-
CHO-M1: Basics of TB and NTEP
Fullscreen-
CHO-CH1: TB & TB Epidemiology
FullscreenTuberculosis
Content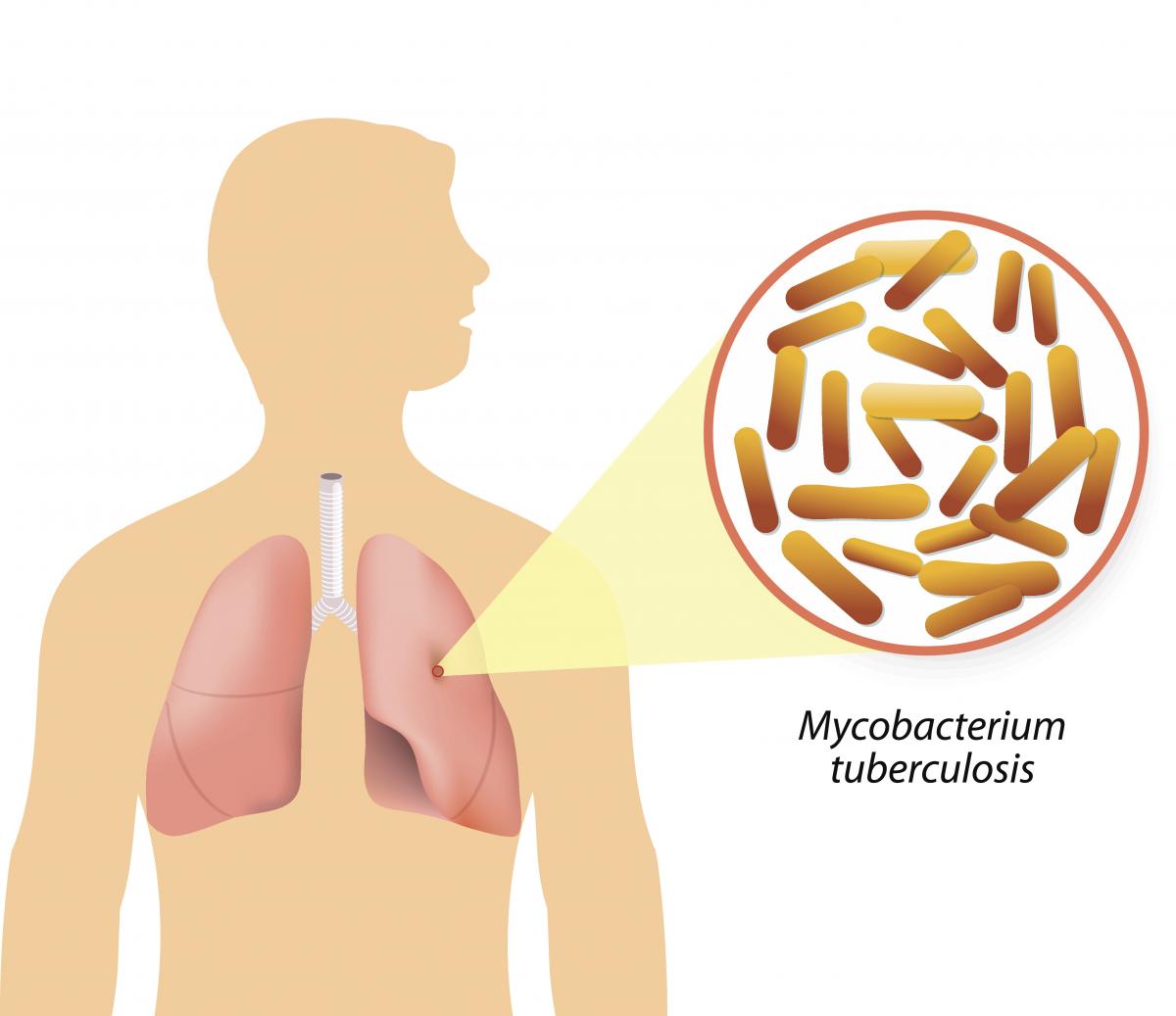
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB-HIV BURDEN
ContentThe interaction between HIV and TB in co-infected persons is bidirectional and synergistic; on the one hand, HIV infection predisposes the development of active TB, and, on the other, the course of HIV-related immunodeficiency is worsened by active TB infection.
Globally and in India, TB is the most common opportunistic infection seen in HIV patients and a leading cause of death in these patients. The lifetime risk of TB in immune-competent persons is 5-10%, whereas, in an HIV-infected person, the annual risk of TB is 5-15%. Thus, people living with HIV are 18 (15-21) times more likely to develop active TB disease than people without HIV.
TB and HIV Burden Trends in India
India is one of the WHO’s 30 high TB/HIV burden countries; of the 3 million TB incident cases, close to 54000 occurred in HIV-infected persons (See Table 1 for more details). TB and HIV are major public health challenges in India and are leading causes of mortality and morbidity among all other infectious diseases.
Table 1: Comparison between global and Indian TB/HIV burden estimates, Source: WHO Global TB Report 2022 INDICATORS GLOBAL ESTIMATES INDIA ESTIMATES Total TB Incidence 11 million 3 000 000 HIV-positive TB Incidence 703 000 54 000 HIV-positive TB Mortality 187 000 11 000 Resources
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
-
CHO-CH2: NTEP
FullscreenIndia's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Demonstration and Training Centre [STDC]: Organogram and Human Resources
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
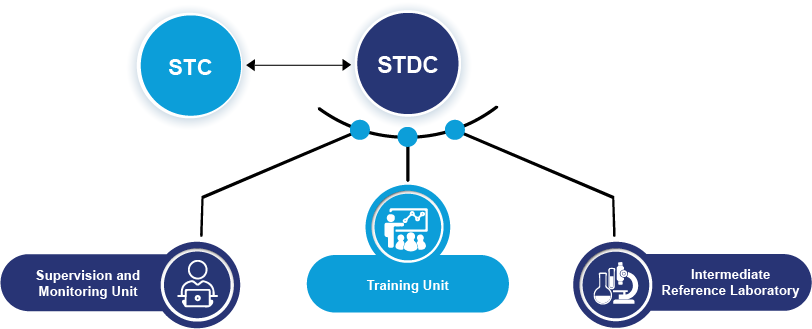
Figure: STDC and its Supporting Units
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
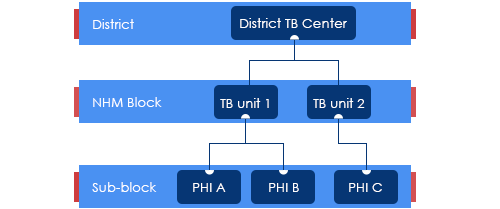
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Drugs Stores in NTEP
ContentImage
DRUG STORE
Central TB Division, MoHFW, has
Under NTEP, there is a large network of drug stores across the country to ensure a regular and uninterrupted supply of drugs and consumables. The Drugs and consumables are procured at the Central level and supplied at Central warehouses (GMSDs & CMSS); further drugs and consumables are supplied to the State Drug Stores and further dissemination to district and sub-district levels following the stocking norms to ensure uninterrupted supply of drugs and consumables to the patient.
To provide overall policy guidance and coordination, the Procurement and Supply Chain Management (PSM) Unit has been established at Central TB Division (CTD), MoHFW, for procurement and Supply Chain Management of all types of anti-TB drugs, diagnostics and consumables.
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Interaction of STS with TB Patient Care Ecosystem
ContentThe Senior Treatment Supervisor (STS) interacts with the patient care ecosystem from the time a TB case is notified, diagnosed and anti-TB treatment is initiated.
The key interactions include:
- Coordination with laboratory technician and Senior TB Lab Supervisor (STLS) for results of TB diagnosis, follow-up, diagnosis, sending samples for drug susceptibility testing whenever required.
- Clinical evaluation of the patient by a Medical Officer (MO) and follow-up evaluation.
- The STS conducts home visits to provide health education and counselling on nutrition and treatment adherence to the patient and family/ caregivers, and for monitoring treatment progress till successful completion of treatment.
- The STS supports the health facility staff to update the information of patients on Nikshay, including on comorbidity, treatment adherence, treatment outcome, contact investigation and their TB Preventive Treatment (TPT).
- Interactions with the District Drug Store (DDS), pharmacist and District TB Centre (DTC) to ensure an adequate supply of drugs for the patient.
- Uses Nikshay Aushadhi for drug request generation, managing drug inventory, dispatch and issue to patients.
- The STS supports assigning treatment support centres and treatment supporters for the patient. The treatment supporters may be community volunteers accessible, willing and acceptable to the patient and who can be accountable to the health system. These include Anganwadi workers, dais, teachers, panchayat leaders, religious leaders, and others.
- The STS coordinates with District TB Officer (DTO) and DTC to ensure the disbursement of incentives to patients under Nikshay Poshan Yojna, incentives to treatment supporters and travel incentives to Drug-resistant TB (DR-TB) patients.
- The STS is crucial in organising community-based Information, Education and Communication (IEC) activities like patient-provider group interaction meetings and community meetings in coordination with the support of field staff, which includes the Community Health Officer (CHO), Multipurpose Health Worker (MPHW), Auxiliary Nursing Midwife (ANM).
- STS works in coordination with the DR-TB coordinator to ensure diagnosis, pre-treatment evaluation, treatment initiation, adherence and follow-up for all DR-TB patients.
