-
STS: TB & TB Epidemiology
FullscreenTuberculosis
Content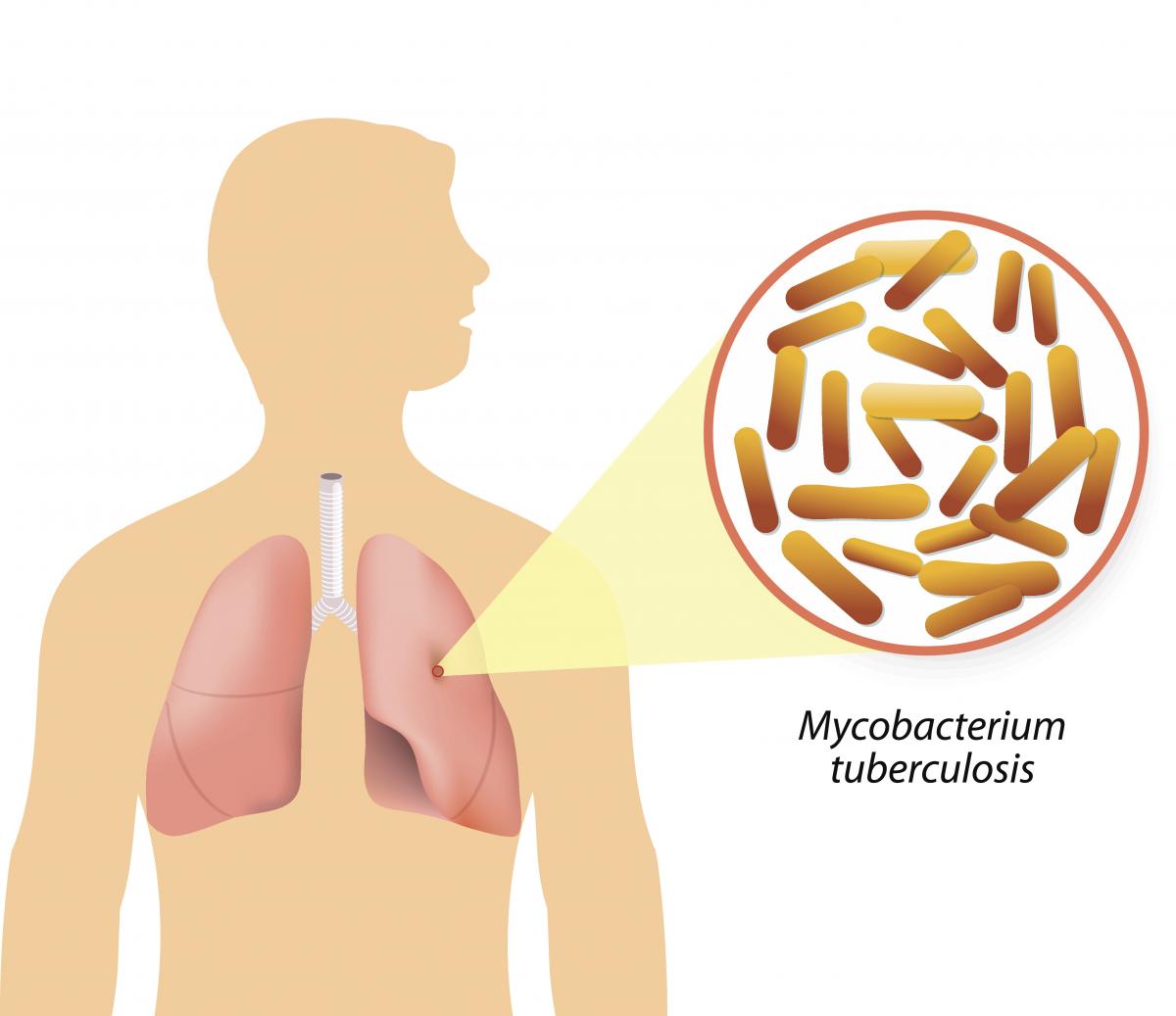
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB-HIV BURDEN
ContentThe interaction between HIV and TB in co-infected persons is bidirectional and synergistic; on the one hand, HIV infection predisposes the development of active TB, and, on the other, the course of HIV-related immunodeficiency is worsened by active TB infection.
