
Yes
-
STS: Internal Evaluation
FullscreenInternal Evaluation
ContentIntroduction
Internal Evaluation (IE) is a process of critically evaluating a programme by the programme people to understand determinants of both good and poor performance and enable uptake of the strategic measures for improvement. IE is an integral component of the National Tuberculosis Elimination Programme’s (NTEP) supervision and monitoring strategy.
Objectives of IE
1. To provide a systematic framework for assessing programme performance, financial & logistics management, recording and reporting, and quality of care received by patients.
2. To give recommendations for improving the quality of programme implementation and performance with a realistic action plan and timeline.
3. To monitor efforts to improve and maintain programme quality and performance over time.
Types of IE
Image
IE Methodology
-
Selection of Districts:
At least one good-performing district and one under-performing district should be selected. For states with population up to 30 million – 2 districts per quarter; 30-100 million – 3 districts per quarter; >100 million – 3-4 districts per quarter should be evaluated. In States/Union Territories (UTs) with 4 or less districts, 1 district or Tuberculosis Unit (TU) per quarter may be evaluated.
-
Selection of TB Units/ Designated Microscopy Centres (DMCs):
Five DMCs are selected as follows:
-
DMC at District TB Centre (DTC)
-
Two DMC that are examining a higher number of TB suspects (preferably from different TU)
-
Fourth and fifth DMC are selected randomly from the remaining DMCs (preferably from different TU)
-
Selection of Directly Observed Treatment (DOT) Centres:
The DOT Centres attached to each of the 5 selected DMCs (and Medical College conveniently selected) should be evaluated.
5 additional DOT Centres must be identified in the district with unique characteristics such as those attached to a medical college (other than the one conveniently selected for a visit), other sectors like ESI, Railways, NGOs, private sector, Anganwadi workers, Accredited Social Health Activist (ASHA), community volunteer) and evaluated.
d) Selection of Patients:
A total of 36 to 39 patients should be interviewed in the district.
-
In each of the 2 DMCs with a low caseload, 4 New Smear Positive (NSP) patients are selected randomly, and one previously treated case conveniently (5 X 2= 10 patients).
-
In each of the DMCs at DTC & 2 TU level DMC, 4 NSP patients are selected randomly, and 1 patient, each of the types Relapse, Treatment after Loss to Follow up (LFU) and Failure, are conveniently selected.
-
Also select 1 TB/HIV patient and 1 DOTS-Plus patient (for districts implementing DOTS-Plus) (7 X 3 =21 + 3 +3= 27).
-
At least 2 paediatric patients undergoing DOTS treatment within the district must be visited.
IE Activities
Image
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is an objective of IE?
To provide a systematic framework for assessment of programme performance.
To give recommendations for improving the quality of the programme.
To monitor efforts to improve and maintain programme quality and performance over time.
All of the above
4
The objectives of IE are:
1. To provide a systematic framework for assessment of programme performance, financial & logistics management, recording and reporting, and quality of care received by patients.
2. To give recommendations for improving the quality of programme implementation and performance with a realistic action plan and time line.
3. To monitor efforts to improve and maintain programme quality and performance over time.
Yes
Yes
-
-
-
STLS: Private sector Engagement
Fullscreen-
STLS: Private sector engagement in NTEP
FullscreenStakeholders for Private Sector Engagament
Importance of Private Sector Engagament
Vision of NTEP regarding Private Sector Engagement
STEPS
ContentThe System for TB Elimination in Private Sector (STEPS) model evolved as a solution to address gaps in the quality of care for patients in the private sector by ensuring standards of TB care in India (STCI). STEPS is envisioned as an equal partnership between the public and private sectors for the benefit of society with TB elimination as the outcome.
The primary objective of STEPS is to address gaps in the quality of care for patients in the private sector by ensuring standards of TB care in both sectors to all citizens in a patient-centric manner.
Components of STEPS
- Establish STEPS centre in each private hospital: These centres act as a single window for notification, linkage for social welfare measures, contact investigation, chemoprophylaxis, direct benefit transfers and treatment adherence support.
- Consortium of private hospitals: Provides policy and resource support, and reviews the centre's performance.
- Coalition of all professional medical associations: Sensitizes and supports specialists and doctors, and advocates with doctors for standards for TB care.
Establishing STEPS Centres
- In January 2019, the STEPS model was initiated and piloted in 14 districts in Kerala.
- Establishing STEPS centres at all private and cooperative hospitals is the heart of private sector engagement in Kerala.
- STEPS centres are single window mechanisms at private hospitals to help doctors and to ensure that all TB patients diagnosed that particular hospital receive high standards of TB care.
- The STEPS centre will coordinate notification and follow up patients till the end of treatment, ensure all public health actions and link them to social welfare measures.
- Patients will be followed up through an ‘after sales service model’ which is based upon a blend of self-initiated business promotion and customer loyalty blended with the social responsibility of private sector
Functions of STEPS Centres
- To act as a single window mechanism for all TB-related services in the hospital
- Notify in Nikshay all TB cases diagnosed in the hospital
- To guide, support and arrange for:
- Universal Drug Susceptibility Testing (UDST)
- National TB Elimination Programme (NTEP) drugs if required
- Direct Benefit Transfer (DBT) of Rs 500 per month during treatment
- Provisions for airborne infection control (AIC) kit
- Mobile based adherence monitoring system (99 DOTS) in case of NTEP drugs
- Offer HIV counselling and testing
- To educate on TB and counsel the patient and family members on the need for completing treatment
- To educate the patient and family members on AIC, adverse drug reactions (ADRs) and smoking cessation
- To follow up the patient periodically over the phone to motivate the patient to continue treatment, detect any ADRs, remind about follow up investigations and scheduled clinical visits
- Update details of bank account, UDST, treatment initiation, co-morbidity and outcome in Nikshay
- Fast tracking patients with infectious TB as a step to ensure AIC in health facility
- Ensuring other public health actions including contact tracing, chemoprophylaxis either directly or linking those patients willing to be followed up by the government field staff to local primary health care team
- Document all activities and submit monthly report to the Private Hospital Consortium

Figure: Schematic Representation of STEPS Center Within a Hospital; Source: STEPS: A Solution for Ensuring Standards of TB Care for Patients Reaching Private Hospitals in India; Shibu B et al. 2021
Forming a Private Hospital Consortium
In every district, a consortium of private hospital owners provides policy and resource support for STEPS centers and reviews the STEPS centres' performance. Consortium members select one of the hospitals to serve as chair for a fixed term. The district program manager of NTEP serves as member secretary. The consortium meets once in 3 months to review the performance of STEPS centers and suggest corrective actions if required.
Create a Coalition of Professional Medical Associations
- In all districts, a coalition of professional medical associations advocates with medical practitioners and sensitizes them on STCI and STEPS.
- In addition to the Indian Medical Association, members of the coalition include associations of chest physicians, pediatricians, general physicians, geriatrics, family medicine, nephrologists, general surgeons, orthopedic surgeons, and radiologists.
- The coalition meets every 3 months to plan and review the activities as per the plan.
Initial Results of STEPS
- Since its pilot, TB patient notification to NTEP from the private sector in Kerala has increased. Also, public health actions, such as Direct Benefit Transfer (DBT), Universal Drug Susceptibility Testing (UDST), HIV testing, etc., for patients diagnosed from the private sector has increased.
- STEPS led to a shift from using private anti-TB drugs to NTEP-supplied drugs, leading to 2,000 additional cases being put on NTEP-supplied drugs. Overall, 70% of all cases notified from the private sector in 2019 were treated with NTEP-supplied drugs.
- Data officially collected by the state drug controller showed that the sale of anti-TB drugs decreased from 1.6 million rifampicin units in 2018 to 0.5 million rifampicin units in 2019 after the establishment of the STEPS model.
- Qualitative feedback also showed that STEPS was an acceptable model to all stakeholders, and patients were satisfied with the services received. During COVID-19, STEPS was resilient enough to ensure TB patient services and facilitate partnerships for COVID-19 management.
Resources
- Guidance Document on STEPS (System for TB Elimination in Private Sector) in Kerala.
- STEPS – A Patient-centric and Low-cost Solution to ensure Standards of TB Care to Patients Reaching Private Sector in India, Rakesh, P.S., Balakrishnan, S., Sunilkumar, M. et al, BMC Health Services Research, 2022.
- STEPS: A Solution for Ensuring Standards of TB Care for Patients Reaching Private Hospitals in India, Shibu Balakrishnan, Rakesh PS, et al., Global Health: Science and Practice, June 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The System for TB Elimination in Private Sector (STEPS) model has led to a quantitative increase in patient health outcomes and is acceptable to TB patients coming from private centres in the pilot districts.
True
False
1
The System for TB Elimination in Private Sector (STEPS) model has led to a quantitative increase in patient health outcomes and was found as an acceptable model to all stakeholders, including patients.
Yes Yes Patient Provider Support Agency [PPSA]: A Multipronged Approach to Engage the Private Sector
ContentTo achieve universal Tuberculosis (TB) care for all notified TB patients, the National TB Elimination Program (NTEP) has initiated the Patient Provider Support Agency (PPSA) initiative.
PPSA is a model under which a third-party agency/non-governmental organization is selected by a state/ city/district NTEP unit to engage private-sector doctors treating patients of TB and provide end-to-end services, such as diagnosis, notification, patient adherence and support, and treatment linkages.
The third-party agency is selected as per the contracting procedures laid down by the respective State National Health Missions (NHM).
PPSA follows a multipronged approach to engage private providers engaged in TB care to patients that includes:
- Mapping private-sector providers (formal and informal), laboratories and chemists
- Increasing engagement of private-sector providers through in-clinic visits and continuing medical education (CME)
- Linking NTEP-provided diagnostic services (sputum microscopy, X-ray, cartridge-based nucleic acid amplification test, sputum collection and transport) and fixed drug combinations (FDCs)
- Facilitating and updating TB notification and other relevant information in Nikshay
- Facilitating incentives given by NTEP to the private-sector doctors and patients
- Counseling the patients to ensure treatment adherence
- Facilitating linkages for drug resistant-TB treatment and HIV services, as required.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Direct Engagement
ContentThe private-sector health facilities have experts and infrastructure to manage TB cases. Under the direct engagement partnership model, the programme manager directly engages private-sector health facilities which provide TB services to ensure that standards of TB care reach all the patients in that facility.