- Ensures standards of TB care in India are followed for patients diagnosed in private health facilities.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Module for Senior Treatment Supervisors, RNTCP, CTD, 2005.
- Guidelines for PMDT in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The STS supports assigning treatment support centres and treatment supporters for the patient. True False 1 The STS supports assigning treatment support centres and treatment supporters for the patient. Yes Yes
-
CHO-CH3: Integration of NTEP with Health System
FullscreenNeed for integration of NTEP with Health System
Content-
The public health system in India through the National Health Mission (NHM) visualises the attainment of Universal Health Coverage (UHC) for all its citizens, which provides access to equitable, affordable and quality health care services, which is also accountable and responsive to the needs of the people.
-
Under the umbrella of NHM, the National TB Elimination Programme (NTEP) ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI).
-
Furthermore, the NHM, under the Ayushman Bharat initiative has taken measures to strengthen the primary care facilities including Primary Health Centres (PHCs) and Sub Health Centres (SHCs) in the Ayushman Bharat Health & Wellness Centres (AB-HWCs).
Need for integration of NTEP with the Health System at Different Levels
- Closer to community TB Services: The integration of TB services with the health system provides an opportunity for the TB programme to leverage the resources under the Ayushman Bharat initiative to take TB interventions closer to the community which were otherwise provided at the primary care level.
- Improved population coverage: Active empanelment and HWC database will help to monitor and identify the left-out population and contribute significantly to the NTEPs case finding activity coverage.
- Improved population health outcomes: Improved availability, access and utilisation of advanced TB treatment services under the ambit of UHC is essential in reducing morbidity and mortality from TB which may in turn also contribute to overall equitable health outcomes.
- Reduced out-of-pocket expenditure: The integration will improve the access to TB services, assure within-reach TB medicines and diagnostic services, provide linkages for care coordination with Medical Officers/ specialists across various levels of care, etc., all of which will reduce the catastrophic expenditures faced by the patients and their families.
- Decreased crowding at the secondary and tertiary health facilities: A strong network of peripheral level TB care services would facilitate in reduction of the overcrowding and the case burden at the secondary and tertiary facilities, which could be utilised for cases with follow-up referral to higher level facilities.
- Increased responsiveness and addressal of social determinants of TB: Provision of TB treatment at the nearest point of care for the communities and engaging the most peripheral workers from the health system like the Accredited Social Health Activists (ASHA) in the TB programme may lead to comfort in accessing the care by the patients and also enable addressing psycho-social determinants of TB.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, CTD, MoHFW, India, 2020.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). True False 1 Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). Yes Yes -
NTEP Integration into Public Health System
ContentIntegrated patient-centred care and prevention are one of the pillars of the End TB strategy. This requires TB services to be made affordable and accessible by integrating them with the general health system.
In 2005, the National Rural Health Mission (NRHM) was established and was merged with the National Urban Health Mission (NUHM) in 2013, to form the National Health Mission (NHM).The National TB Elimination Programme (NTEP) is a flagship programme under the NHM and fund allocation to NTEP occurs through the NHM.
NTEP integrates with the public healthcare system at various levels as follows:
- Community level – Accredited Social Health Activists (ASHA)/ Community Health Volunteers (CHVs)/ Multipurpose Workers (MPWs)
- Ayushman Bharath Health and Wellness Centre - Sub Health Centre (ABHWC - SHC)
- Ayushman Bharath Health and Wellness Centre - Primary Health Centre (ABHWC - PHC)
- Community Health Centre (CHC)
- District/ Taluka hospital
- Medical Colleges
- Other health institutions in the public sector – ESI, railways, ports and the ministries of mines, steel, coal, etc.
Note: As far as NTEP is concerned, a Peripheral Health Institution (PHI) is a health facility headed by a Medical Officer
TB services are provided free of cost through the public health system.
Services provided include:
- Advocacy, Communication and Social Mobilisation (ACSM) and Information Education and Communication (IEC)
- Screening for TB – Active Case Finding (ACF), Passive Case Finding (PCF), Intensified Case finding (ICF)
- Diagnosis of TB and drug resistance – Designated Microscopy Centre (DMC) or TB diagnostic centres. Some of the PHIs themselves act as DMCs or Sputum Collection Centres
- Treatment for DS-TB and H Mono/Poly DR-TB through PHIs
- Treatment for DR-TB through District/Nodal DR-TB Centres
- Treatment Support through out treatment course
- Clinical follow-up and comorbidity management
- Referral services for those with Adverse Drug Reactions (ADRs)
- Screening for Tobacco and Alcohol addiction and linkage to de-addiction services
- TB preventive therapy
- Data management in Ni-kshay
References
- Technical and Operational Guidelines for Tuberculosis, 2016.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
- Detect-Treat-Prevent-Build: Strategy for TB Elimination in India by 2025, Indian J Community Med., 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these is included in the TB services available at sub- centre level?
Providing treatment support and follow-up of TB cases in the sub- centre area
Conducting ACSM and IEC activities
Refering TB symptomatics to the nearby DMC/ TDC
All of the above
4
Services at ABHWC – SHC level include:
- Conduct ACSM and IEC activities
- Conduct case-finding activities in the catchment area of the centre – Active/ Passive/ Intensified
- Refer TB symptomatics to the nearby DMC/ TDC
- Linkage of positive DS-TB cases to the nearest PHC for initiation of TB treatment
- Referral of DR-TB cases to the nearest Nodal DR-TB Centre for treatment
- Treatment support and follow-up of TB cases in the sub- centre area
- Liasoning with the STS and MOTC for TB control activities in the area
- Facilitates data entry in Ni-kshay.
Yes
Yes
Ayushman Bharat Health and Wellness Centres
ContentAyushman Bharat (AB) is an attempt to move from a selective approach to health care to deliver comprehensive range of services spanning from preventive, promotive, curative, rehabilitative and palliative care. AB-HWCs are envisaged to deliver expanded range services that go beyond maternal and child health care services to include care for non-communicable diseases, palliative and rehabilitative care, oral, eye and ear nose and throat care, mental health and first level care for emergencies and trauma, including free essential drugs and diagnostic services.
It has two components which are complementary to each other.
- Under its first component, 1,50,000 Health and Wellness Centres (HWCs) will be created to deliver Comprehensive Primary Health Care, which is universal and free to users, with a focus on wellness and the delivery of an expanded range of services closer to the community.
- The second component is the Pradhan Mantri Jan Arogya Yojana (PM-JAY) which provides health insurance cover of Rs. 5 lakhs per year to over 10 crore poor and vulnerable families for seeking secondary and tertiary care.
On 14th April 2018, the Honorable Prime Minister of India launched the first Health and Wellness Centre at Jangla, Bijapur, Chhattisgarh. Health Sub-Center (HSC), PHC (Primary Health Center) and Urban PHCs are currently being upgraded to reach a goal of 1.5 lakhs AB-HWC by 2022.
The National TB Elimination Program (NTEP) has also integrated TB services as part of the health and wellness center service delivery package.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, MoHFW, 2021.
- Ayushman Bharat - Health and Wellness Centre Website, Government of India.
Kindly provide your valuable feedback on the page to the link provided HERE
-
CHO-CH4: Patient Management
FullscreenOverview of the Patient Management Workflow in Nikshay
ContentNikshay is an integrated Information, Communication and Technology (ICT) platform adopted by the National Tuberculosis (TB) Elimination Programme (NTEP) for TB patient management and care.
The patient management workflow in Nikshay streamlines a series of activities required for TB patients from identification of presumptive TB cases to recording treatment outcomes. Nikshay uses in-built modules in the platform to perform these tasks. There are also different user logins that allow certain functions (see figure below).
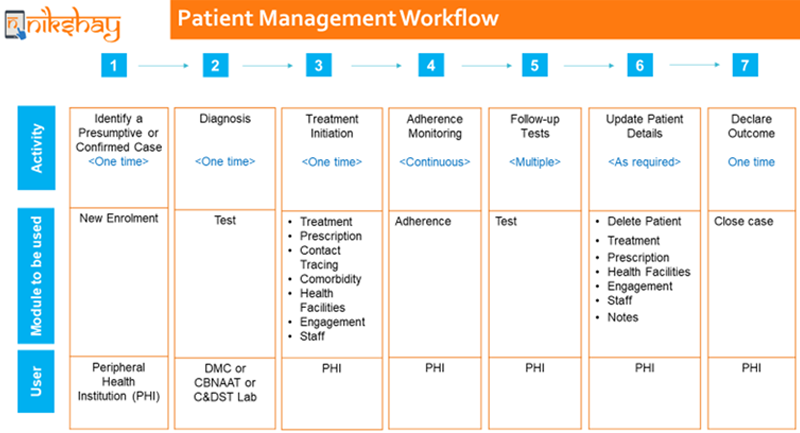
Figure: Overview of the TB Patient Management Workflow in Nikshay; Source: Module 1: Introduction to Nikshay

Summary of the Patient Management Workflow in Nikshay
STEPS ACTIVITY AND NIKSHAY MODULE DETAILS 1 Identify a presumptive or confirmed TB case and notify that case using the New Enrolment Module.
- A Nikshay ID will be generated for the patient upon enrolment, which will be unique and used for the entire TB care life cycle of that patient.
2 Request for diagnostic tests using the Test Module.
- On receiving test results, update it using the patient’s Nikshay ID, irrespective of whether they are positive or negative.
- Once diagnosed positive for TB, notify the patient as a confirmed TB case.