Globally and in India, TB is the most common opportunistic infection seen in HIV patients and a leading cause of death in these patients. The lifetime risk of TB in immune-competent persons is 5-10%, whereas, in an HIV-infected person, the annual risk of TB is 5-15%. Thus, people living with HIV are 18 (15-21) times more likely to develop active TB disease than people without HIV.
TB and HIV Burden Trends in India
India is one of the WHO’s 30 high TB/HIV burden countries; of the 3 million TB incident cases, close to 54000 occurred in HIV-infected persons (See Table 1 for more details). TB and HIV are major public health challenges in India and are leading causes of mortality and morbidity among all other infectious diseases.
Table 1: Comparison between global and Indian TB/HIV burden estimates, Source: WHO Global TB Report 2022 INDICATORS GLOBAL ESTIMATES INDIA ESTIMATES Total TB Incidence 11 million 3 000 000 HIV-positive TB Incidence 703 000 54 000 HIV-positive TB Mortality 187 000 11 000 Resources
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Epidemiological Triad of TB
ContentThe Epidemiologic Triad is a model used in the field of epidemiology to study diseases and how they are spread. It consists of a triangle with three vertices or corners.
The three vertices for infectious diseases consist of:
1. Agent, or microbe that is the factor causing the disease.
2. Host, or organism harbouring the disease.
3. Environment, or those external factors that cause or allow disease transmission.
In the Epidemiological Triad of TB (Figure), the agent is the TB causing bacteria Mycobacterium tuberculosis; the host refers to humans that are susceptible to TB. Susceptibility or the risk factors for acquiring TB can be:
- Close contact with a person having TB disease
- Nutritional status of the host
- Existing co-morbidities
- Low immunity.
Susceptibility of the host can also vary due to age, gender, genetic composition, race, ethnicity, etc.
As TB is an airborne disease, environmental factors come into play for the transmission of TB. These include crowding, poor ventilation, bad sanitation, indoor air pollution, etc.
The understanding between the interplay of agent, host and environment is essential to understanding the epidemiology of TB and taking measures to control it. The risk of TB due to environmental factors can be reduced by practising airborne infection prevention measures like good ventilation, hand hygiene and cough etiquette.

Figure: Epidemiological Triad of TB
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The three vertices of the Epidemiological Triad are agent, host and environment.
TRUE FALSE 1 The three vertices of the Epidemiological Triad are agent, host and environment.
Yes Yes Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
Chemotherapy and its implication in TB control
ContentChemotherapy for TB is the use of an anti-TB drugs to kill, or prevent the replication of, TB mycobacteria in the patient’s body. Effective anti-TB chemotherapy renders the patient non-contagious and cures the patient, thereby interrupting the chain of transmission. Mortality rates of TB range from 50-80% in untreated smear-positive individuals and drop to lower than 5% under chemotherapy.
Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment. TB disease must be treated for at least 6 months and in some cases even longer. The use of multi-drug therapy reduces the incidence of drug-resistant cases and increases the overall effectiveness of treatment.
If treatment is interrupted, any surviving bacteria may cause the patient to later become ill and infectious again, potentially with drug-resistant disease.
How infectious are tuberculosis patients under chemotherapy?
Under effective chemotherapy, there is a substantial decline in infectiousness in two weeks time, and may not be a major source of risk to any contacts. This decline is indicated by the rapid fall in the number of viable organisms in the sputum, and reduced frequency of coughing.
Types of Chemotherapy in TB
- Preventive Chemotherapy: Regimen for healthy but TB infected persons with a high risk of developing TB, in order to prevent them from developing TB.