In a region where there is no dedicated Patient Provider Support Agency (PPSA), the National TB Elimination Programme (NTEP) can directly empanel and engage a private/ corporate/ trust hospital and designate them as “TB Treatment Centres”.
Services that can be provided under this model are:
- Identifying presumptive TB cases and testing them for TB with reimbursement of testing cost to the laboratory.
- Notifying and managing drug-sensitive TB with reimbursement of medicine cost to the disbursing chemist.
- Managing ambulatory treatment support of Drug-resistant TB (DR-TB) as per need.
- Bundling treatment services with public health actions by engaging facilities which can do both directly or who can engage another service provider to ensure complete coverage of public health actions for patients treated in their facility.
- Providing specialist consultation when the NTEP does not have enough specialist doctors to manage patients or requires additional specialist doctors.
Covering Private Sector TB Patients through Public Health System: The Mehsana Model of Universal Access to Free TB Care, Gujarat
- Mehsana is a town in Gujarat implementing India’s first pilot allowing for universal free anti-TB drugs in India.
- The programme is managed by the district TB office, supported by technical partners, and has engaged a large proportion of private providers.
Overview of the Mehsana Model
- The patient goes to a Private Provider (PP)/ chemist/ pharmacist.
- PPs/ chemists refer presumptive TB cases for chest X-rays or smear tests.
- The patient is provided with a unique number (i.e., a voucher) when prescribed a diagnostic test. The e-voucher links the patient with NTEP.
- A call centre operated by an NTEP staff member generates and tracks this e-voucher and reimburses the diagnostic facilities for the test.
- If the initial test is positive, the provider refers the patient to a formal provider for Drug Susceptibility Testing (DST). Costs of these tests are also reimbursed via the e-voucher.
- The PP also notifies the case, and incentives for notification are sent to the PP/ chemist.
- Monthly prescriptions come with an e-voucher, which patients can use to obtain medications (from a list of approved anti-TB drugs) from any local chemist who participates in the initiative
Over the entire course of the treatment process, the TB programme in Mehsana deploys field workers to monitor and facilitate drug compliance via home visits.
All the chemists and doctors in Mehsana were mapped and engaged. Doctors were trained to help them tailor prescription practices. NTEP offered no financial incentive to the doctor and only offers a minor overhead charge to the pharmacists.
In the end, the programme provides a win-win situation for all: the chemist acts as a referral point, the patient gets the right diagnosis and free drugs, and the private physician retains his or her patients.
Key Results
Of all the patients who initiated anti-TB treatment through the initiative, 72% successfully completed their regimens.
Lessons Learned from the Mehsana Model
Mehsana helped demonstrate proof of concept for a model that directly engages private healthcare providers to diagnose, notify, and treat TB cases and to strengthen adherence to the TB treatment regimen.
- Since PPs are often the first point of contact for patients, it is important to directly engage them by offering the right incentives to promote standard TB care.
- Information, Communication and Technology (ICT) tools were used at various stages (during the mapping exercise and the use of e-vouchers) of the initiative. Thus, the role of technology in existing partnership options must not be discounted.
Resources
- NTEP Training Modules (5-9) for Programme Managers & Medical Officers, NTEP, 2020.
- Mainstreaming Private Healthcare Systems for Tuberculosis Control, The Bridgespan Group, 2018.
- Ending Tuberculosis in India: A Political Challenge & an Opportunity, IJMR, 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is true about the Mehsana model?
It is a private sector partnership model that directly engages chemists.
It is a proven model that shows increased case notifications.
It did not require the use of any ICT tools.
Options 1 and 2
4
The Mehsana Model of Universal Access to Free TB Care, Gujarat is a private sector partnership model that directly engages private providers/ chemists to ensure standards of care for TB. It is a proven model that shows increased case notifications.
Yes Yes Mandatory Notification of TB Diagnosis
ContentTB is a notifiable disease in India, and TB notification has been made mandatory at the point of diagnosis since May 2012. This means that when a case of TB is diagnosed and/or put on treatment it is to be reported to the NTEP.
- Every healthcare provider, i.e., clinical establishments run or managed by the Government (including local authorities), private or NGO sectors and/or individual practitioners, need to notify diagnosed or treated TB patient’s.
- Reporting is to be done on the online reporting system called Nikshay and should include details of patient identification, and TB diagnosis.
- This, apart from enabling essential public health actions such as Treatment initiation, and Contact Tracing, chemoprophylaxis, but also enables provisions of Direct beneficiary transfer for Nikshay Poshan Yojana
Points to Note:
As per MCI code of ethics a registered medical practitioner giving incorrect information on his name and authority about notification amounts to misconduct and such a medical practitioner is liable for deregistration. It is the duty of the registered medical to divulge this information to the authorized notification official as regards communicable and notifiable diseases.
Resources
PHA for patient notified from the private sector
ContentAs a public health responsibility to prevent transmission of TB infection and development of drug resistance it is essential to engage both the public and private sectors for effective TB prevention and control. A total of seven standards related to Public Health Actions (PHA) (Standard 12 to Standard 18) have been mentioned in the Standards for TB Care in India (STCI)-2014. All patients notified from the private sector also need to be offered all public health actions.
This could be achieved in collaboration with the local public health services and/or other agencies.
1) Provide Access to Correct and Complete Diagnosis for Private Sector Patients
- In this regard all private providers must be sensitized, and their capacities must be built with respect to early diagnosis, prompt referral for sputum smear examination to the National TB Elimination Programme (NTEP) diagnostic facilities / NTEP accredited private labs.
- All private providers and chemists/pharmacists must mandatorily notify the TB patients to the local health authorities – District Health Officer / District TB Officer.
2) Provide Support for Treatment Adherence
- A treatment support plan must be developed at the time of treatment initiation for all patients in the private sector too, in mutual consultation with patient and private provider.
- All patients receiving treatment from the private sector must also be eligible to receive counselling services and upon consent, home visit counselling sessions (or at the location convenient to the patient) may be provided to patients and their caregivers under the NTEP’s Public Private Mix (PPM) or in association with partner agencies providing counselling services under NTEP.
- Any instance of treatment interruption must be reported at the earliest through Ni-Kshay.
- The patients may also be linked to Ni-Kshay call-centers for adherence support.
- The NTEP has also partnered with Patient Provider Support Agency (PPSA) / Patient Provider Interface Agency (PPIA) wherein vouchers were provided to private sector TB patients for utilizing subsidized TB diagnostic and follow up investigation services and can be scale up in high burden districts across the country with support from state governments/ Corporate Social Responsibilities (CSR) agencies.
4) Contact Tracing and TB Preventive Treatment
- All private providers must hold a responsibility to ensure that persons in close contact with patients who have infectious tuberculosis are evaluated at the earliest and managed in line with NTEP recommendations. The district health officers and district TB officers must be responsible to ensure this is being done on a regular basis.
- Eligible contacts should also be counselled for initiation of TB preventive treatment.
5) Linkage to Social Welfare and Protection
- Upon notification by the private provider and initiation of appropriate TB treatment, all patients seeking treatment under the private sector become eligible to receive direct benefit transfer (DBT) under the government of India's Nikshay Poshan Yojana (NPY)
- In districts where PPSA is available, PPSA staff may perform the linkage of private sector patients to DBT services and in districts where PPSAs are not available, the TB Health Visitor/ Senior Treatment Supervisor (STS) needs to undertake the public health action under the supervision of the PPM Coordinator.
- The patients may also be guided and linked to various other social protection and welfare schemes available under central and state governments. The partner agencies with expertise in referral linkages shall help the NTEP in achieving this.
6) Liaison with Professional Bodies
- Professional bodies such as Indian Medical Association and Indian Pharmaceutical Association must be involved for advocacy regarding the services available under public health actions of NTEP for the private patients.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, GoI, 2021.
- Mandatory TB Notification Gazette for Private Practitioners, Chemists and Public Health Staff, RNTCP, 2018.
- Notification of TB Cases: Amendments, MoHFW, GoI, 2015.
- TB Notification Order, MoHFW, GoI, 2012.
- National Strategic Plan for Tuberculosis Elimination 2017-2025, RNTCP, CTD, MoHFW, 2017.
- Standards for TB Care in India, WHO, 2014.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Linkage of private sector TB patients to available social support schemes is a part of public health action. True False 1 Linkage of private sector TB patients to available social support schemes is a part of public health action Yes Yes Schedule H-1 Regulation
ContentUnder the Drugs & Cosmetics Rules 1945, drugs specified under Schedule H are required to be sold by retail on the prescription of a Registered Medical Practitioner (RMP) only. At present, Schedule H contains 510 drugs.
Recently, a new Schedule H1 has been introduced through gazette notification GSR 588 (E) dated 30-08-2013, which contains certain third and fourth-generation antibiotics, certain habit-forming drugs and anti-TB drugs.
These drugs are required to be sold in the country under the following conditions:
(1) The supply of a drug specified in Schedule H1 shall be recorded in a separate register at the time of the supply giving the name and address of the prescriber, the name of the patient, the name of the drug and the quantity supplied and such records shall be maintained for three years and be open for inspection.
(2) The drug specified in Schedule H1 shall be labelled with the symbol "Rx" which shall be in red and conspicuously displayed on the left top corner of the label, and shall also be labelled with the following words in a box with a red border:
“Schedule H1 Drug Warning:
-It is dangerous to take this preparation except in accordance with the medical advice.
-Not to be sold by retail without the prescription of a Registered Medical Practitioner.”
List of anti-TB drugs included in Schedule H1
- Ethambutol hydrochloride
- Ethionamide
- Isoniazid
- Levofloxacin
- Moxifloxacin
- Pyrazinamide
- Rifabutin
- Rifampicin
Obligations of Chemists with Regard to Sales of Anti-TB Drugs Under Schedule H1
- Mandatorily keep a copy of the prescription of drugs covered under Schedule H1 in a separate record and such record should be maintained for three years and be available for inspection.
- The supply of a drug specified under schedule H1 shall be recorded in a separate register at the time of supply giving the name and address of the prescriber, the name of the patient, the name of the drug and the quantity supplied and such record shall be maintained for three years and be open for inspection (Annexure IV).
Table: Annexure IV – Schedule H1 Drugs Record Format; Source: Frequently Asked Questions on Gazette on Mandatory TB Notification for Chemists/ Pharmacies. tbcindia.gov.in.