3 Initiate treatment by entering treatment information in Treatment Prescription, Contact Tracing, Comorbidity, Health Facilities, and Engagement Staff Modules. 4 Enter adherence monitoring details in the Adherence Module. 5 Request for follow-up tests using the Test Module. Update test results using same processes in Step 2. 6 Update patient details as required using Modules like Delete Patient, Treatment, Prescription, Health Facilities, Engagement, Staff, Notes. 7 Declare outcome upon receiving treatment outcome details of patient in the Close Case Module. Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Patient management in Nikshay
ContentVideo fileVideo: Patient Management in Ni-kshay
Enrolling a patient in Nikshay
ContentVideo fileDeduplication while enrolling a new patient
ContentVideo fileVideo: Deduplication while enrolling a new patient - Web
Video fileVideo: Deduplication while enrolling a new patient - Mobile
Searching and viewing patient lists
ContentVideo fileVideo: Searching and viewing patient lists
Requesting a Test on Nikshay
ContentOnce a presumptive TB patient is identified, the patient is enrolled online by a healthcare worker or doctor in Nikshay online portal. For diagnosis of Tuberculosis, the treating physician can request a test utilizing the request test option of Nikshay online portal. The step-by-step approach for test request is as follows:
Step 0: Go to the Patients Page.
Step 1: Select the “Tests” tab.
Step 2: Click the “Add Test” button.
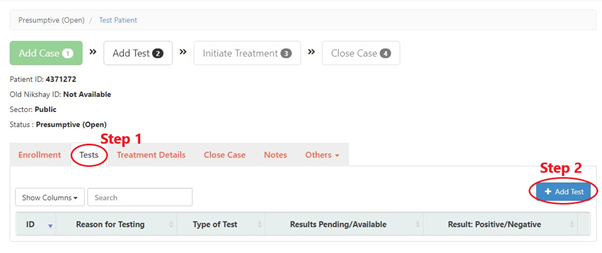
Step 3: Fill the form.
Step 4: Select the “Test Status” as “Results Pending”.
Step 5: Click the “Add Test” button by selecting the appropriate test for the patient.
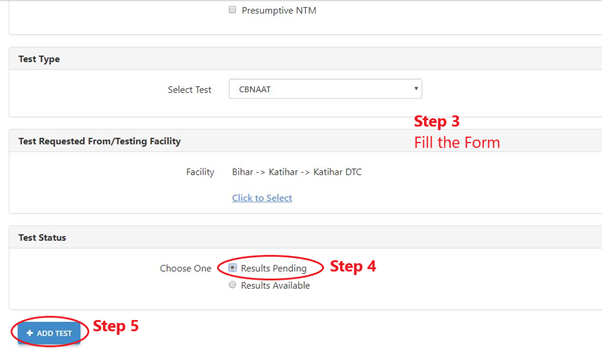
In a situation where the patient is referred to another health facility for TB testing, one needs to select the test requested along with the facility name where the patient will visit for undergoing the TB test. the results are added by the concerned healthcare worker only after the test is conducted and the result is available.
In the absence of such results, it will show ‘Result pending’ instead of ‘Result available’ status.
Video fileVideo: Process to add tests on Ni-kshay
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Add comorbidity
ContentVideo fileVideo: Add Comorbidity in Ni-kshay - Web
Video fileVideo: Add Comorbidity in Ni-kshay - Mobile App
Unified Patient Page
ContentVideo fileVideo: Unified Patient Page
Task List on Ni-kshay
ContentVideo fileVideo:
Task List (Web)
Video fileVideo: Task List on Ni-kshay - Mobile
-
-
CHO-M2: TB Diagnosis and Case finding
Fullscreen-
CHO-CH5: Diagnostic Technologies
FullscreenTesting for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
Cartridge Based Nucleic Acid Amplification Test [CBNAAT]
ContentCartridge Based Nucleic Acid Amplification Test (CBNAAT) is a rapid molecular diagnostic test. It is used for diagnosis of Tuberculosis (TB) and Rif-resistant Tuberculosis (RR-TB) in NTEP. Results are obtained from unprocessed sputum samples in about 2hours which helps in early detection and treatment of TB patients.
India has vast number of CBNAAT laboratories which are utilized for TB/RR-TB detection and Universal Drug Susceptibility Testing (UDST) under the National TB Elimination Program (NTEP).

Figure: CBNAAT Cartridge and Machine in Use (Image courtesy: USAID supported Challenge TB Project)
The CB-NAAT system detects DNA sequences specific for Mycobacterium tuberculosis complex and rifampicin resistance by Polymerase Chain Reaction (PCR). It concentrates Mycobacterium tuberculosis bacilli from sputum samples, isolates genomic material from the captured bacteria by sonication and subsequently amplifies the genomic DNA by PCR. The process identifies clinically relevant rifampicin resistance-inducing mutations in the RNA polymerase beta (rpoB) gene in the Mycobacterium tuberculosis genome in a real-time format using fluorescent probes called molecular beacons.
Video fileVideo: Cartridge-Based Nucleic Acid Amplification Test [CBNAAT] - GeneXpert Technology
Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- India TB Report 2021, National TB Elimination Program (NTEP), MoHFW, 2021.
Assessment Questions
Question
Answer 1
Answer 2
Answer3
Answer 4
Correct Answer
Correct explanation
Part of pre-test
Part of post-test
Under NTEP, CBNAAT is offered upfront for which of these categories?
PLHIV
Paediatric presumptive TB
Presumptive DR-TB
All of the above
4
Under NTEP, CBNAAT is recommended upfront for People living with HIV, Paediatric Presumptive TB patients, Presumptive DR-TB patients and patients notified from the Private sector.
Yes
Yes
CBNAAT requires the processing of sputum samples before testing
True
False
2
Results are obtained from unprocessed sputum samples in about 2hours from a CBNAAT machine
Yes
Yes
Truenat
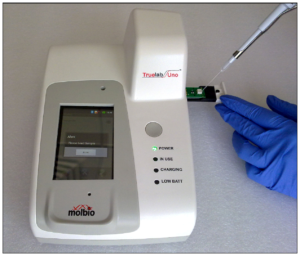
ContentTruenat is an indigenous rapid molecular test platform that is currently under use in NTEP for diagnosis of TB and Rif Resistance. It is a platform utilising real-time Polymerase Chain Reaction (PCR) technology built into micro-PCR chips.
Testing on Truenat involves three components:
- Workstation (consisting of 2 devices)
- Trueprep AUTO Universal Cartridge-based Sample Prep Device for the automated extraction and purification of DNA
- Truelab Real-time micro PCR Analyzer for performing real-time PCR. It is available as 1 (Uno), 2 (Duo) or 4 (Quattro) chip ports.
- Cartridge and Chip
- Reagent kits (Sample Pre-treatment and Prep kits)

Figure: Truenat Source: MolBio Products.
Test results for MTB detection and Rif Resistance has a turn around time of 1-2 hours. Depending on the micro-PCR chips used various tests can be performed using Truenat. Truenat MTB micro-PCR chips detect Mycobacterium tuberculosis bacteria for TB diagnosis. Truenat MTB RIF micro-PCR chip is used as a reflex test to detect resistance to Rifampicin (RIF), the first-line drug for TB treatment
Truenat has many advantages. Truenat is designed to be mobile and is battery operated (~8 hours on full charge). It can be deployed in peripheral laboratories and microscopy centres with minimal or no added facilities and hence it is more point-of-care. Biosafety requirements are similar to smear microscopy. However, it is multi staged and partially automated, requiring the presence of a Lab Technician through out the test.
Resources
- Truenat MTB Kit Insert.
- Trueprep AUTO Universal Cartridge-based Sample Prep Device.
- Practical Guide to Implementation of Truenat Tests for the Detection of TB and Rifampicin-resistance, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Truenat is used in NTEP for: MTB detection Rif Resistance Detection INH resistance Detection MTB and Rif Resistance Detection 4 Truenat is used for MTB and Rif Resistance detection in NTEP Yes Yes The Truelab Analyzer is available in how many chip ports?
2 (Duo)
1 (Uno), 2 (Duo) and 4 (Quattro)
1 (Uno)
4 (Quattro)
2
The Truelab Analyzer is available as 1 (Uno), 2 (Duo) and 4 (Quattro) chip ports.
Yes Yes - Workstation (consisting of 2 devices)
Line Probe Assay [LPA]
ContentLine Probe Assay (LPA) is a rapid molecular test available at centralised laboratories.
The assay is based on Polymerase Chain Reaction (PCR) that can simultaneously detect Mycobacterium tuberculosis complex as well as drug sensitivity to anti-TB drugs.

Figure 1: The GenoType MTBDRplus Molecular LPA Procedure; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Advantages of LPA
- Rapid molecular test. (Turnaround time: 3-5 days)
- Highly sensitive and specific.
- Performed directly from sputum smear-positive specimens and on isolates of M. tuberculosis complex grown from smear-negative and smear-positive specimens.
- Detects multiple gene mutations in anti-TB drugs.
- First-line LPA detects mutations to rifampicin and isoniazid
- Second-line LPA detects mutations to fluoroquinolones and aminoglycosides.
- Suitable for low and high-throughput labs.
Disadvantages of LPA
- Cannot be used as a point-of-care test.
- Requires appropriate laboratory infrastructure, equipment and biosafety precautions.
- Different rooms (DNA extraction, pre-amplification, amplification, post-amplification/ hybridization) are required to perform different steps (Figure 2).