- Standard Chemotherapy: Two-phased chemotherapy for an average of 6-8 months based on the combination of at least four major drugs (HRZE) given for 2 months during the initial intensive phase of treatment and followed by a combination of at least 2 drugs given for at least 4 months during the continuation phase of treatment.
- Chemotherapy for Drug-resistant TB: Two-phased chemotherapy varying from 9 - 24 months in patients having demonstrated resistance to drugs used in standard chemotherapy. The regimen varies with the drug to which the resistance is present, however, each regimen contains a mix of second-line anti-TB drugs including injectables.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Infectiousness and Host Susceptibility, The Journal of Infectious Diseases, Vol. 216, suppl_6, 2017.
- Tuberculosis chemotherapy: Current Drug Delivery Approaches, Respiratory Research 7, Article no. 118, 2006.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which type of chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB? First-line anti-TB drugs Preventive Chemotherapy Standard Chemotherapy Chemotherapy for Drug Resistant-TB 2 Preventive chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB. Yes Yes Incidence of TB Disease
ContentIncidence is an epidemiological measure of the occurrence of new cases of a disease in a population over a specified period of time. Tuberculosis (TB) incidence is the number of new cases of active TB disease during a certain time period (usually a year), and is better expressed as a rate, as shown in the figure below.


Figure: Deriving the Incidence of TB Disease for a Given Population
Tuberculosis incidence varies considerably in different populations and population segments.
In 2021, the Global TB incidence was 134 (125-143) per 100,000. The TB Incidence rate of India is - 210 (178-244) per 100,000 in 2021 according to WHO Global TB Report 2022.
Resources
- India TB Report, 2022.
- Epidemiologic Basis of Tuberculosis Control, Hans L. Rieder, 1999.
- Morbidity Frequency Measures, Centers for Disease Control and Prevention.
- Global Tuberculosis Report 2022.
Prevalence of TB Disease
ContentPrevalence is an epidemiological measure of the proportion of a population with a disease or a particular health condition at a specific point in time (point prevalence) or over a specified period of time (period prevalence).
Tuberculosis (TB) prevalence refers to the number of people with TB that are present in a particular population at a given time. Calculation of the TB prevalence rate is shown in the figure below.

Figure: Deriving the Prevalence of TB Disease for a Given Population
TB prevalence rate is derived by adding the number of persons that develop new TB disease (i.e., incident cases) and those who already have the disease (i.e., existing cases), and dividing the sum by the total population from which the cases arose.
TB prevalence varies widely and is affected by a number of factors such as age, gender, population density, rural/urban settings, as well as socioeconomic factors.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
TB Notification rate
ContentTB notification rate is the number of TB cases notified over a specified time period for a specified population, usually per lakh. It indicates how many cases have been diagnosed and informed to the National TB Elimination Program.
It is mostly calculated annually, and the calculation formula is as follows:

Figure: Deriving the Annualized TB Case Notification Rate
The National TB Elimination Program calculates TB notification rates based on TB cases notified using the digital surveillance system called Nikshay. Each state/district is provided with an annual target for TB case notification, the progress of which is measured periodically to understand efforts taken for the detection of TB cases.
Example
If the number of TB patients diagnosed in District X one year is 1000, and the mid-year population of District X is 10,00,000, then the annualized TB case notification rate is calculated as follows:
100 cases/100 000/year
Resources
-
STLS: NTEP
FullscreenEnd TB strategy
ContentThe World Health Organisation End TB Strategy, adopted by the World Health Assembly in 2014, aims to end the global TB epidemic. The strategy draws on the opportunities presented by the Sustainable Development Goals (SDGs), especially those goals aimed at achieving universal health coverage and social protection from disease.
The table given below provides information on the vision, goal, milestones and targets for the End TB Strategy.