Sl No:
Date
Name of doctor/ prescriber
Address & Reg. No:
Name of patient & address
Name of drug
Batch number
Expiry
Quantity sold
Bill no.
Resources
- Rules for Selling of Drugs Under Schedule H1, Press release by MoHFW, 2013.
- The Drugs & Cosmetics Act and Rules, Ministry of Health & Family Welfare, Government of India, 2016.
- Frequently Asked Question on Gazette on Mandatory TB Notification for Chemists/ Pharmacies, Central TB Division.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Schedule H1 drugs can be sold without the prescription of a registered medical practitioner.
True
False
2
Schedule H1 Drug Warning:
-It is dangerous to take this preparation except in accordance with the medical advice.
-Not to be sold by retail without the prescription of a Registered Medical Practitioner.”
Yes
Yes
Incentive For Notification and Outcome Declaration
-
-
STLS: ACSM
Fullscreen-
STLS: Advocacy, Communication & Social Mobilization in NTEP
FullscreenAdvocacy Communication and Social Mobilisation
ContentAdvocacy refers to activities that seek to influence the influencers and decision-makers, so as to make TB more central as a public health agenda and enlist their (influencers’) support to create an enabling environment in support of the National TB Elimination Programme (NTEP) to eliminate TB. Advocacy fosters political will, increases financial and other resources on a sustainable basis, and holds authorities accountable to ensure that pledges are fulfilled and results achieved.
Communication is a process people use to exchange information about TB through media, including such channels of communication as mass media, mid-media, and Interpersonal Communication (IPC). Much of the communication effort on TB is concerned with transmitting a series of messages to the people affected by TB through mass media and mid-media, which are necessary but not sufficient. As ‘participation’ and ‘dialogue’ are necessary for effective communication, IPC occupies a place of vital importance. Communication aims to improve knowledge about TB and TB services and change attitudes and practices to encourage people to seek care and complete TB treatment.
Social mobilisation is the process of bringing together different stakeholders and building partnerships to prevent, detect, and cure TB. It targets different sections of the targeted population, say a village community, ward, or other small groupings, and raises awareness of and demand for the TB elimination program. The emphasis here is on community participation and involvement in TB case detection and cure.
Resources
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Placing TB higher on the political agenda of governments is an achievement of:
Advocacy
Coordination
IPC
None of the above
1
Advocacy is a broad set of coordinated efforts to place TB higher on the political agenda, strengthen government commitment to implement or improve TB-related policies and increase and sustain financial and other resources for TB.
Yes
Yes
What is A in ACSM
ContentIn ACSM, "A" stands for Advocacy. "Advocacy" is an activity by an individual or a group that aims to influence the decisions within political, economic and social institutions.
Advocacy focuses on influencing policy-makers, funders and international decision-making bodies through a variety of channels:
- Conferences, summits and symposia
- Celebrity spokespeople, press conferences, news coverage
- Meetings between various levels of government and civil society organizations
- Official Memoranda of Understanding (MoU), parliamentary debates and other political events
- Partnership meetings, patients’ organizations, private physicians, radio and television talk shows, and service providers.
Types of advocacy
- Policy advocacy: Mainly targets policy-setting, influencing policymakers to incorporate the latest evidence and informs senior politicians and administrators how an issue will affect the country, and outlines actions to take for improving the laws and policies.
- Programme advocacy: Targets opinion leaders at the community level on the need for local action.
- Media advocacy: Validates the relevance of a subject, puts issues on the public agenda and encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilization for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
News reports on World TB day celebrations are an example of which of the following types of advocacy?
Policy advocacy
Programme advocacy
Media advocacy
None of the above
3
Media advocacy encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Yes Yes What is C in ACSM
ContentCommunication aims to favourably change knowledge, attitudes and practices among various groups of people.
Types of communication in healthcare are:
- Oral/verbal communication- by word of mouth (speech/talk)
- Written communication- exchange of facts, ideas and opinions through the use of written materials
- Non verbal communication- through gestures, body language or posture, facial expressions, and eye contact
- Visual communication- exchange of ideas through visuals
Health communication aims to influence and empower individuals, populations and communities to make healthier choices. It frequently informs the public of the services that exist for diagnosis and treatment and relays a series of messages about the disease. It aims to inculcate behaviour change for healthy life choices.
E.g.: “Seek treatment if you have a cough for more than two weeks”, “TB hurts your lungs” or “TB is curable”.
Approaches to health communication
1. Informative communication
Provides information about a new idea and makes it familiar to people.
2.Educative communication
A new idea on health behaviour is explained, including its strengths and weaknesses.
3.Persuasive communication
Usually in the form of a message that promotes a positive change in behaviour and attitudes, and which encourages that audience to accept the new idea. This approach to message development involves finding out what most appeals to a particular audience. Persuasive approaches are more effective than coercive approaches in achieving behaviour change.
4.Prompting communication
Messages are designed so that they are not easily ignored or forgotten they can be used to remind the audience about something that reinforces earlier messages.
Behaviour Change Communication (BCC)
- Behaviour Change Communication (BCC) is an interactive process of any intervention with individuals, groups or communities to develop communication strategies to promote positive health behaviours which are appropriate to the current social conditions and thereby help the society to solve their pressing health problems.
- BCC creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
- It aims to change behaviour – such as persuading people with symptoms to seek treatment – and to foster social change, supporting processes in the community or elsewhere to spark a debate that may shift social mores and/or eliminate barriers to new behaviour.

Figure: Behaviour Change Communication
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What does the environment created by behaviour change communication encourage the TB-affected communities to do?
Discuss, debate, organize, communicate
Discuss, organize, implement, communicate
Organize, enforce, communicate
None of the above
1
Behaviour change communication creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
What is SM in ACSM
ContentSocial Mobilisation (SM) is the process of bringing together different stakeholders and building partnerships to prevent, detect and cure TB. It generates dialogue, negotiation and consensus among a range of players that includes decision-makers, the media, Non-government Organisations (NGOs), opinion leaders, policy-makers, the private sector, professional associations, TB-patient networks and religious groups.
At the heart of social mobilisation is the need to involve people who are either living with active TB or have suffered from it at some time in the past.
Aims of Social Mobilisation
• Increase awareness of the disease (TB) and the demand for diagnosis and treatment services
• Expand service delivery through community-based approaches
• Enhance sustainability, accountability and community ownership of TB services
Activities for Social Mobilisation
- Group and community meetings - Engaging yuva/ mahila mandals, village health sanitation and nutrition committees under the National Rural Health Mission (NRHM), sensitization of local and religious leaders on TB and related stigma in the community. Regular meetings at the village level to address myths and misconceptions and help people with TB symptoms seek timely and appropriate care or referrals.
- School activities - Conducting TB awareness campaigns in schools by addressing the school assembly/ class, painting competitions, rallies, road shows, essay competitions, drawing competitions, exhibitions, dramas, pictorial presentations, quizzes, puzzles, puppet shows, leaflet distributions etc.
- Traditional media group performances - Performing entertainment-centred folk performances, street plays with scripts centred around TB awareness messages.
- Rallies and road shows - Spreading TB related messages on World TB day.
- Home visits - Encouraging interpersonal communication and empowering former TB patients and TB champions to become Directly Observed Treatment, Short-course (DOTS) providers.
Here, inter-personal communication and group communication are the main channels of communication for disseminating TB-related key messages.
In the National TB Elimination Programme (NTEP), partner NGOs play an important role in social/ community mobilisation. It generates dialogue, negotiation and consensus, engaging a range of players in interrelated and complementary efforts while taking into account people’s needs.
Resources
- Advocacy,Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
A roadshow was conducted by local PHC in a village on World TB day with message to End TB. This is an example of:
Policy making
Social mobilisation
Institutional strengthening
Diagnostics
2
Roadshow is one of the activities of social mobilisation strategy which aims at increasing awareness about the disease, involving major stakeholders.
ACSM goals for TB Elimination
ContentAdvocacy, Communication and Social Mobilization (ACSM) strategies are directed at achieving specific goals in terms of TB elimination.
They are:
- Setting and developing the policy based on the latest evidence
- Mobilizing political commitment and resources for TB
- Improving case detection and treatment adherence
- Widening the reach of services
- Combating stigma and discrimination
- Empowering people affected by TB and the community at large
It is useful to determine how ‘ideal behaviour’ in the community relates to these goals. The ‘ideal behaviour’ which is promoted through messages and ACSM strategies should be connected to the overall goal of the TB control programme. A few examples of this are:
- For the general public: Going to a healthcare provider at the first signs of possible TB infection (ideal behaviour) relates directly to the National TB Elimination Programme (NTEP) goal of increasing the case-detection rate for TB.
- For healthcare providers: Following the standards set for the treatment of TB – includes knowing what regimen, how to administer anti-tubercular therapy and what treatment path to take in case of multidrug-resistant or extensively drug-resistant TB. This relates to treatment adherence and outcomes.
The ACSM goals are planned in such a way as to achieve/ address:
• Structural or systemic issues (such as the lack of community Direct Observation Treatment, Short-course (DOTS) programmes)
• Communication interventions (such as behaviour change)
• Individual and social barriers (such as stigma, risk perception and knowledge among populations and health staff)
• Social mobilization activities that promote changes throughout a community or priority group.
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilization for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Seeking healthcare at the earliest symptom of TB directly relates to which goal of NTEP?
Mobilizing political commitment and resources for TB
Improving case detection
Widening the reach of services
Combating stigma and discrimination
2
Improving case detection is an important goal of NTEP and seeking health care early helps in the detection of more number of cases.
Yes Yes Target Audience for ACSM activities
ContentIdentifying target audience is a key step in the process of developing Advocacy, Communication and Social Mobilisation (ACSM) strategy.
Specific target audience need to be addressed to prevent hinderances in achieving the programme objectives.
Image
Figure: Steps in Identifying Target Audience for ACSM Activities
Target Audience for ACSM Activities
-
Advocacy
• Decision-makers at national, regional and district levels (National Health Mission officials, District Magistrate, National TB Elimination Programme leadership)
• Policy-makers
• Professional groups
• Funders
• Media
-
Communication
• General public, including different vulnerable groups, healthcare workers (i.e., primary healthcare providers, Allopathic and Ayurvedic, Yoga and Naturopathy, Unani, Siddha and Homeopathy (AYUSH) doctors, private healthcare providers, traditional healers, etc.)