- Requires trained manpower to perform tests and interpret test results.
- Stringent internal quality control is required to prevent contamination.

Figure 2: Amplification (A) and Post-amplification Laboratory (B) for LPA; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Resources
- Guidelines for PMDT in India, 2021.
- Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test LPA can be used as a point-of-care test. True False 2 LPA cannot be used as a point-of-care test. Yes Yes Solid and Liquid Culture in TB
ContentCulturing TB Bacilli is well known and historic method for detection/ confirmation of Tuberculosis. It is a highly sensitive and specific phenotypic test; it can detect even a few viable bacilli in the sample (Upto 10 Colony Forming Units- CFUs). TB bacilli multiply in the culture and form colonies of TB bacilli which can are easily be identified.
Based on the growth media used Culture is divided in to two types, Solid and Liquid Culture methods. Types Culture:
- Solid Culture on Lowenstein Jensen media : Historic gold standard culture test. Results take usually upto 2 months (60 days).
- Modern Liquid culture systems: (e.g. BACTEC MGIT 960, BacT Alert or Versatrek etc.) Results take usually up to 42 days.
Uses
- Solid culture is the gold standard diagnostic test for TB. But it is not used for the purpose of TB diagnosis due to the long turn around time of 2 months. It is largely used for research purposes where it is used as the baseline test on which the sensitivity and specificity of other tests are calculated.
- Liquid Culture is being used for follow-up monitoring of patients on drug resistant TB treatment to detect treatment failure. Liquid culture is also used for long term follow up patients who have successfully completed treatment to detect recurrence.
- Liquid culture is used as a previous step to grow bacilli and obtain isolates prior to Drug Susceptibility Testing.
- Liquid cultures are also used in TB prevalence surveys for its high sensitivity and specificity
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Culture Drug Susceptibility Testing [CDST]
ContentCulture Drug Susceptibility Testing (CDST) is a growth-based phenotypic method used to check the susceptibility of Mycobacterium tuberculosis strains to various first and second line anti-TB drugs. Mycobacterial resistance to a particular drug is identified if there is growth observed in culture in presence of that drug.

In NTEP CDST is the standard method to detect resistance in samples of patients who have tested positive on followup. While CDST is possible on both Solid and Liquid culture, currently, the NTEP utilizes only liquid culture as a method for DST, due to faster Turn around times.
CDST testing services are available under NTEP in designated, specialized laboratories called CDST Labs both in public and private sector. Currently there are 80 such laboratories (60 certified for First Line and 49 for Second line drugs). Such designated laboratories are subject to regular external quality assessment, often by the National Reference Laboratory at that region.
Quality assured DST to R, H, Z, Mfx, Lfx, Lzd, Am, Km and Cm are available across the country.
Resources
-
CHO-CH6: Dignostic Network and Hierarchy
FullscreenLaboratory Hierarchy and Network
ContentNTEP laboratory network is comprising of National Reference Laboratories (NRLs), state level Intermediate reference laboratories (IRLs), Culture & Drug Susceptibility Testing (C & DST) laboratories and peripheral level laboratories. Peripheral level laboratories consist of designated microscopy centres (DMCs) and NAAT labs.
NTEP has a quality assured laboratory network for bacteriological examination of sputum in a 3-tiered system.
Figure: Laboratory network of NTEP
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
NAAT Labs and their role
ContentThe National Tuberculosis (TB) Elimination Program (NTEP) has a network of Nucleic Acid Amplification Tests (NAAT) laboratories coupled with Designated Microscopy Centers (DMCs) to form the backbone of the diagnostic component of TB services.
Nucleic Acid Amplification Tests (NAAT) laboratories includes Cartridge-based NAAT (CBNAAT) and TrueNat tests. These tests detect tuberculosis as well as rifampicin resistance and are more sensitive than smear microscopy.
Functions of Nucleic Acid Amplification Test (NAAT) Laboratories:
- Acting as a hub for collection of samples from public and private health facilities (spokes)
- Universal Drug Susceptibility Testing (UDST) to rule out rifampicin resistance among confirmed TB patients
- Timely provision of NAAT test result to the TB patient, medical officer of the concerned health facility and NTEP staff for related actions
- Acting as a sample dispatch center for the Culture DST laboratory for subsequent processing of samples for first-line line probe assay (LPA) and second-line drug resistance testing utilizing second line LPA and liquid culture DST
- Recording and reporting including digitization of diagnostic process from collection to test result in NTEP Nikshay portal and Laboratory Information Management System
- Management of supplies and logistic associated with laboratory logistic (CBNAAT cartridges and TrueNAT chips) and reporting any additional requirement thereof
- Supporting the quality assurance activities undertaken by District or Intermediate Reference Laboratory under NTEP
- Support health system in carrying out special drives for vulnerable and at-risk population and their testing directly by CBNAAT (slum population, diabetic population, smoker, malnourished people, patients of silicosis and kidney dialysis etc.)
Resources
- RNTCP Technical and Operational Guidelines for TB Control in India, 2016.
- Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Functions of a Designated Microscopy Centres [DMC]
ContentFunctions and Integrated Services of the DMC
- Testing of Sputum samples by Microscopy.
- Request/ referral for microscopy or Nucleic Acid Amplification Test (NAAT) or Culture and Drug Susceptibility Test (C&DST) or Chest X-ray (CXR) or Tuberculin Skin Test (TST) is generated at the PHI-DMC, as well as follow-up tests.
- Maintain consumables and logistics required for testing/ packaging and transport.
- Maintain TB laboratory registers for recording and reporting.
- Notify every TB patient in Nikshay at the earliest and update information of patients on comorbidity, treatment adherence, treatment outcome, contact investigation and TB Preventive Treatment (TPT).
- Biomedical waste management for the waste generated at DMCs.
- A DMC is required to participate in the External Quality Assurance system(EQA) of NTEP to ensure standardized quality diagnostic testing.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Sputum Collection centres
ContentTo increase access to diagnostic services, NTEP has a provision for sputum collection centres in areas where the health facility is not equipped with key requirements to conduct sputum microscopy, molecular tests, drug susceptibility testing or follow up examinations.
Sputum collection centres are dedicated locations where sputum samples are collected, packaged and then transported to nearby TB diagnostic centres. It could be attached to any near-by health-facility as well.
Requirements of a Sputum Collection Centre
To function as sputum collection centres, the following is essential:
- Linkage/ mapping (time and distance) to testing laboratory
- Availability of adequate number of sputum cups and falcon tubes, logistics for sample packaging and transport
- Identification of open areas for sputum collection
- Staff trained in NTEP guidelines on sputum collection, sample packaging and transport, complete and correct documentation of laboratory request form, and infection control practices
- Feasibility and financial measures required for sample transport
- Inclusion of local volunteers, courier services, sample transportation under National Health Mission Free Diagnostic Services or other mechanisms as decided by the state/district
- Availability of Information, Education and Communication (IEC) material, training modules, and job-aids
Sputum collection centres are established in:
- Ayushman Bharat Health and Wellness Centres/Sub-centres
- Urban primary health centres
- Tribal, hilly, desert and difficult-to-reach areas of the country
Resources
- Training Modules for Programme Managers and Medical Officers
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres
- Mycobacteriology Laboratory Manual, GLI Initiative, 2014
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under NTEP, where are sputum collection centres established to increase access to diagnostic services? Tribal areas Ayushman Bharat health and wellness centres Difficult-to-reach areas All of the above 4 To increase access to diagnostic services, sputum collection centres are established in Ayushman Bharat health and wellness centres, Urban health centres, tribal, hilly, desert and difficult-to-reach areas of the country. Yes Yes
-
CHO-CH7: Approaches to TB Case Finding
FullscreenApproaches to TB Case Finding
ContentPeople who have been exposed to patients with infectious TB are known as TB contacts; they constitute a high-risk group for TB. Case finding investigation contributes to the early detection of TB cases, and results in identifying a significant number of additional patients.
Figure: Approaches to Tuberculosis Case Finding
Active case-finding requires systematic screening and clinical evaluation of populations who are at high risk of developing TB, such as people living in slums, tribal areas, congregate settings, persons who are household contacts of TB cases
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Active Case Finding
ContentSystematic screening of all individuals of a defined population is known as active case finding. It is applied outside of health facilities at the community level by the health system.
Objective of ACF is to:
- identify cases early, initiate prompt treatment, reduce risk of poor treatment outcomes and reduce risk of further transmission of TB
- to provide access to diagnosis services to populations that would have been otherwise unreached
It is effort intensive and is recommended only in population groups where there is estimated high case load. In NTEP, ACF is recommended only to be performed in Key / vulnerable population.
ACF can also be clubbed with suitable ACSM campaigns to create awareness about the signs and symptoms and about TB in the target population/ community. It can also be combined with other health activities/ campaigns (such as Pulse Polio/ Leprosy screening/ population based screening for NCDs) for increased efficiency.
Resources
- Training Modules for Programme Managers and Medical Officers.
- Active TB Case Finding, Guidance Document.
- WHO recommendations for Systematic Screening for Active Tuberculosis
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is not a primary objective of ACF? Increase TB notification Early identification of cases. Reduce the risk of transmission of TB. Reduce the risk of poor treatment outcomes. 1 Notification is not a primary objective of ACF. Yes Yes Passive Case Finding
ContentPassive case finding is essentially where the patient self reports to the health care provider with symptoms. This requires that affected individuals are aware of their symptoms, have access to health facilities, and are evaluated by health workers or volunteers who recognise the symptoms of TB and link those individuals for TB testing services.