Table: Details on the End TB Strategy; Source: The End TB Strategy, World Health Organisation, 2015, p2. Vision of the End TB Strategy A world free of TB:
- Zero TB deaths
- Zero TB disease cases
- Zero suffering due to TB
Goal of the End TB Strategy To end the global TB epidemic by 2035 End TB Milestones for 2025 - 75% reduction in tuberculosis deaths (compared with 2015)
- 50% reduction in tuberculosis incidence rate (less than 55 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
End TB Targets for 2035 - 95% reduction in tuberculosis deaths (compared with 2015)
- 90% reduction in tuberculosis incidence rate (less than 10 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
The National Strategic Plan (2017-2025) proposes bold strategies with commensurate resources to rapidly decline TB in the country by 2030 in line with the global End TB targets to attain the vision of a TB-free India.
Resources
- National Strategic Plan for Tuberculosis Elimination 2017–2025.
- The End TB Strategy, World Health Organisation, 2015.
Sustainable Development Goals [SDGs] related to TB
Content
Figure: Summary of the Sustainable Development Goals
- Goal 3 is related to Good Health and Well-being. It mentions that 'Each nation needs to ensure healthy lives and promote the well-being of all ages'.
- The United Nations Sustainable Development Goals (SDGs) include ending the TB epidemic by 2030 under Goal 3.
- Goal 3.3: By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.
India is a signatory of the United Nations Sustainable Development Goals and has targeted TB elimination by 2025, five years ahead of the SDG timeline.
Resources
Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Training and Demonstration Centre [STDC]
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
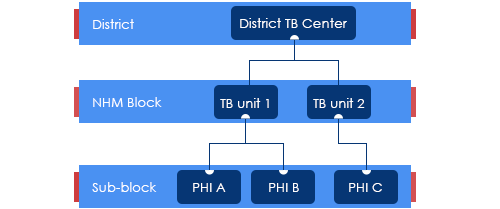
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Drugs Stores in NTEP
ContentImage
DRUG STORE
Central TB Division, MoHFW, has
Under NTEP, there is a large network of drug stores across the country to ensure a regular and uninterrupted supply of drugs and consumables. The Drugs and consumables are procured at the Central level and supplied at Central warehouses (GMSDs & CMSS); further drugs and consumables are supplied to the State Drug Stores and further dissemination to district and sub-district levels following the stocking norms to ensure uninterrupted supply of drugs and consumables to the patient.
To provide overall policy guidance and coordination, the Procurement and Supply Chain Management (PSM) Unit has been established at Central TB Division (CTD), MoHFW, for procurement and Supply Chain Management of all types of anti-TB drugs, diagnostics and consumables.
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Interaction of STLS with TB Patient Care Ecosystem
ContentThe Senior Tuberculosis Laboratory Supervisor (STLS) interacts with the TB patient care ecosystem from the time a presumptive TB case is identified, examined, diagnosed, notified, and put on anti-tuberculosis treatment till the completion of treatment.
The key interactions include:
- Coordination with the Medical Officer (MO) of various dispensaries and other health establishments to ensure referral of the presumptive TB cases to the Designated Microscopy Centers (DMCs) and Nucleic acid amplification test (NAAT) laboratories for diagnosis of TB and DR-TB.
- Coordination with laboratory technicians of the DMCs and NAAT laboratories for results of TB diagnosis, follow-up, and sending samples for further testing to the designated Intermediate Reference laboratories (IRLs).
- STLS is also responsible for providing monthly supply of staining regents, consumables, NAAT cartridges and chips to the LTs of the DMC and NAAT Laboratories.
- STLS is the key person for ensuring quality assured TB diagnosis in the district. This is done by performing activities like On-site evaluation (OSE) visits, Random Blinded Rechecking (RBRC) of smears and providing quality assured staining reagents to the DMCs.
- STLS is also responsible for providing monthly supply of staining regents, consumables, NAAT cartridges and chips to the LTs of the DMC and NAAT Laboratories.
- Coordination with Senior Treatment Supervisor (STS) to ensure that all TB patient diagnosed are initiated on treatment.