• TB patients currently on treatment as well as cured TB patients
• Contacts of patients with active TB
• People at high risk of developing TB
-
Social mobilisation
• Communities
• Community groups, e.g., mahila mandals, youth groups
• National and local level leaders
• Local Non-government Organisations (NGOs), Youth organizations, Community-based Organisations (CBOs)
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Identifying target audience is crucial in the process of developing ACMS strategy.
True False 1 Specific target audiences need to be addressed to remove the causes/ reasons that are hindering programme objectives.
-
ACSM approaches
ContentOnce Advocacy, Communication and Social Mobilisation (ACSM) objectives are designed, linking them with activities strengthens the overall programme effectiveness. Several ACSM approaches can be considered for TB. Decisions on which approach or combination of approaches to use should take into account the benefits and risks, the time frame and the expertise and financial resources needed for effective implementation.
There are two parameters to determine:
(1) What ACSM activities to conduct?
(2) Which channels of communication to use?
Following are the various ACSM approaches relevant to the National TB Elimination Programme (NTEP) and the activities included in it:
NTEP Goal
ACSM Approaches
Activities & Channels
Gaining political commitment to TB elimination
- Educate national policy-makers and political leaders about the health and economic benefits of TB elimination. Aim to have TB declared a national health priority.
- Educate local and community level authorities to encourage them to contribute to TB elimination efforts.
- Solicit the support of international and national partners.
- Seminars and briefing meetings
- Print information (letters, fact sheets)
- Events around World TB Day and other occasions
Improving case detection
- Raise public awareness about TB.
- Reduce stigma against people with TB and correct misconceptions about TB infection by actively involving current and former TB patients.
- Help health workers, communities and individuals identify TB cases.
- Encourage individuals to seek care from appropriate sources.
- Target hard-to-reach populations (prisoners, urban poor, homeless).
- Formative research to determine the best messages and approaches
- Mass media including radio and television
- Distribution of print materials at community meetings or events
- Interpersonal communication and counselling training for health workers
- Community mobilisation activities
Increasing treatment success and discouraging the spread of Multidrug-resistant TB (MDR-TB)
- Give people with TB hope of complete cure.
- Encourage people with TB to seek treatment from appropriate sources.
- Provide materials to counsellors.
- Encourage people with TB to complete treatment even if they improve before treatment ends.
- Make people with TB aware of possible side effects, and where to seek care, if present.
- Encourage health workers, family and community members to directly observe people with TB taking their medicine.
- Engage people who are fully recovered to encourage people currently affected by TB to complete treatment.
- Interpersonal communication and counselling training for health workers
- Mass media, including radio and television
- Extensive distribution of print materials at healthcare facilities
- Community mobilisation activities
- Peer education at community or interest group meetings
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI. 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Factors to be considered while adopting an ACSM approach include:
Risks & benefits
Time frame
Expertise & financial resources
All of the above
4
Decisions on which ACSM approach or combination of approaches to use should take into account the benefits and risks, the time frame and the expertise and financial resources needed for effective implementation.
Yes
Yes
Communication channels
ContentThere are several communication channels for the effective dissemination of messages.
Below are various channels with their advantages and disadvantages listed.
Channels/ Tools Audiences Reached Advantages Disadvantages Mass media channels Television Households, families - Wider reach in urban and rural areas
- Maximum impact due to audiovisual elements
- Expensive production costs
- Less reach among rural and migrant populations, who are vulnerable to TB.
Radio Individuals, households, families - Radio production is simple and much less expensive than TV.
- Relatively wider reach than TV among rural and migrant populations.
- Accessible even on mobile phones
- Radio listening is no more popular; TV viewing/online portals are more popular.
Newspapers
and
magazines
Educated
individuals,
households
- Timely and fixed schedule of dissemination.
- Pictorial description of message.
- Not useful for the illiterate population
- People read newspapers for news about political developments, crime, etc., and not for advertisements per se, unless the advertisement is attractive and eye-catching enough.
Mid-Media - Outdoor Publicity Materials and Folk Arts/ Dramas Posters Individuals - Strong pictorial description of the message.
- Useful in high-traffic areas
- Brief messages
- Short lifespan
Pamphlets Individual - Good for communicating core messages with illustration/ visual support.
- Mass distribution and a kind of take-home message.
- Not very expensive.
- Can be used for repeated exposure and to reinforce messages broadcasted through mass media.
- Useful for the literate population, but can be used by the illiterate people as well
- If the pamphlet looks attractive enough, it is taken home and contents are deciphered with the help of literates or children at home/ in the neighbourhood.
Brochures Individuals, groups - Detailed information/ instructions with illustrations/ visuals/ graphs etc.
- Production costs may be relatively high.
Flip charts Individuals - Good support in counselling sessions.
- Production costs may be relatively high.
Wall writings/ hoardings Individuals, households - Useful in high-traffic areas.
- Good for identification, pictorial description and reinforcement of message
- Only for the literate population.
- Message retention is low
Kiosks Individuals - Face-to-face communication along with audio-visual communication for better message retention.
- Useful in dispelling myths and practices.
- Expensive to scale up.
- Requires trained staff.
- Relatively small reach.
Mobile vans and videos on wheels Groups, community - Entertaining and can grab audience attention and better message retention
- Expensive to implement and scale up
- Relatively small reach
- Requires precision of timing
Folk dramas Groups, community - Entertaining and can grab audience attention and better message retention
- Can touch an emotional chord with individuals/ households; useful for sensitisation.
- Relatively small reach.
- Expensive to scale up.
- Requires precision of timing.
- Requires good artists with prior training.
Interpersonal Communication (IPC) Counselling Individuals - Credible source due to face-to-face communication.
- Allows detailed explanation of key health messages.
- Can help dispel myths and check wrong practices.
- Time-taking to build reach.
- Small reach (individual).
- Costly to scale up.
- Requires special training.
Home visits Households - Credible source due to face-to-face communication.
- Allows detailed explanation of key health messages.
- Can help dispel myths and check wrong practices.
- Useful for rapport building.
- Time-taking to build reach.
- Small reach to the target audience.
- Requires adequate capacity building.
Community Dialogue Seminars, workshops, and Parliament questions Policy-makers, implementers, urban population - Brainstorming of key stakeholders.
- Identification of key communication challenges,
- Key inputs from experts and academicians.
- Not timely.
- High cost of implementation.
- Time-taking to bring about change.
- Difficulty in mobilizing key stakeholders.
Public meetings and gatherings Key
influencers,
individuals,
households
- Emphasis on key messages by influencers/ stakeholders.
- Useful for addressing different segments of the target audience together.
- Intermittent in occurrence.
- High organising cost.
- Only verbal communication involved.
- Reach is relatively small.
Working with groups Households,
individuals
- Dissemination of key messages among communities.
- Word-of-mouth communication.
- Low frequency.
- Only verbal communication involved.
Social Media Facebook, Blogs, YouTube, SMS Individuals - Targets individuals but has a wide/ mass reach.
- An effective method of reaching a large number.
- High visibility among decision-makers.
- Only limited people have access to internet accounts on Facebook, and an even smaller number have blogs.
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Home visits for communication are an example of: Mass media Interpersonal communication Community dialogue Mid-media approach 2 A home visit is a form of Interpersonal Communication (IPC).
- Credible source due to face-to face communication
- Allows detailed explanation of key health messages
- Can help dispel myths and check wrong practices
- Useful for rapport building
Yes Yes ACSM activities at different levels
ContentAdvocacy, Communication and Social Mobilization (ACSM) activities must place the individual at the centre and bring in the family, community and society to bring about sustained changes in TB perceptions and behaviours. ACSM activities must target these 4 groups accordingly:
- Individual: Specific interventions that ensure sustained engagement of people or individuals in maintaining positive behaviours/ changing to desired behaviours. E.g., counselling, use of positive TB messages, message by TB champions, etc.
- Family: Interventions that create an enabling environment for promoting positive behaviour change and developing necessary skills for a person affected by TB. E.g., counselling of the entire family.
- Community: Mobilizes groups toward a common goal, raises local resources and fosters support and awareness for TB-related issues. E.g., conducting TB awareness campaigns in public meeting places, melas, street dramas, etc.
- Society: Advocates for rights-based and socially inclusive approaches and seek support for the TB programme. E.g., workshops and seminars to drive change in legislation, policy, partnerships and resource allocation.
Aimed at individuals, families, communities, and the society, varied ACSM activities are undertaken at the national, state, district and community levels to:
- Create awareness and an enabling environment
- Build capacities to bring about desired changes in TB-related health behaviour
- Sustain positive behaviour
These are shown in the figure below.

Figure: ACSM Activities Spanning Across All Levels
Resources
- Operational Handbook on Advocacy, Communication, and Social Mobilization (ACSM), NTEP, 2014.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACSM activities span across which levels? Individual only. Individual, family, community, society and from central down to the village level. Individual and family levels only. ACSM activities do not span across any level. 2 ACSM activities must span across the individual, family, community, societal levels, and from the central down to the village level. ACSM planning format
ContentComponents of Advocacy, Communication and Social Mobilisation (ACSM) Planning Format
- Activity - The number of planned activities is mentioned against the timeline (for every quarter). Common activities listed in the format include community meetings, patient-provider meetings, school activities and outreach activities.
- Timeline - Timelines are divided into four quarters, but one must ensure that activities are spread across all the quarters and not aggregated in the last quarter of January–March.
- Budget - Budgeting for ACSM activities should cover materials, events, training, monitoring, evaluation, etc.
- Justification - The reason/ purpose for undertaking the ACSM activities is recorded.
The planning format also collects historical budgets proposed, allotted and spent for previous years to see if allotted budgets were properly utilised. The current allocation depends on the historical trend of spending.