This approach to case finding has the least effort and cost and is a minimum expectation. In a Peripheral Health Institution (PHI), it is estimated that about 2-3% of new adult outpatients are symptomatic that require referral for TB diagnosis (presumptive TB cases).
Passive case finding may miss TB patients if :
- The disease is mild/ transient.
- Access to healthcare is poor.
- Health providers do not have an adequate index of suspicion and are unable to reliably link respiratory symptoms to TB.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following can be considered a passive case finding? TB case finding for all patients attending an HIV clinic. TB case finding in all inmates of an elderly home. Patients attending a PHC with symptoms are referred for testing by the doctor. TB case finding among household contacts of a TB case. 3 All other examples except those attending PHC referred for TB testing are cases of active or intensified case finding effort. Yes Yes What may cause a passive case finding to miss cases? Healthcare providers fail to notify the case. Healthcare providers do not refer cases for TB testing. There are no health facilities in the area. Both 2 and 3 4 Healthcare providers failing to notify cases is missing notification and not related to passive case finding. Yes Yes Intensified Case Finding
ContentIntensified Case Finding (ICF) is a case finding approach between Active and Passive approaches. Here individuals coming in contact with the health system through any activity are screened actively for symptoms of TB and referred for testing.
This approach brings the benefit of active case finding approach by active screening for TB symptoms, but does limit the extensive effort required by restricting to only those people who has some or the other healthcare problem. This approach is considered for people attending a healthcare facility.
Some examples of ICF are screening for TB symptoms and referral for testing in:
- all cases attending an HIV clinic.
- among children with malnourishment who attend a nutrition clinic.
- all mothers attending the antenatal clinics
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is an example of an intensified case finding?
Systematic screening for TB of all contacts of TB cases. Screening all cases attending an OPD with respiratory symptoms for TB testing. Referring cases that report more than 2 weeks of cough from an OPD for TB testing. Screening all people belonging to a slum for TB symptoms. 2 Systematic screening of TB contacts and those belonging to a slum population are examples of active case finding.
Referring to cases that report TB symptoms is a passive case finding.
Yes Yes Bidirectional Screening
ContentBidirectional screening is a method to identify cases in diseases which have predisposition to each other or has a significant influence on each other. For example TB and HIV, where having HIV increases risk of developing TB and cases with TB would have poor outcomes if co-infected with HIV.
Screening for TB is done through four-symptoms complex based screening or through Chest X-ray. Screening for the linked disease is carried out as per the policies of the corresponding health program.
Bi-directional screening policies are implemented by various disease control programs. For example, with NTEP the following disease control efforts implement a bidirectional screening policy:
- HIV through NACO
- COVID19
- Diabetes Mellitus (DM) through NPCDCS
- Tobacco through National Tobacco Control Program
Both programs monitor bidirectional screening, referral and testing as per their own policies.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Bidirectional screening for TB is not done in which of the following conditions? Diabetes Tobacco abuse/ addiction Pregnancy COVID-19 3 Although pregnant mothers may be screened for TB as a part of intensified case finding, all TB cases are not actively/ routinely screened for pregnancy. Yes Yes
-
CHO-CH8: TB Case Finding in NTEP
FullscreenClassification of TB cases based on history of Previous TB treatment
Content- New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
- Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated(cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
- Transferred In: A TB patient who is received for treatment in a Tuberculosis Unit, after registered for treatment in another TB unit is considered as a case of transfer in.
- Transferred Out : A patient who has been transferred to another recording and reporting unit and whose treatment outcome is unknown.
Classification of TB on the basis of Drug Resistance
ContentResistant Sensitive Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistant to Isoniazid (H) Rifampicin (R) Fluroquinolones (FQ) =
Ofloxacin, Levofloxacin,
MoxifloxacinGroup A Drugs =
Bedaquiline/ LinezolidH Mono / Poly Drug Resistance Resistant Sensitive Unknown/ Sensitive Unknown/ Sensitive Rifampicin Resistance (RR) Unknown/ Sensitive Resistant Unknown/ Sensitive Unknown/ Sensitive Multi Drug Resistance TB (MDR TB Resistant Resistant Unknown/ Sensitive Unknown/ Sensitive Pre-Extensive Drug Resistance (Pre -XDR) Resistant Resistant Resistant Unknown/ Sensitive Extensive Drug Resistance (XDR) Resistant
Resistant Resistant Resistant Resources:
Classification of TB on the basis of diagnosis
ContentOn the basis of diagnosis, Tuberculosis (TB) can be classified into 2 main types:
- Microbiologically confirmed TB
- Clinically diagnosed TB
Microbiologically Confirmed TB
- Microbiologically confirmed TB refers to a presumptive TB case from which a biological specimen is positive for acid-fast bacilli/ Mycobacterium tuberculosis on smear microscopy, culture, or on a rapid diagnostic molecular test (such as Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ Truenat).
- All such diagnosed cases should be notified at the source, regardless of whether TB treatment has started.
Clinically Diagnosed TB
- Clinically diagnosed TB refers to a presumptive TB case that is not microbiologically confirmed but has been diagnosed with active TB by a clinician who has decided to give the patient a full course of anti-TB treatment.
- This definition includes cases diagnosed on the basis of X-ray abnormalities or suggestive histology or extrapulmonary cases without laboratory confirmation.
- Clinically diagnosed cases subsequently found to be microbiologically positive (before or after starting treatment) should be reclassified as microbiologically confirmed.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Definitions and Reporting Framework for Tuberculosis, WHO, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TB is classified on the basis of diagnosis into which of the following? Microbiologically confirmed TB and clinically diagnosed TB Mono-resistant TB and poly-resistant TB Recurrent cases and previously treated cases None of the above 1 TB can be classified on the basis of diagnosis into 2 main types: Microbiologically confirmed TB and Clinically diagnosed TB.
-
CHO-CH9: Active Case Finding Campaign
FullscreenACF campaign activities
ContentActive Case Finding (ACF) is a provider-initiated activity with the primary objective of detecting TB cases early by active case finding in targeted groups and to initiate treatment promptly.
- It can target people who anyway would have sought health care with or without symptoms or signs of TB and also people who do not seek care.
- Increased coverage can be achieved by focusing on clinically, socially and occupationally vulnerable populations.
- ACF activities in a campaign mode will create mass awareness about the signs and symptoms in general population
Objective of ACF campaign activities- Reaching the unreached in a campaign mode to enhance TB case finding

Figure 1: Objectives of active case finding
Beyond TB disease, screening can also identify individuals who are eligible for and would benefit from TB preventive treatment (TPT) once TB disease is ruled out, thus further averting future incident TB.
General process is as below:

Figure 2: ACF campaign general process
Resources
- WHO consolidated guidelines on tuberculosis: Module 2: Screening, Systematic screening for TB disease;WHO 2021
- India TB Report 2022, Central TB Division, MoHFW 2022
- Active TB Case Finding- Guidance document, Central TB Division & DGHS, MoHFW 2017
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF will help in reducing spread of tuberculosis True False 1 ACF helps in early case detection & treatment initiation, thus reducing community level prevalence of TB disease & limit spread
Mapping the population for ACF
ContentMapping of vulnerable population is a pre-requisite for conducting an efficient ACF campaign. It involves understanding the population characteristics, identifying and enumerating and mapping the target population.
Guidelines for mapping
- Identify & map high risk/ vulnerable populations in the local area with the following guidance. If additional information is available locally, it can be used for the prioritisation of target groups.
Priority Urban area Rural area Tribal area
1 Slum Difficult to reach villages Difficult to reach villages & hamlets 2 Prisons inmates Mineworkers Villages with a known higher caseload 3 Old Age homes Stone crusher workers Tribal school hostels 4 Construction site workers Populations groups with known high malnutrition Areas with known high malnutrition 5 Refugee camps Populations known to drink raw milk Villages seeking care from traditional healers 6 Night shelters Populations known to eat uncooked meat Populations known to drink raw milk 7 NACO/SACS identified HRG for HIV NACO/ SACS identified HRG for HIV Populations known to eat uncooked meat 8 Homeless Weaving & Glass industrial workers Tribal areas with little ventilated huts 9 Street children Cotton mill workers 10 Orphanages Unorganised labour 11 Homes for destitute Tea garden workers 12 Asylums Villages largely seeking care from traditional healers 
Figure 1: Schematic map for house to house survey of identified vulnerable population
- Without proper mapping, there is a high chance of missing cases. The success of the active TB case finding campaign relies on how good the mapping is.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF campaign activities are done in all individuals of a defined area. True False 2 Symptom screening as part of the ACF campaign will be done in the identified and mapped target groups only (not in the general population).
Yes Yes Microplanning and execution of ACF campaign
ContentMicroplanning for ACF Campaign
A microplan is a detailed plan of action in terms of human resources, materials, money and time. A good microplan ensures that the health intervention reaches each individual beneficiary and is crucial to the success of the activity. For Active Case Finding (ACF), microplanning is performed at the health facility level and collated at the block, district and state levels. Training for the same is given to concerned personnel during state, district and block level meetings prior to the campaign. Microplan at PHI, Block, District and State levels should be ready at least 15 days prior to the initiation of field activities.
Microplanning is done with respect to:
I. Advocacy, Communication and Social Mobilization (ACSM)
A comprehensive IEC plan should be made with communication material for mass media, mid-media and print media to reach out up to the remotest village in advance.