- Coordination with STS and PMDT Coordinator in updation of relevant NTEP records, line-list of presumptive DR-TB patients and preparation of Quarterly Reports
- The STLS interacts with the health care staff to facilitate change management with respect to use of Information and Communications Technology (ICT) and Ni-kshay tools for concerned data entry, validation & its use for public health action.
- STLS ensures that the laboratory results related to diagnosis and subsequent follow-ups are updated by the LTs in a timely manner.
- STLS ensures that the laboratory results related to diagnosis and subsequent follow-ups are updated by the LTs in a timely manner.
- STLS constantly Interacts with the District Drug Store (DDS), pharmacist and District TB Centre (DTC) to ensure adequate supply of CBNAAT cartridges and Truenat Chips to the NAAT laboratories and also keeps a track of transaction related to receipt and dispatch of these Cartridges and Chips.
- This process is undertaken by the use of Ni-kshay Aushadhi. SLTS uses Ni-kshay Aushadhi for request generation, inventory management, and issue of cartridges and Chips to NAAT laboratories.
- This process is undertaken by the use of Ni-kshay Aushadhi. SLTS uses Ni-kshay Aushadhi for request generation, inventory management, and issue of cartridges and Chips to NAAT laboratories.
- The STLS supports assigning treatment support centers and treatment supporters for the patient. The treatment supporters may be community volunteers accessible, willing, and acceptable to the patient and who can be accountable to the health system. These include Anganwadi workers, dais, teachers, panchayat leaders, religious leaders, and others.
- The STLS coordinates with District TB Officer (DTO) and DTC to conduct monthly and quarterly review meetings.
- The STLS is crucial in undertaking active case finding activities and organizing community-based Information, Education and Communication (IEC) activities like patient-provider group interaction meetings and community meetings in coordination with the support of field staff, which includes the ASHA workers, Community Health Officer (CHO), Multipurpose Health Worker (MPHW), and Auxiliary Nursing Midwife (ANM).
- The STLS coordinates with the private health care settings including the standalone laboratories in the districts to ensure that the patients diagnosed in these facilities are notified to the programme and appropriate public health action is taken when required.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test STLS helps the DTO in organising review meetings. True False True The STLS coordinates with District TB Officer (DTO) and DTC to conduct monthly and quarterly review meetings. - Coordination with the Medical Officer (MO) of various dispensaries and other health establishments to ensure referral of the presumptive TB cases to the Designated Microscopy Centers (DMCs) and Nucleic acid amplification test (NAAT) laboratories for diagnosis of TB and DR-TB.
-
STLS: Integration of NTEP with Health System
FullscreenNational Health Mission [NHM]
ContentThe National Health Mission (NHM) was launched by the Government of India in 2013, subsuming the National Rural Health Mission (NRHM) and National Urban Health Mission (NUHM). Figure 1 shows the history of the NHM.
The vision of NHM is “Attainment of Universal Access to Equitable, Affordable and Quality health care services, accountable and responsive to people's needs, with effective intersectoral convergent action to address the wider social determinants of health.”
Image
Figure 1: History and Make-up of the NHM; Source: Annual Report 2015-16, Ministry of Health and Family Welfare (MoHFW)
NHM further aims to support the existing national programmes of health and family welfare (Figure 2) including reproductive and child health, malaria, blindness control, iodine deficiency, filariasis, kala-azar, tuberculosis (TB), leprosy, and integrated disease surveillance.
Image
Figure 2: Health Programs Supported by NHM NHM and the National Tuberculosis Elimination Program (NTEP)
Integrating the NTEP with the health system increases the effectiveness and efficiency of TB care and control. India's TB control programme has been mainstreamed efficiently with the NHM.
The overall responsibility for the financial management of the NTEP is with the MoHFW, Director General of Health Services (DGHS) through the NHM.
At the state level, the State Health Society or its equivalent under the NHM of the state manages the financing of the TB Control Programme.