Table: Example of ACSM Implementation Plan Format
Activity
Timeline
Budget
Justification/ Remarks
Q1
Q2
Q3
Q4
(Apr - June)
(July - Sep)
(Oct - Dec)
(Jan - Mar)
1. State Level
Image
Advocacy, Communication and Social Mobilisation
Justification/ Remarks
Activity
Budget Proposed in last annual action plan
(2012 – 2013)
Amount available in this Head (2012 – 2013)
Amount spent by district (2012 - 2013)
Approved ACSM Plan for 2013 -2014
Amount spent in 2013-2014 (till Sep 2013)
Permissible Budget as per population norm for 2014 - 2015
Budget proposed for 2013 - 2014
Total
0
Name of Activity
Number of activities undertaken in 2012-2013
Number of activities undertaken in 2013-2014 (till Sep 2013)
Number of Activities Proposed in 2014-15
Budget Proposed for Next FY 2014-2015
Apr-Jun
Jul-Sep
Oct-Dec
Jan-Mar
Total
Community meeting
0
Patient – provider meeting
0
School activity
0
Outreach activity
0
CME
0
0
0
0
Total
0
0
0
0
0
0
0
0
Resources
Assessment
Question
Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation How many components are there in the ACSM planning format? 3 4 5 2 2 Activity, Timeline, Budget and Justification are the key components of PIPs for ACSM. Developing ACSM Annual Action Plan
ContentThree Levels of Advocacy, Communication and Social Mobilisation (ACSM) Activities
- Preparation of district- and state-level Project Implementation Plans (PIPs) is an important component of the National TB Elimination Programme (NTEP) under the umbrella of the National Health Mission (NHM).
- State PIP is prepared annually which helps states in identifying and quantifying their targets for programme implementation during the year.
- This takes a bottom-up participatory approach that promotes need-based and decentralised planning.
Image
Figure 1: Bottom-up approach used in developing ACSM annual action plan
Steps in Planning ACSM PIP
- Draft of district PIPs are discussed in groups of 4–5 districts and ‘finalised’ as district PIPs.
- The district PIPs are consolidated into one document as the draft of state PIP by the IEC officer, in consultation with the STO and other concerned staff.
- In the process, the district PIPs and the state PIP are finalised and sent to Central TB Division (CTD) for approval.
- Once the state ACSM PIP and budget are approved by the CTD, the State IEC Officer (SIECO) should rework the state and district PIPs to reprioritise ACSM activities based on the allotted budget.
Image
Figure 2:Steps in Planning ACSM PIP
Abbr: DMC: Designated Microscopy Centre; PHI: Peripheral Health Institute; TU: TB Unit; DTO: District TB Officer; STO: State TB Officer; NTEP: National TB Elimination Programme.
Resources
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Planning of ACSM activities is a bottom-up approach. False True 2 ACSM project implementation plan takes inputs from all implementing levels - DMC, PHI, and TUs. Planning at the sub-district level starts as a bottom-up approach. Organising Community meetings
ContentCommunity meetings are organised by the Senior Treatment Supervisor (STS) or the partner Non-Government Organisation (NGO) under the supervision of the Medical Officer.
- These meetings are conducted to create awareness about TB among the general population, community leaders, people’s representatives, Self-help Groups (SHGs), community volunteers, traditional healers, etc.
- These meetings are organised in a community centre or any other suitable place at the village and slum level.
- To maximise the output, the community meetings should be planned appropriately.
Following are the steps involved in planning a community meeting:
Image
Resources
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who supervises the conduct of community meetings? DTO STO MO STLS 3 Community meetings are organised by the STS or the partner NGO under the supervision of the Medical Officer. YES YES Peer group interventions
ContentCommunity or peer-led measures penetrate better into the intricate layers of key population and facilitate Intensive Case Finding (ICF). Peer group support helps patients deal with challenges that they face during the treatment period. Several Tuberculosis (TB) patients find their treatment period stressful and having a peer to talk to, who has undergone similar challenges, and a doctor or counsellor to answer their questions, helps build confidence and realization that they are not alone in this journey.
Image
Figure 1: Characteristics of a Peer Group
Image
Figure 2: Peer group interventions has an influence on the knowledge, attitude, and quality of life of the pulmonary tuberculosis patients
-
Peer group intervention is human centered approach as it involves perspectives from the patients and their care givers encouraging them to openly discuss their concerns. Peer group intervention builds collective strength and solidarity among patients attending the group meeting and improve their treatment experience by learning from experience of peers. Talking to others in support groups reduces anxiety, improves self-esteem, and helps members' sense of well-being overall.
-
Peers are an underused resource for strengthening TB control among socially excluded populations. There is a need for further research into the contribution of peers to TB control, including analyses of economic effectiveness.
Peer group interventions for TB patients are:
-
Conducting patient support group meetings where patients and care givers can discuss their concerns and invite other patients who have addressed similar issues in their treatment. Social support from family and friends, helps in patient’s adherence to treatment. Treatment adherence is a key to the completion of TB treatment. The support is part of an external stimulus which can develop a particular behavior in human.
-
Peer group members can facilitate linkages to nutrition and other forms of support for TB patients – Patients or caregivers can be linked to support services like counselling, nutrition and social entitlements, either from the NTEP or through other public schemes or community structures.
-
Peer group members can help each other by sharing their knowledge to create linkages with the medical support systems – TB patients who develop side effects due to medication, should be linked for medical support during the meetings. Medical Doctor/STS/TBHV/CHO shall provide counselling to patients regarding side effects of the TB treatment and how to address the issues. Members act as role models for each other. Seeing others who are contending with the same adversity and making progress in their lives is inspiring and encouraging.
-
Peer group members can facilitate interactions of family members with Medical officer (M.O.)/National TB Elimination Programme (NTEP) staff – Peer group meetings can be used to counsel the caregivers on how to take care of the patient at home. A support group is a safe place for someone who needs to talk about intensely personal issues, experiences, struggles, and thoughts.
Resources
Guidance document on community engagement under NTEP Central TB Division, MoHFW, GoI September 2021
NTEP Training Modules 5 to 9, Central TB Division, MoHFW, GoI 2020
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Peers are an underused resource for strengthening TB control among socially excluded populations. There is a need for further research into the contribution of peers to TB control, including analyses of economic effectiveness.
True
False
1
Community or peer-led measures penetrate better into the intricate layers of key population and facilitate Intensive Case Finding (ICF).
-
ACSM activities in schools
ContentIn order to create awareness and mobilise young students to fight against TB, the National TB Elimination Programme (NTEP) encourages TB awareness campaigns in schools.
Common school activities undertaken to create awareness about TB among children include the following:
- Addressing the school assembly/ classes
- Holding painting competitions
- Holding rallies and road shows
- Holding essay competitions
- Holding slogan competitions
- Reading TB leaflets during prayers
- Organising quizzes
- Puzzle games
- Pictorial presentations (presenting TB-related information in the form of pictures)
- Organising exhibitions (posters, models etc.)
- Katputli shows
- Distributing leaflets containing information about TB
Steps for Organising School Activities
School activities could prove very effective, provided they are well planned. Following are the steps for effective organisation of school activities:
Image
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Training school teachers is a part of the ACSM activities in schools. True False
1
Training of school teachers, who will in turn conduct school activities in a planned manner is a part of ACSM activities in schools. YES
YES
Community mobilization strategies-Tribal areas
ContentTribal people (10.4 Cr, 8.6% of total population) have higher prevalence (703 per 100,000) of TB compared to national average (256 per 100,000).10.4% of all TB notified patients are from tribal communities. The National TB program has prioritized this subgroup of population through Tribal Action Plans since 2005.
As a part of the Multisectoral collaboration with various Ministries, a guidance note on the joint action plan was developed by Ministry of Health and Family Welfare (MoHFW) and Ministry of Tribal Affairs in October 2020 and shared with the Secretaries of all States/ UTs for field level implementation. Tribal TB initiative, a unique partnership between the Ministry of Health and Family Welfare and Ministry of Tribal Affairs was initiated to improve the cascade of TB care and support services among Tribal Populations in India. The technical assistance for this initiate will be provided by USAID.
Challenges in communities in tribal areas:
Access, availability, and utilization of TB care services of these communities are hindered by:
- Geographical barriers
- Poor state of social determinants
- High impact of malnutrition, insufficient community involvement
- Health system constraints including lack of trained human resources
- Cultural and communication gaps between the care provider and the community, etc.
- The COVID-19 pandemic has probably further worsened the situation.
Community mobilization strategies in tribal areas:
Image
Various departments which play a role in community mobilization in Tribal areas:
- National Program Management Unit (NPMU) provides technical assistance in monitoring and implementation of the Tribal TB Initiative.
- Coordination among National Tuberculosis Elimination Programme (NTEP), National Health Mission (NHM), Ministry of Development of Northeastern Region, Ministry of Tribal affairs at National, state and district levels through national level Technical Support Unit.
Image
- Coordination with ‘Centre of Excellence’ within the Ministry of Tribal Affairs, with a key focus on TB.
- Partnering with private sector players for leveraging resources for TB elimination in Tribal communities.
- Documenting best practices, and commission tribal health research studies in collaborations with identified government institutions.
- Various departments collaborate for improving the operational excellence of existing demand-side interventions such as Village Health Sanitation and Nutrition Days (and committees), Jan Arogya Samiti platforms, Jan Andolan initiatives, engaging TB-Champions, and training of faith healers and other community influencers.
Resource
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Community mobilization strategies in tribal areas include home visits. True False 1 Community mobilization is about seeking cooperation and support from different stakeholders in general and the community in specific.
Home visits will improve awareness on various government schemes, provisions, facilities available for TB patients and to improve treatment literacy and adherence among TB patients in tribal areas.
Community mobilization strategies-Rural areas
ContentRural populations have more limited access to primary care physicians than residents of urban areas, and are older, sicker, and poorer than urban counterparts. Travel to reach a primary care provider may be costly and burdensome for patients living in remote rural areas, with subspecialty care often being even farther away. These patients may substitute local primary care providers for sub specialists, or they may decide to postpone or forego care. Many social determinants act as barriers for rural communities to access health services.
Challenges faced by communities in rural areas are:
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
- Cultural and social norms surrounding health behaviors
- Low health literacy levels and incomplete perceptions of health
- Linguistic and educational disparities
- Limited affordable, reliable, or public transportation options
- Unpredictable work hours or unemployment
- Poor primary healthcare and infrastructure in rural areas
- Lack of access to tuberculosis testing and treatment centers in remote unreached areas
- Unregulated indigenous system of medicine
- Poor airborne infection control
- Poor nutrition and Malnourishment
Community mobilization strategies in rural areas include:
Image
Various committees which play a role in community mobilization in rural areas:
Image
- Village Health Sanitation and Nutrition Committees (VHSNCs) - In each Gram Panchayat, Village Health Sanitation and Nutrition Committees (VHSNCs) have been formed at the village level under National Health Mission (NHM). These committees are entrusted with community-level planning and implementation of health and sanitation, and have representation from the local government, local health centre, and the local community.