II. Logistics
- Microplan should include planning additional consumables required for the campaign
- It includes additional slides, laboratory reagents, sputum cups, falcon tubes, sample transport boxes, X-ray films, Cartridge-based Nucleic Acid Amplification Test (CBNAAT) cartridges, etc. Additional sputum containers (minimum 1000 per lakh population) will be procured and supplied to health staff for collecting sputum sample from the eligible symptomatic two weeks before the start of field activities
- Linkages of Peripheral Health Institute (PHI) areas with Designated Microscopy Centre (DMC), X-ray facilities, CBNAAT lab, Extra Pulmonary (EP) sample collection and EP testing should be included in the planning up-front.
- Laboratory technicians of the linked DMC and CBNAAT labs should be well informed about the increase in workload and recording of information during ACF activities.
III. Field activities including human resources
- Maps prepared for other campaigns like Pulse Polio, Leprosy Case Detection Campaign (LCDC), etc. must be used while planning. If maps are not available with local bodies, search team members and supervisors should be sent to the area before the ACF campaign, in order to become familiar with the area and develop maps.
- The number of houses to be covered each day should be mentioned in the microplan. This number may vary from day to day depending upon the geographical situation of the area planned to be covered by the team on a particular day.
- Teams of two persons each should go house-to-house. Out of the two members in each team, one should be a local volunteer (including Accredited Social Health Activist (ASHA)).
- Each team should be allocated clear-cut, well-demarcated areas clearly mentioning the starting and ending points, identifiable with landmarks; for each day of House to House (h-t-h) activity.
- In special areas, one additional person from the local community, where the team will be working, should accompany the team.
- Human resources required for covering the mapped vulnerable population during field activities should be calculated and recorded.
- For planning and implementation purposes, urban areas should be divided into smaller planning units based on municipal wards or assemblies, or by roads or prominent landmarks. Each such unit should be put under the charge of a medical officer or nodal officer.
- Involvement of the local community, leaders, health officials, municipal bodies and their staff is essential in planning.
- Local staff is familiar with the layout of the urban areas and their inputs are vital for planning and supervision of house-to-house activities.
Execution of Microplan
The ACF campaign is executed as per the microplan and supervision is done with reference to the microplan
The House to House (h-t-h) survey is done for 2 weeks
A survey team consisting of 2 persons - one NTEP staff/ partner organization staff/ General Health services staff and one local volunteer / ASHA worker. They go from house to house in the mapped vulnerable areas/ key population groups and screen individuals for symptoms of TB. After screening, the eligible population for sputum examination includes: Persistent cough for ≥2 weeks, Fever for ≥2 weeks, Significant weight loss (>5% weight loss over last 3 months), Presence of blood in sputum any time during the last 6 months, Chest pain in the last one month, History of Anti-TB Treatment (previous/ current). If any one of these is present, a sputum cup or falcon tube is given to them and a sputum sample is collected. Sputum samples thus collected are transported to a designated lab using the sample transport system existing in the area. testing using smear microscopy/CBNAAT will be done for all symptomatic persons as per the state policy. Those who are microbiologically confirmed to be positive should be initiated on treatment within 2 days. Additionally, the team will look for other symptoms/diseases also. If person is having any symptoms or other ill health, s/he will be referred for evaluation by a Medical Officer for further management, if needed. Field Activity Report will be submitted by each health staff on a daily basis to the Medical Officer of the Peripheral Health Institution
Resources
- Active TB Case Finding – Guidance Document, 2017, Central TB Division, MoHWF, New Delhi.
- Active Case Finding for Tuberculosis in India: A Syntheses of Activities and Outcomes Reported by the National Tuberculosis Elimination Programme, Burugina Nagaraja S et al, Trop Med Infect Dis., 2021.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is wrong about microplanning in ACF?
Microplan is first made at the state level. It is a detailed plan of the human resources, logistics and field activities required in the ACF campaign.
A good microplan is important for the success of the ACF campaign.
Supervision of field activities is done with reference to the microplan.
1
Microplan is made at the health facility level and then collated at subsequent levels.
Yes
Yes
Recording formats under ACF campaign
ContentVulnerability mapping and Microplanning are 2 important activities of Active Case Finding which precede field activities. Vulnerable populations should be mapped and recorded in prescribed formats from health facility level onwards. Mapping data from PHI are consolidated at Block level, those at Block level are consolidated at district level and those at district level are consolidated at state level. Data from mapping formats is used for microplanning. Microplanning forms the basis of field activities. Microplans are also consolidated at subsequent levels. During supervision and monitoring, it is important to assess the activities with respect to the microplan.
The recording formats for ACF include:
1. Formats for mapping - Health Facility Level, Block Level, District Level and State Level
2. Formats for microplanning - Manpower, Logistics, Field Activity
FORMATS FOR MAPPING





Mapping details should also be entered in Ni-kshay under the section shown below:
Image
Fig: Ni-kshay section for reporting various ACF activities
FORMATS FOR MICROPLANNING
Based on the requirement obtained from the mapping exercise, microplanning is done with respect to human resource, logistics and field activities
Human Resource Planning Form



Field activities are captured in Form 1 & 2 of the ACF. The data from field activities are compiled at the PHI level and submitted to the District and State using google sheets at present. Although there is no specific mechanism to demarcate the presumptive TB patients and the confirmed (clinical and microbiological) TB cases in Ni-kshay, States follow different mechanism including marking in the Laboratory register as ACF testing and sending a separate sheet to the district in paper format.
Reference:
1. Active TB Case Finding - Guidance Document, Central TB Division & DGHS, MoHFW, 2017
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Vulnerability mapping and microplans for ACF should be recorded at
Health facility level
District level
State level
All the above
4
Mapping activities should be recorded at health facility level and consolidated at subsequent levels (district, state, etc)
Yes
Yes
-
-
CHO-M3: TB Treatment and care
Fullscreen-
CHO-CH10: General concepts in TB Treatment
FullscreenGoals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentThe Medical Officer (MO) of the referring health facility initiates TB treatment on receipt of the diagnostic test results. All efforts are made to initiate the treatment at the earliest.
The treatment regimen is decided based on the type of patient and TB (based on drug sensitivity pattern, i.e., drug-sensitive TB or H-mono/ poly resistance, history of adverse drug reaction to anti-TB drugs).
The patient needs constant support of a health volunteer or peer, who can monitor the treatment, help him in getting a follow-up, keep him motivated, counsel the family/ contacts, etc. These health volunteers/ peers are called treatment supporters in NTEP.
The steps in treatment initiation include:
- The MO performs a clinical evaluation of the patient and assesses for comorbidities.
- Counselling of TB patients and their families should be done.
- Peripheral health worker/ treatment supporters responsible for monitoring treatment adherence and treatment providers acceptable to the patient should be assigned.
- A treatment card should be opened for each patient.
- Each patient should be given a TB Identity Card.
- Drugs should be made available at the treatment centre.
- Public health action for all notified TB patients should be initiated.
All the process related to patient treatment initiation should be documented in Nikshay.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What key activities are included during TB treatment initiation?
Clinical evaluation
Counselling
Treatment card and TB ID card opened, Nikshay updated with treatment details
All the above
4
During TB treatment initiation the key activities include clinical evaluation of the patient; counselling of patient and family members; opening of treatment card and TB ID card and updating of treatment details on Nikshay.
Yes
Yes
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Closing Cases and Assigning Treatment Outcomes
ContentVideo fileVideo:
Closing Cases and Assigning Treatment Outcomes (Web)
Video fileVideo:
Closing Cases and Assigning Treatment Outcomes (Mobile)
Adverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
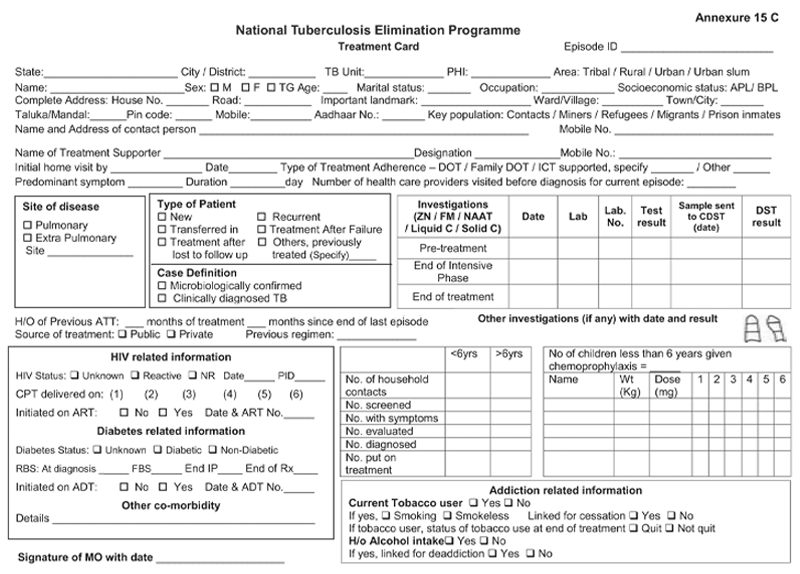
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
Follow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
-
CHO-CH11: DS-TB Treatment and care
FullscreenDrug-sensitive Tuberculosis
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Categorization of TB Treatment Regimen
ContentDaily Regimen is prescribed for TB patients, where patients need to consume the medicine daily.