At the sub-district level, the TB Unit (TU) is the nodal point for TB control activities. TUs are based mainly in NHM health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
Resources
Medical Colleges
ContentMedical colleges in the country are integrated with the National TB Elimination Programme (NTEP) to widen access and improve the quality of TB services. Medical colleges provide specialized services for seriously ill TB patients.
The integration of medical colleges in the program is in a structured task force mechanism at different levels:
- National
- Zonal
- State
One national and six zonal task forces have been formed under the programme along with task forces for all states. A core committee is also formed in each medical college. These task forces are created with defined roles and responsibilities for the effective involvement of medical colleges in the programme.

Core Committee
Every medical college will have core committees representing various hospital departments and NTEP nodal officers. These committees meet quarterly and review the implementation of the program in the medical college.
Functions of the core committee:
- They organise sensitisation workshops and training for faculty members, postgraduates, undergraduates, interns, paramedical staff, etc.
- Ensure that teachings on TB/ NTEP form part of the curriculum for all medical colleges.
- Coordinate between various departments so that patients get the services under one roof.
- Coordinate with the district TB programme.
Role of Medical College in NTEP
- Medical colleges coordinate with the district TB programme for participation in quality assurance, supervision, monitoring, review and evaluation.
- Operational research is one of the important activities of medical colleges.
- Every medical college should have TB detection facility and treatment support centres. These centres are equipped with trained additional human resources such as medical officers, laboratory technicians and TB health visitors.
- The National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients.
- Medical colleges undertake advocacy for the programme.
- Medical colleges also functions as peripheral health institutes (PHI), maintain TB notification registers and submit monthly PHI reports: They have Nikshay user access and need to enter TB-related data on a real-time basis.
Resources
RNTCP Technical and Operational Guidelines for Tuberculosis Control in India, 2016.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Every medical college should have a DR-TB facility? True False 1 National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients. Need for integration of NTEP with Health System
Content-
The public health system in India through the National Health Mission (NHM) visualises the attainment of Universal Health Coverage (UHC) for all its citizens, which provides access to equitable, affordable and quality health care services, which is also accountable and responsive to the needs of the people.
-
Under the umbrella of NHM, the National TB Elimination Programme (NTEP) ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI).
-
Furthermore, the NHM, under the Ayushman Bharat initiative has taken measures to strengthen the primary care facilities including Primary Health Centres (PHCs) and Sub Health Centres (SHCs) in the Ayushman Bharat Health & Wellness Centres (AB-HWCs).
Need for integration of NTEP with the Health System at Different Levels
- Closer to community TB Services: The integration of TB services with the health system provides an opportunity for the TB programme to leverage the resources under the Ayushman Bharat initiative to take TB interventions closer to the community which were otherwise provided at the primary care level.
- Improved population coverage: Active empanelment and HWC database will help to monitor and identify the left-out population and contribute significantly to the NTEPs case finding activity coverage.
- Improved population health outcomes: Improved availability, access and utilisation of advanced TB treatment services under the ambit of UHC is essential in reducing morbidity and mortality from TB which may in turn also contribute to overall equitable health outcomes.
- Reduced out-of-pocket expenditure: The integration will improve the access to TB services, assure within-reach TB medicines and diagnostic services, provide linkages for care coordination with Medical Officers/ specialists across various levels of care, etc., all of which will reduce the catastrophic expenditures faced by the patients and their families.
- Decreased crowding at the secondary and tertiary health facilities: A strong network of peripheral level TB care services would facilitate in reduction of the overcrowding and the case burden at the secondary and tertiary facilities, which could be utilised for cases with follow-up referral to higher level facilities.
- Increased responsiveness and addressal of social determinants of TB: Provision of TB treatment at the nearest point of care for the communities and engaging the most peripheral workers from the health system like the Accredited Social Health Activists (ASHA) in the TB programme may lead to comfort in accessing the care by the patients and also enable addressing psycho-social determinants of TB.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, CTD, MoHFW, India, 2020.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). True False 1 Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). Yes Yes -
Fullscreen