- Panchayat Raj Institution (PRI) - Members of PRI refers to local self-government at the village level. The village pradhan (head) and members of the Panchayat are elected members of the Gram Panchayat. They are the key people who can, after sensitization, mobilize the community for TB care and control and make allocations for TB patients’ nutrition and travel requirements.
- Yuva mandal/Mahila mandals (Youth/women’s clubs) - Community-level federations of young boys/girls/women, sometimes even comprising several women SHGs.
- Self-help groups (SHG) - An SHG is a group of individuals with a homogenous social and economic background, who voluntarily come together to regularly save small amounts of money and contribute to a local fund to meet the members’ emergency needs on a mutual help basis. These groups collectively manage their payments and ensure proper use of credits. Many NGOs currently engaged in the project are involved in formation/registration of these SHGs. It would be advisable to involve these NGOs for ease of implementation.
- Community-based organizations (CBO) - A CBO is a small group of people from a community, who come together for a particular purpose. It may be a local association of people mobilized around water conservation, mother and childcare, sustainable agriculture, education, or adolescent health; a group of social service persons; or any other such active group in a village.
Resource:
Assessment:
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Community mobilization strategies in rural areas includes empowering key decision-makers, people affected by TB, and marginalized and vulnerable populations.
True
False
1
This leads to raising awareness of services available and general health literacy surrounding TB.
More people accessing public health services will lead to better utilization of services.
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
Community mobilization strategies-Urban areas
ContentIndia has historically been called a rural economy but has witnessed fast-paced urbanisation in the last few decades. Currently, one-third of our population is urban. It is projected that by 2030, 46% of our population will be living in cities. Urban areas are characterised by high economic activity, diversity of livelihood opportunities and infrastructural development. Migrants are drawn to urban areas for employment opportunities and to establish a better life for themselves and their families.
Challenges faced by communities in urban areas: Most individuals and families living in urban areas face multiple and overlapping vulnerabilities. The vulnerabilities faced by urban people come from:
-
-
1. Residential vulnerability: Slum or slum-like habitations face the insecurity of tenure and are unserved or under-served with basic public services like sanitation, clean drinking water and drainage.
-
2. Occupational vulnerability: Urban residents working in the informal sector, daily wage labourers, factory workers working without adequate safety equipment, sanitation workers without adequate protective equipment and bonded labour are occupationally vulnerable.
-
3. Social vulnerability: Hinders access to resources such as health services, education and access to government schemes/ programmes because of societal discrimination. Widows, transgenders, the elderly, the disabled and those belonging to scheduled castes and tribes face discrimination because of their disadvantaged social status.
Social and systemic barriers to accessing public healthcare services in urban areas:
-
-
1. Limited availability of government primary healthcare services: Primary healthcare facilities in urban areas are limited in number. Urban residents have access to ‘larger’ or secondary/ tertiary hospitals (even for minor ailments) and private sector providers, paying heavily out of their pockets.
-
2. Overcrowding in public hospitals: Patients are forced to procure products and diagnostic services from other private providers due to lengthy waiting times.
-
3. Inconvenient timings: As most public health services open in the morning hours, consulting a doctor may mean the loss of a day’s wage for the poor. The alternative is to go to private doctors during evening hours.
Community mobilisation strategies for urban areas: Key strategies for community mobilisation in urban areas to facilitate improved case-finding, testing and treatment are given below.
-
-
1. Peer outreach at TB testing and treatment sites: Peer educators will be linked with TB service providers. These can be peers from a targeted intervention or HIV care and support programmes. Community or peer-led measures will penetrate better and facilitate Intensified Case Finding (ICF).
-
2. Mobile unit with the display of Information, Education and Communication (IEC) materials along with a facility for sputum collection and transportation.
-
3. Safe virtual or physical spaces (for example telephone hotlines, or drop-in centres) to seek information and referrals for care and support for TB treatment. Weekly/ fortnightly awareness sessions, testing days and follow-up testing days for TB can be organised in coordination with District TB Officers (DTOs).
-
4. Involvement of Community-based Organisations (CBOs)/ civil societies
Various departments/programs which play a role in community mobilisation in urban areas:

Resources
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Collaboration of National TB Elimination Programme (NTEP) and National Urban Health Mission (NUHM) is to develop strategies to address urban TB.
False
True
2
National Urban Health Mission integrates vertical health programs in its services. It makes special efforts to make its services accessible by the urban marginalized population through its location, service delivery, outreach and making its service providers sensitive to the needs of its target population.
-
IEC material for general public
ContentInformation, Education and Communication (IEC) material for the Public has been made available on the Central TB Division official website. In the home page of https://tbcindia.gov.in under the ACSM/IEC option IEC materials like launch video on World TB Day, Posters on TB Arogya Sathi, Ni-kshay Poshan Yojana, Ni-kshay Patrika, Documentaries, Radio Spots, TV Spots/TVC’s, Script for Nukkad Natak’s and Exhibition Panels are available in the public domain.
Image
Figure 1: IEC Material available in Public Domain: Source: tbcindia.gov.in
Information, Education and Communication (IEC) materials for the general public include:
- Mid-Media
- Banners
- Flip charts
- Wall writings
- Hoardings
- Posters
- Pamphlets
- Mobile vans and videos on wheels
- Folk performances
- Kiosks individuals - Face-to-face communication along with audio-visual communication for better message retention. Useful in dispelling myths and practices.
Image
Figure 2: Poster for TB Arogya Sathi App: Source: tbcindia.gov.in
Image
Figure 3: Poster for Nikshay Poshan Yojana: Source: tbcindia.gov.in
- Mass media
- Newspapers
- Television
- Radio
- Magazines
Image
Figure 4: Snapshots from a TVC’s: Source: tbcindia.gov.in
- Social Media
- Blogs
- YouTube
Image
Figure 5: Ni-kshay e-patrika: Source: tbcindia.gov.in
- Interpersonal Communication (IPC)
- Counselling
- Home-visits
- Community Dialogue
- Public meetings and gatherings
Image
Figure 6: Script for Nukkad Natak available on Central TB Division website: Source: tbcindia.gov.in
Resources
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Counselling and home visits are not part of the IEC materials/ tools available to the public. False True 1 Counselling and home visits are part of the interpersonal communication of the IEC strategy.
-
STLS: Community engagement in NTEP
FullscreenCommunity Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
Strategies of Community Engagement in NTEP
Content- Scaling up community participation in the National TB Elimination Programme through community-led activities and working with various community groups, especially TB survivors and key populations
- Empower TB survivors and affected populations to act as mentor’s/change agents and build their capacity for engaging them in programme planning, implementation and monitoring
- Working with community stakeholders to aid in early case identification amongst the vulnerable population
- Increasing accountability of the service delivery system through community participation
State TB Forum
ContentThe TB forum for community engagement aims to empower and engage the TB-affected community. The forum acts as a bridge between the community, TB patients, the health system and civil society. In these forums, advocacy activities are undertaken to influence policy changes for accessible, affordable, supportive TB services to the entire population with a special focus on poor and vulnerable groups.
Under the National TB Elimination Programme (NTEP), there are provisions for the constitution of state TB forums at the state level. The state TB forum consists of various stakeholders as shown in the table below. The meetings of these forums are to be convened at least every 6 months at the state level.
Table: Composition of the State TB Forum
Chairperson Principal Secretary / Secretary Health & Family Welfare, State Govt. Co-Chairperson Mission Director (National Health Mission) Members - Project Director, SACS
- Director Health Services
- WHO Representative – TB Consultant
- State Chairman/ Secretary, Tuberculosis Association of India
- Public Health Foundation of India/ any reputed public health institute
- State President, Indian Medical Association
- Professor of Pulmonary Medicine and Professor of Community Medicine of Medical Colleges
- Two representatives of reputed local NGOs/ CSOs on a rotation basis
- One representative from NTEP partners on a rotation basis (REACH/ UNION/ CHAI/ PATH/ FIND/ WHP/ KHPT)
- Representative of PLHIV Networks
- Five TB patient representatives (past TB patients/ family members)
- Representative of Corporate Sector/ Industry/ PSU
- State TB Officer
- One representative each from SACS, NPCDCS, SPMU, RCH, NUHM
Abbr: SACS: State AIDS Control Society; WHO: World Health Organisation; NGOs/CSOs: Non-governmental and Civil Society Organisations; NTEP: National TB Elimination Programme; WHP: World Health Partners, PLHIV: People Living with HIV; PSU: Public Sector Undertaking; NPCDCS: National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular diseases and Stroke; SPMU: State Programme Management Unit; RCH: Reproductive Child Health; NUHM: National Urban Health Mission Functions of the State TB Forum
- To advise on strategies for engaging communities affected by TB and increasing community participation in TB programs by forming a network of people affected by TB.
- To periodically review the progress of community involvement and network of people affected by TB.
- Highlight the concerns and needs of TB patients, work with the government and a broad range of individuals/ organisations to develop better and more responsive health services.
- Advocate for greater and more equitable access to quality, accurate and independent information for patients. To focus on reducing health inequalities by campaigning for patients to have the right to be involved in decision-making.
- Enable dialogue between all stakeholders involved in a TB patient’s care such as government (including local self-government), medical and paramedical associations, industry, medical insurance companies, private healthcare providers and diagnostic centres.
- Create and manage resources to sustain and accelerate TB prevention, control, care and treatment services through community engagement and a network of people affected by TB.
- Facilitate nutritional support, linkages with social welfare schemes, and rehabilitation of TB patients.
- Perform grievance redressal.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Concerning the state TB forum, which of the following is false? It is involved in engaging communities affected by TB at the state level. It is chaired by the person affected by TB. It has 33 stakeholders. It convenes meetings biannually. 2 State TB forums are chaired by the Principal Secretary/ Secretary HFW, State Govt. Yes Yes Local Self Government [LSG]
ContentLocal Self Government is the management of local affairs by local bodies who have been elected by the local people.
-
The local self-Government includes both rural and urban government.
Image
Figure 1: Types of local self government
Rural Local Governments:
-
Panchayati Raj Institution (PRI) is a system of rural local self-government in India. PRI was constitutionalized through the 73rd Constitutional Amendment Act, 1992. The panchayat raj system in the entire country is not the same but, by and large, structure of LSG in most of the States have the three-tier structure:
Image
Figure 2: Structure of Panchayati Raj
Urban Local Governments:
-
An urban area is usually a compact and densely populated area. All types of urban local governments are democratically elected by the people based on electoral wards.