Daily Regimen comprises of the first line Anti TB drugs, based on
- Age: Adult/Paediatric
- Weight of the patient: Weight Bands
Age: Based on the age, patients are categorized into
- Adults: Patient's age should be 19 years or more.
- Paediatrics: Patient's age up to 18 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosage is based on the TB patient’s weight.
- A weight band category is defined for Adult and Paediatric patients separately and medicines are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
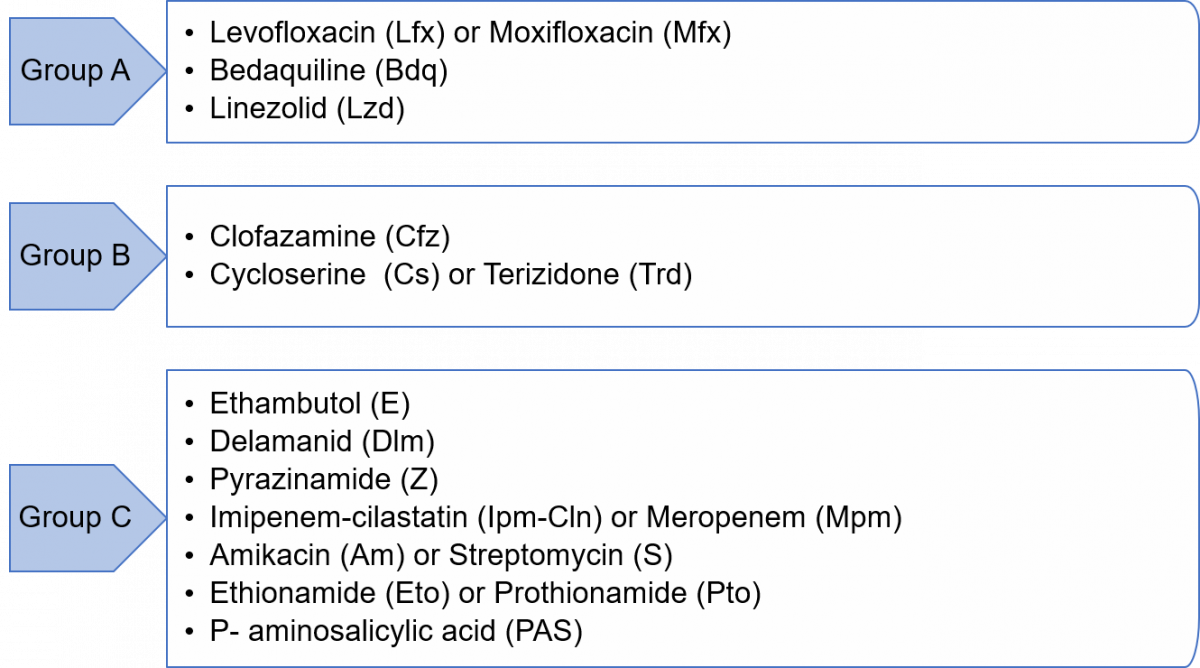
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
-
CHO-CH12: TB Infection treatment and care
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
TB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes Counselling for TPT
ContentCounselling is of paramount importance for TB Preventive Treatment (TPT) initiation and completion as most of the target population screened and found eligible would know that they do not have TB disease, would be symptom-free or otherwise healthy and would not feel the need to take any treatment, especially Household Contacts (HHC).
Stakeholders Involved in Counselling for TPT (Figure below)

Figure: Stakeholders involved in counselling for TPT
Abbr: HWCs: Health and Wellness Centres; PHC: Primary Health Centre; ICTC: Integrated Counselling and Testing Centres; ART: Anti-retroviral Therapy; PLHIV: People Living with HIV
Components of Counselling for TPT
While counselling the person and family members, the treating doctors/ staff must follow the steps outlined in the table below for an effective counselling session.
Component
Actions to be taken
Confidentiality
Ensure confidentiality when seeking a person’s commitment to complete the course before initiating TPT.
Information
Provide information on:
- TB infection
- Need for TPT and protective benefits to the individual, household and wider community
- TPT is available free of charge under National Tuberculosis Elimination Programme (NTEP)
- TPT regimen prescribed, including duration, schedule of medication collection, and directions on how to take the medications
- Potential side-effects and adverse events involved and what to do in the event of various side-effects. People treated with rifamycins should be alerted in advance about the pink discolouration of secretions due to this medicine
- Importance of completing the full course of TPT
- Reasons and schedule of regular clinical and laboratory follow-up for treatment and monitoring
- Signs and symptoms of TB and advise on steps if they develop them
Medication adherence support
Agree on the best way to support treatment adherence, including the most suitable location for drug intake and the need for a treatment supporter, if required.
Family support
Involve family members and caregivers in health education when possible.
Openness
Invite clarification questions and provide clear and simple answers.
Information, Education and Communication materials
- Provide information materials in the local language and at the appropriate literacy level of the person concerned.
- Reinforce supportive educational messages at each contact during treatment.
Call support (in case of emergencies)
Provide a telephone number of the HCW staff/ TB Health Visitors and Senior Treatment Supervisors concerned to call for other queries or a need to contact health services for advice.
The National TB Elimination Programme (NTEP) national call centre (NIKSHAY SAMPARK – Toll-free number 1800116666) may be provided to index TB patients, those initiated on TPT and family members to serve as a resource for information, counselling and troubleshooting as required to enable TPT initiation, follow-up monitoring and completion.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following people are involved when counselling for TPT?
Index TB patients
Caregivers
Family members
All of the above
4
When counselling persons eligible for TPT, it is best to involve the index TB patients, their families and caregivers.
Yes Yes Monitoring adherence to TPT
ContentTo achieve high treatment completion rates and the desired epidemiological impact of the TB Preventive Treatment (TPT), monitoring TPT treatment adherence, including management of missed doses and Adverse Drug Reactions (ADRs), is of paramount importance under the National TB Elimination Programme (NTEP).
Significance of Monitoring Adherence to TPT
Adherence to the TPT course and treatment completion are important determinants of clinical benefit, both at the individual and population levels as:
- Irregular or inadequate treatment reduces the protective efficacy of the TPT regimen.
- Poor adherence or early cessation of TPT can potentially increase the risk of the individual developing TB, including drug-resistant TB.
- Efficacy of TPT is greatest if at least 80% of the doses are taken within the duration of the regimen. The total number of doses taken is also a key determinant of the extent of TB prevention.

Figure: Strategies to Promote Adherence
Prevent TB India App and Integration with Nikshay as a Monitoring Tool
- Currently, under the NTEP, the person’s lifecycle approach and TB treatment episode level are recorded in Nikshay.
- TPT information management is integrated with this existing Nikshay approach. This includes information on screening, testing, eligibility assessment, TPT initiation, adherence monitoring and follow-up till treatment completion.
- The NTEP has adapted the World Health Organisation (WHO) Prevent TB India app and hosted it on Nikshay as an interim solution till the Nikshay TPT module is developed and fully functional.
- Health workers or treatment supporters will make entries directly into the app.
- The TPT monitoring dashboard can be accessed by various levels of supervisors using their respective Nikshay login ids using a link provided in the Nikshay Reports section on TPT Reports.
- A web-based comprehensive dashboard for Prevent TB initiative is also available at https://ltbi.nikshay.in/ltbi-generic-new/#/
Table: Roles of Stakeholders in Monitoring Adherence to TPT Role
Stakeholder
Treatment support and adherence monitoring including entry of daily doses taken in the Prevent TB India app/ Nikshay TPT module.
Community volunteers (TB survivors/ champions, Accredited Social Health Activists (ASHAs) and Anganwadi Workers)
- Regularly undertake home visits or tele/ video calls to monitor TPT adherence.
- Identify treatment interruptions at the earliest (Dashboards of Prevent TB India app/ Nikshay TPT module may be checked every week along with pill counting).
- HWCs/ sub-centre/ urban health posts (Community Health Officers (CHOs), Auxillary Nurse Midwives (ANMs), multipurpose workers and other field staff)
- Primary Health Centres (PHCs)/ Urban PHCs/ Private clinic (Medical Officers (MO), staff nurse)
- Adherence support and clinical monitoring through the concerned PHC/ sub-centre.
- Supportive supervision and handholding support to field level facilities and frontline workers, ASHAs and community volunteers on digital recording, using Prevent TB India app and monitoring TPT and follow-up examinations.
TB Unit (MO, Laboratory Technicians (LTs), staff nurse, pharmacist, counsellor (if available), Senior Treatment Supervisors (STS), Senior TB Laboroary Supervisors (STLS), TB Health Visitors (TBHV))
Ensuring adherence support for People Living with HIV (PLHIV) on TPT through mechanisms such as outreach workers, PLHIV networks, peer support groups, etc.
Anti Retroviral Therapy (ART) centre/ Link ART centre (MO, pharmacist, (institutional) staff nurse, counsellor, care coordinator)
Monitor and support adherence to TPT.
Tertiary care/ Medical colleges/ Corporate hospitals/ District hospitals/ Dialysis/ Cancer facilities (doctors, staff nurses)
Review data updating in Prevent TB India app/ Nikshay TPT module wherever available, check the quality of data regularly and provide feedback to TPT treatment supporters and for retrieval of TPT interrupters.
Supervisory staff at all health facilities including the State/ District TB cell (State TB Officers (STO), District TB Officers (DTO), State/ District Programme Coordinators)
Resources:
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment.