-
Municipal administration is necessary to provide basic civic facilities like water supply, drainage, garbage disposal, public health, primary education, construction, and maintenance.
Image
Figure 3: Types of Urban local bodies
- Other types of urban local governments in India - Notified Area Committee, Town Area Committee, Cantonment Board, township, Port trust, Special purpose agency.
Role of Local Self Government in Health.
-
The common departments in the LSGs are General Administration, Finance, Public Works, Agriculture, Health, Education, Social Welfare, Information Technology, and others. Thus, LSG could play an important role in addressing the determinants of health.
-
LSGs play an active role in preventive healthcare services like vaccination, controlling drinking water and foods, mother-child health, disease screening programs, sanitation precautions, controlling of wastes and animal diseases, controlling of environmental factors that have disease risks such as air and water pollution. They are seen as critical to the planning, implementation, and monitoring of the NHM. Implementation of the NHM in achieving its outcomes is significantly dependent on well-functioning gram, block and district level panchayats.
-
LSGs also deliver services toward health promotion.
-
The other services provided by the LSGs are: Emergency and ambulance services, rehabilitation centers, elderly care centers and home care services
-
ASHA/USHA is one of the important functionary in health care service delivery and selected by the Gram Panchayat.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
The fundamental objective of Panchayati Raj system is to ensure which among the following?
1. People’s participation in development
2. Political accountability
3. Democratic decentralisation
4. Financial mobilisation
1,2,3
2,3
1,4
1,3
4
Panchayat Raj Institution (PRI) was constitutionalised to build democracy at the grassroots level and was entrusted with the task of rural development in the country. Active participation and vigilance on the part of the rural public is a must for the sustenance of democratic de-centralisation.
-
Role of LSG in TB Elimination
ContentLocal Self Governance is the management of local affairs by local bodies who have been elected by the local people. There are 2 types of Local Self Government (LSG): panchayats in rural areas and municipalities in urban areas. Local self-government (LSG) has deep connections and linkages with local people. Role of LSG in Tuberculosis (TB) elimination includes:
Image
Fig 1: Role of Local Self Government in TB Elimination
-
Awareness generation activities
With the participation of Panchayati Raj Institution (PRI) members in rural areas and municipalities in urban areas following awareness generation activities can be carried out:
- Health education on symptoms of TB, good cough etiquettes, available services for screening, diagnosis and treatment of TB, patient support/benefit schemes, TB in vulnerable groups (children, pregnant women, diabetic patients, patients on immunosuppressants, alcoholics and smokers) with emphasis on periodic screening for TB.
- Observance of World Tuberculosis Day on March 24
- Organize health-checkup camps and talks with the TB survivors
- Sensitize Panchayat Raj Institutions (PRI) members, faith leaders etc.
- Organize anti-stigma and non-discrimination campaigns
- Advocacy interventions
Local administration or Panchayat Raj Institutions (PRI) can be engaged in advocacy interventions to promote healthy behaviours and leverage support of TB patients:
- To install spitting bins.
- To install signages on good cough etiquettes.
- Free distribution of masks/handkerchief/tissues to TB patients in the community.
- Services for case finding (Active and latent TB Infection)
With the help of LSGs outreach activity can be planned and undertaken by community/non-governmental organizations (NGO) volunteers, Accredited Social Health Activist (ASHA) and Multi-Purpose Worker (MPW-Male)/ Auxiliary Nurse Midwife (ANM) under the supervision of the Community Health Officer (CHO)/Medical Officer- Urban Primary Health Centre (MO-UPHC), for case finding. These activities include:
- Vulnerability assessment
- Screening for symptoms of TB using Community Based Assessment Checklist (CBAC)
- Periodic active case finding among identified vulnerable populations
- Prompt referral of persons with TB symptoms to health center
- Treatment support and monitoring
- Local self governments can engage in formation and conducting meetings of treatment support groups.
- Health education for TB patients and their household contacts can be conducted on TB symptoms, treatment, managing adverse drug reactions, nutrition during house visits and treatment support group meetings.
- Counselling for TB patients and caregivers can be organised by PRI members and local administration.
- LSGs can mobilise funds from philanthropists to support the TB Patients, to supplement and augment healthcare facilities, screening and testing requirements, buying diagnostics and any other resources that might be required.
- TB preventive measures
- Under supervision of LSGs screening can be conducted of household/workplace contacts and other contacts of TB patients as eligible in the local context and identified vulnerable population for TB/latent TB infection.
- LSG can promote airborne infection control at workplaces and community settings.
- Interventions to ensure community participation
- LSGs can participate in identifying and training TB Champions and facilitate their participation in Village Health Sanitation Nutrition Committees (VHSNCs), Mahila Arogya Samitis (MASs), Jan Arogya Samitis and TB forum meetings.
- VHSNCs and MASs can discuss TB related issues in their meetings, conduct awareness programmes and extend support to case finding and treatment.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India 2020
- Pradhan Mantri Khanij Kshetra Kalyan Yojana (PMKKKY), Ministry of Mines, Government of India, 2015.
- Training Modules (5-9) for Programme Managers and Medical Officers, Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Local self-government can help in identifying and mapping socially and clinically vulnerable groups using available data from Municipal/ Block/ Taluka/ Zila Panchayats' records. Periodic drives can be conducted by them to identify and trace cases and link them to services provided under National Tuberculosis Elimination Programme (NTEP) and other social schemes.
True
False
1
Media advocacy by local self-government can engage the local media to disseminate information. With strategic communication and social mobilisation through Local self-government, the community members will help in gaining awareness about the services available in NTEP as well as other social schemes.
-
District TB Forum
ContentThe district TB forum is a community-engagement modality that aims to empower and engage the TB-affected community. Constituted by TB patients (cured or on treatment), community leaders, government officials, experts and NGOs; it gives a voice to the affected community and advocates with the programme managers for the resolution of challenges faced by TB patients in accessing TB services.
District TB forum is composed of various stakeholders as shown in the table below and its meeting is to be convened at least every 6 months at the district level.
Table: Composition of the District TB Forum
Chairperson District Magistrate Co-Chairperson Chief Executive Officer, Zilla Parishad Members - District Development Officer
- Chief Medical/ Health Officer
- WHO Representative – TB Consultant
- Representative of Tuberculosis Association of India
- Pulmonologist and Professor of Community Medicine of Medical Colleges
- District President, Indian Medical Association
- Two representatives of reputed local NGOs/CSOs on a rotation basis
- Representative from NTEP partners on a rotation basis (REACH/ UNION/ CHAI/ PATH/ FIND/ WHP/ KHPT)
- Five TB patient representatives (past TB patients/ family members)
- Representative of district-level PLHIV Network
- Representative Officer from RCH who manages NGOs
- District TB Officer
- PRI member (Zilla Parishad/ BDC/ Panchayat)
- Journalist
- Advocate
- Representative of the corporate sector
Abbr: WHO: World Health Organisation; NGOs/CSOs: Non-governmental and Civil Society Organisations; NTEP: National TB Elimination Programme; WHP: World Health Partners, PLHIV: People Living with HIV; RCH: Reproductive Child Health; PRI: Panchayati Raj Institutions; BDC: Block Development Council Functions of the District TB Forum
- To advise on strategies for engaging communities affected by TB and increasing community participation in TB programs by forming a network of people affected by TB.
- To periodically review the progress of community involvement and network of people affected by TB.
- Highlight the concerns and needs of TB patients, and work with the government and a broad range of individuals/ organisations to develop better and more responsive health services.
- Advocate for greater and more equitable access to quality, accurate and independent information for patients. To focus on reducing health inequalities by campaigning for patients to have the right to be involved in decision-making.
- Enable dialogue between all stakeholders involved in a TB patient’s care such as government (including local self-government), medical and paramedical associations, industry, medical insurance companies, private healthcare providers and diagnostic centres.
- Create and manage resources to sustain and accelerate TB prevention, control, care and treatment services through community engagement and a network of people affected by TB.
- Facilitate nutritional support, linkages with social welfare schemes, and rehabilitation of TB patients.
- Perform grievance redressal.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Concerning the district TB forum, which of the following is true? It is involved in engaging communities affected by TB at the state level. It is chaired by the person affected by TB. It has only 3 stakeholders. It convenes meetings biannually. 4 The district TB forum engages communities affected by TB at the district level is chaired by district magistrates, convenes meetings biannually, and comprises of various stakeholders. Yes Yes TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
Joint Effort for Elimination of Tuberculosis [JEET] Model of the Patient Provider Support Agency [PPSA]
ContentStudies have shown that nearly half of all patients with TB in India first seek care in the private sector, where there are significant gaps across the patient-care cascade, notably diagnostic delays, irrational and non-standardized regimens, and under-reporting to authorities. As a result, over a million cases of TB are missed in India every year. In order to address these challenges, project “Joint Effort for Elimination of Tuberculosis” (JEET) was envisaged. The key objective of this project is to set up effective and sustainable structures to strengthen existing systems and seamlessly extend quality TB care to patients in the private sector.
Patient Provider Support Agency (PPSA)
PPSA is one of the implementation Models under JEET Project and is responsible for continuous, end-to-end engagement of private sector to provide quality TB services to patients seeking care in private sector. The PPSA Model has the following key components:
1. Engagement of private providers
-
Network with private sector providers and promotes quality and early diagnosis,
-
Use of rapid diagnostics and Drug Susceptibility Testing (DST), TB notifications, and treatment as per Standards for TB Care in India (STCI)
-
Utilisation of available public sector services under the National TB Elimination Programme (NTEP) for the patients seeking care in the private sector.
2. Support engaged private sector providers for TB notifications in Ni-kshay
-
Through sensitisation
-
By establishing mechanisms/ modalities to support private sector notifications.
3. Linkage to free diagnostics services by the programme
-
All the presumptive TB cases are linked to free TB diagnostics services extended through a sample transport mechanism established under PPSA.
4. Linkage to free treatment services by the NTEP
-
Facilitates issue of NTEP Fixed Dose Combinations (FDCs) through engaged private sector practitioners and chemists
-
Facilitates linking patients to the public sector for initiation of treatment of Drug-sensitive TB (DS-TB) and Drug-resistant TB (DR-TB)
5. Support for treatment adherence
Adherence support is provided to patients through:
-
A team of treatment coordinators
-
NTEP provided Information and Communication Technology (ICT) enabled mechanism/ Call Centre for reminder SMS and phone calls.
6. Incentives to patients and private providers
-
NTEP provisioned incentives as per the National Strategic Plan (NSP) are provided to the engaged private providers and patients seeking care through them.
Image
Figure: The Service Delivery Model for PPSA
Patient Provider Support Agency Lite (PPSA lite)
An alternative model of PPSA called PPSA lite is implemented in 141 cities across seven states. City officers in PPSA lite cities/ districts support:
-
Mapping of private practitioners and identification of TB champions
-
Private sector provider engagement through Continuing Medical Education (CMEs)
-
Capacity building of NTEP staff to undertake private sector engagement.
-
Providing program monitoring support and facilitating reviews.
Resources
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Under PPSA treatment adherence support is provided to patients in the private sector.
True
False
1
Adherence support is provided to patients through a team of treatment coordinators and through NTEP-provided Information and Communication Technology (ICT) enabled mechanism/ Call Centre for reminder SMS and phone calls.
YES
YES
-
Patient-provider meetings
ContentPatient-provider meetings are important to ensure patient support and improve case holding/ treatment adherence.
Objective: To orient the patients on the course of the treatment, the importance of adherence and the risk for close contact. It also provides a platform to discuss the difficulty in following treatment courses by the patients and the need for further counselling if required.
Purpose: The purpose of this meeting is to counsel patients in a group who are on treatment or who are about to begin treatment. This is an opportunity for free interaction between providers and patients and also an opportunity for patients to clarify their doubts, if any.
Facilitators: These meetings are organized by the treatment supporter/ Directly Observed Treatment (DOT) provider. The Senior Treatment Supervisor (STS)/ Medical Officer (MO) are to conduct these meetings.
Target Group: Patients on treatment or who are about to begin treatment. There could be 5-10 patients (minimum) in such meetings. (If there is a large number of patients at one centre, small groups of about 10 patients may be made so that better interaction takes place between patients and providers).
Participants: Block medical officer/ Medical Officer - TB Control (MO-TC), field staff (STS, TB Health Visitor (TBHV), Senior TB Lab Supervisor (STLS)), general health system staff, patients and their attendees.
Place: These meetings are to be organized at the health facility.
Duration and Frequency: These meetings can be organized once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility.
- Each meeting can be for half-hour to one hour.
- The patient may be provided refreshments (tea, snacks etc.)
Note: Patient-provider interaction meetings are additional to, and are different from, interpersonal communication that the provider has with the patient while administering treatment.
Messages to be Provided to Patients
- Basic information about tuberculosis, cough etiquette, etc.
- Importance of completing treatment
- Side-effects of drugs and how to manage these
- Importance of follow-up sputum examination
- Prophylaxis for children in the family
- Do’s and don’ts including protective measures, the role of a nutritious diet, etc.
Health Communication Materials: Flip book, banner, posters on TB, etc., are to be provided and used during these meetings.
Report Writing: At the end of each meeting, a report may be prepared to state the date and time of meetings, number of patients, name of facilitators, presence of MO in the meeting, topics covered/ main points discussed in the meeting, along with major concerns mentioned by the patients.
- The report is to be prepared by the STS.
- The list of patients who attended the meeting may be attached to the report.
- It may be more convenient to have a register at each centre for such meetings, and patients can write their names in the same register.
- These may be submitted by STS to the MO-TC on a monthly basis for onward submission to the District TB Officer (DTO) to be included in the quarterly Performance Monitoring Report (PMR).
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Technical and Operational Guidelines for Tuberculosis Control, RNTCP, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How often should patient-provider meetings be conducted? Everyday Twice a year Once every month Once a year 3 Patient-provider meetings can be organised once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility. Yes Yes
-
Fullscreen























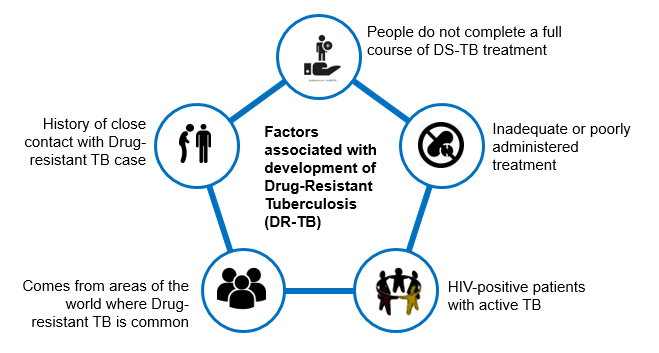




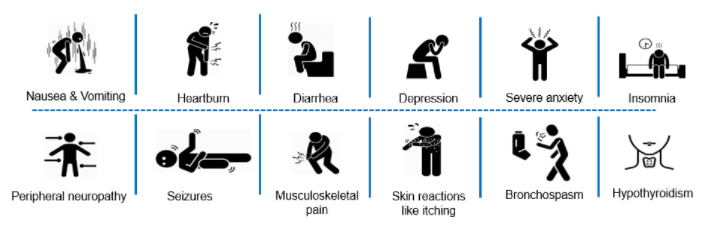

















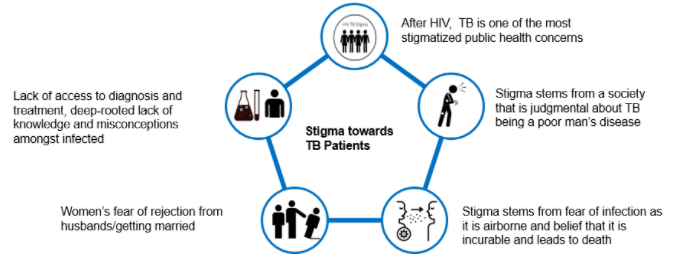

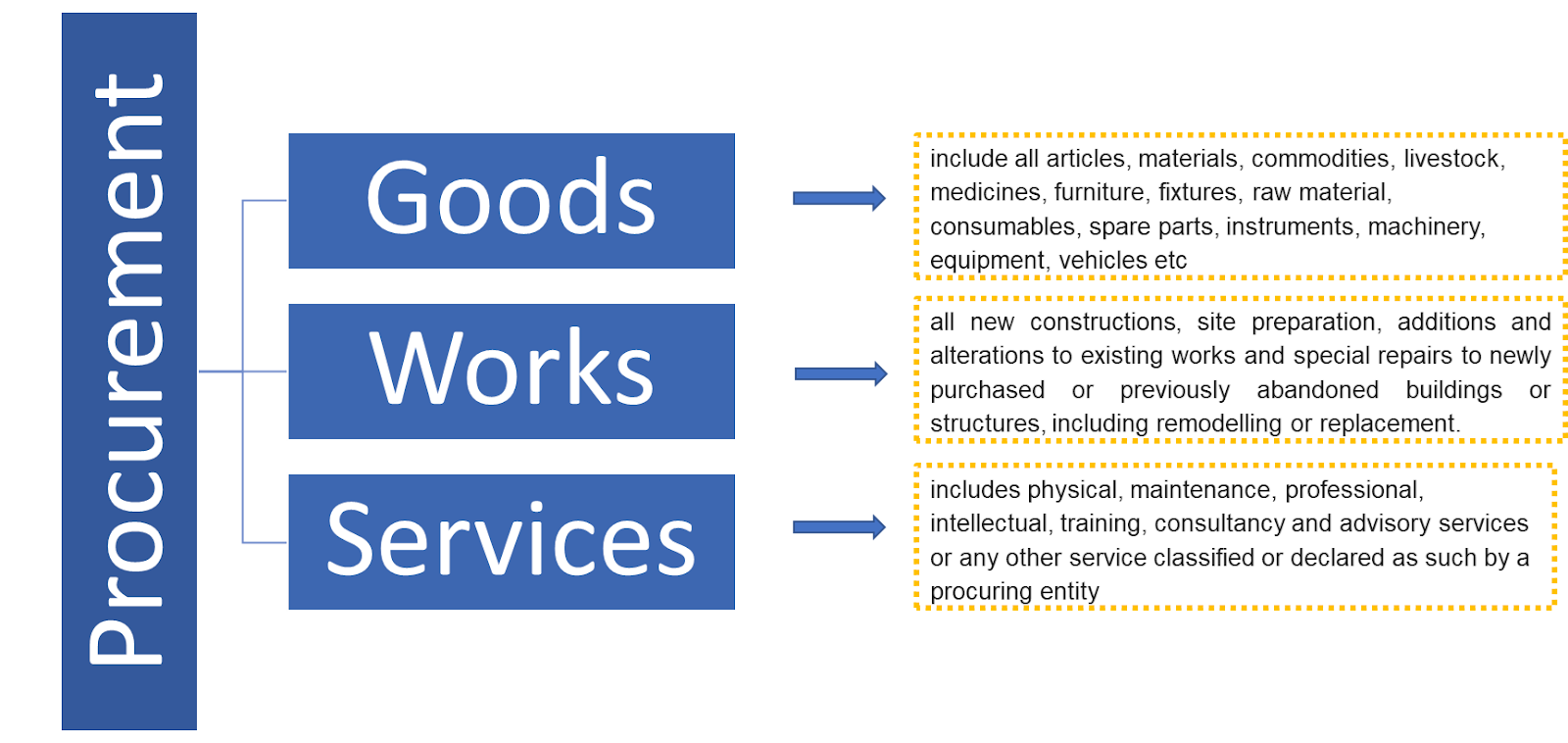






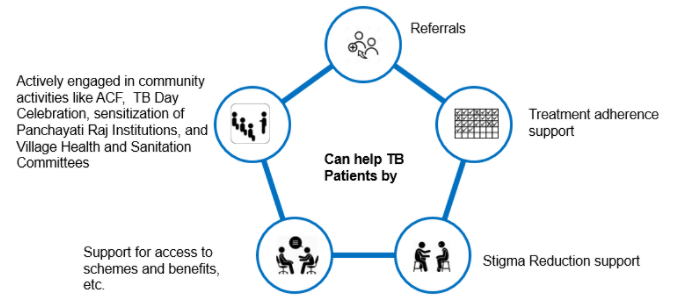
{kind=link}