- Prevent TB Dashboard.
- Prevent TB India Mobile App.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which tools are used to monitor TPT adherence under the NTEP?
Video calls
Counting empty blisters
Directly asking the patient
Options 1 and 2
4
TPT adherence monitoring tools include direct observation of drug intake, 99DOTS/ MERM, counting empty blisters, tele/ video calls and refill monitoring.
Which of the following apps are currently used by NTEP to monitor TPT adherence?
TB Aarogya Sathi
Prevent TB India App
TPT app for NTEP
None of the above
2
NTEP has adapted the WHO Prevent TB India app and hosted it on Nikshay to monitor the entire TPT care cascade, including TPT adherence.
-
CHO-CH13: TB-Comorbidities and special situations
FullscreenComorbidity & special situation with TB
ContentSeveral medical conditions are risk factors for TB and poor TB treatment outcomes. Similarly, TB can complicate the course of some diseases. Therefore, it is important to identify these comorbidities in people diagnosed with TB to ensure early diagnosis and improved outcomes. When these conditions are highly prevalent in the general population, they can significantly contribute to the TB burden. Consequently, reducing the prevalence of these conditions can help prevent TB.
TB shares underlying social determinants with many of these conditions. Addressing the social determinants of health is a shared responsibility across disease programmes and other stakeholders within and beyond the health sector.
Figure: Various comorbid and special situation related with tuberculosis
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Silicosis in TB Patients
ContentSilicosis is a progressive and disabling interstitial lung disease caused by inhalation and deposition in the lungs of particles of free silica.
Mutual Risk of TB and Silicosis
- TB is a clinical complication of silicosis, called silico-tuberculosis. Silica-exposed workers with or without silicosis are at increased risk for TB. There is also an increased risk of extrapulmonary TB in individuals exposed to silica.
- The risk of a patient with silicosis developing TB is 2.8 – 3.9 times higher than a healthy individual.
- The risk of TB relapse in patients with silicosis is approximately 1.5 times higher than in patients without silicosis.
The presence of silica particles in the lung and silicosis may:
- Facilitate initiation of TB infection and progression to active TB
- Exacerbate the course and outcome of TB, including prognosis and survival
Diagnosis
The diagnosis of silicosis is made based on a history of exposure to silica accompanied by a clinical and radiological profile consistent with the disease.
Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), patients with silicosis are first screened according to the four-symptom complex to rule out/in active TB and tested for TB accordingly.
If active TB is ruled out >> Refer for Tuberculin Skin Test (TST)/ Interferon Gamma Release Assay (IGRA) >> Positive test >> Evaluate with Chest X-ray (CXR) >> Commence TB Preventive Therapy (TPT) irrespective of CXR results.
CXR often indicates TB in silicosis patients earlier than the clinical symptoms, and regular radiographic screening is required for early TB detection. Radiographic comparison of serial films is done with particular attention to:
- Rapid appearance of new opacities, symmetric nodules or consolidation and the finding of pleural effusion or excavations.
- Cavitation is the strongest indicator of probable silico-tuberculosis.
Other diagnostic tools that can help in diagnosis are:
- Chest Computed Tomography (CT) scan
- Bronchoscopy with bronchoalveolar lavage in conjunction with transbronchial biopsy
- Spirometry
Treatment and Follow-up
To keep the disease from getting worse, all silicosis patients need to eliminate any more exposure to silica. Supportive measures include the use of cough medicines, bronchodilators, oxygen therapy and pulmonary rehabilitation.
TB treatment in patients with silicosis is challenging, perhaps due to impairment of macrophage function by free silica and/or poor drug penetration into fibrotic nodules. Usual anti-TB drugs with directly observed therapy are recommended but for an extended duration of at least 8 months, to reduce the chances of relapse.
Follow-up of patients with silicosis and TB follow the same schedule as is in prevailing guidelines.
Prevention
TB prevention in silicosis patients is essential and includes:
- Active surveillance of vulnerable groups including workers
- Adoption of measures to reduce exposure to silica dust
- Patients with silicosis are eligible for TPT after ruling out active TB
NTEP is in the process of engaging with the Ministry of Labour and Mining to identify high priority districts with stone crushing units/ mining industry. Specific guidelines will be developed to support persons with an occupational risk for TB and provide access, diagnosis and treatment services from the programme.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Silico-tuberculosis, Silicosis and Other Respiratory Morbidities Among Sandstone Mine-workers in Rajasthan - A Cross-sectional Study, Saranya Rajavel et al., 2020.
- Mini-review: Silico-tuberculosis; Massimiliano Lanzafame et al, 2021.
- Immunity to the Dual Threat of Silica Exposure and Mycobacterium tuberculosis, Petr Konečný et al., 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about silicosis and TB is/are incorrect?
TB is a clinical complication of silicosis, called silico-tuberculosis.
Silica-exposed workers with or without silicosis are at increased risk for TB and EPTB.
TB in patients with silicosis is easily diagnosed clinically as the patient coughs up silica particles.
TB treatment in patients with silicosis is often of extended duration to prevent relapse.
3
Clinical diagnosis of active TB superimposed on silicosis is often difficult, particularly in the initial phases, when clinical manifestations may not be indicative and radiological alterations can be indistinguishable from those due to the pre-existing silicosis.
Yes Yes Cancer in TB patients
ContentRelationship between Cancer and Tuberculosis (TB)
TB and malignancy may be related in the following four ways:
- TB as a marker for occult cancer: Occult cancer may lead to locally-reduced infection barriers and/or generalised immunosuppression, rendering a cancer patient susceptible to TB infection/ reactivation.
- TB as a risk factor for cancer: TB may increase the risk of cancer locally and systemically through chronic inflammation, fibrosis and production of carcinogenic molecules.
- Shared risk factors for TB and some cancers: Shared risk factors such as smoking, alcoholism, Chronic Obstructive Pulmonary Disease (COPD) and immunosuppression, including HIV, may lead to both TB and cancer, affecting both prevalent and subsequent cancer risk.
- Treatment of cancer-fueling TB: Many cancers are treated with immunosuppressants or steroids. These drugs might induce immunosuppression in the patients undergoing treatment for cancer and hence, a flare-up of TB.
Mutual Risk of Cancer and TB
- TB patients are 2-11 times more likely than non-TB patients to develop lung cancer, according to studies.
- After cancer diagnosis, the incidence of TB also increases, both in the short term and long-term.
- All types of cancer increase the risk of the development of active TB, but with varying degrees. Haematologic cancer patients had the highest rates of active TB, followed by head and neck cancers, lung cancer and breast cancer patients.
There is intrinsic immunosuppression due to the cancer itself, immunosuppressive effects of chemotherapy, or other host factors (e.g., smoking, malnutrition) that may increase the susceptibility to both cancer and TB. Thus, there is increased incidence of TB in cancer patients, and vice-versa.
Diagnosis of TB in Cancer Patients: Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), cancer patients are first screened according to the four-symptom complex to rule out/in active TB and all presumptive TB cases need to undergo testing for TB.
Co-existence of TB and cancer poses a diagnostic challenge since clinical and radiological presentations between TB and cancers are similar, hence the need for bidirectional screening. E.g., if biopsy specimens reveal infiltration by malignant cells, still send sample for microbiological confirmation of M. tuberculosis. Thus, allowing for accurate diagnosis and initiation of anti-TB treatment instead of attributing clinical deterioration to chemotherapy complications and progression of underlying malignancy.
Diagnosis of lung cancer in TB patients is usually done in consultation with a clinical specialist and can include examination of induced sputum specimens for malignant cells, as well as use of other diagnostic tools such as Computed Tomography (CT) scans, bronchoscopy, Positron Emission Tomography (PET) scans, Magnetic Resonance Imaging (MRI), histopathology and the use of biological markers.
Treatment
TB treatment in cancer patients uses the standard DS-TB/DR-TB regimens and course, except that the treating physician should assess the drug interactions between anti-TB and anti-cancer drugs. For cancer treatment, drugs may have to be modified to accommodate anti-TB treatment and to aid better prognosis of the TB outcome. However, all decisions must be taken by a competent specialist after examining the individual case.
Curative resection, chemotherapy and radiation therapy are the mainstay treatment options for cancer in TB patients. Co-existence of TB in cancer patients necessitates anti-TB treatment with extended duration, if required. Follow-up during and after treatment also follows prevailing guidelines.
Prevention
Under the NTEP, TB prevention in cancer patients is essential and includes:
- Regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-Tumour Necrosis Factor (TNF) medicines.
- Education and referral of patients who do not have TB symptoms for TB infection testing/assessment of their eligibility for TPT.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis and Risk of Cancer: A Danish Nationwide Cohort Study, D. F. Simonsen et al., International Journal of Tuberculosis and Lung Diseases, The Union, 2014.
- Increased Risk of Active Tuberculosis after Cancer Diagnosis, Dennis F. Simonsen et al., Journal of Infection, 2017.
- Pulmonary Tuberculosis as Differential Diagnosis of Lung Cancer; MLB Bhatt et al., South Asian Journal of Cancer, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about cancer and TB is/are incorrect?
Under NTEP, regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-TNF medicines is done.
TB increases the risk of developing cancer, but cancer patients do not usually get TB.
Sputum smear microscopy is important when diagnosing TB in cancer patients.
All of the above
2
There is mutual risk between cancer and TB. TB increases the risk of developing cancer, and cancer patients are more likely to develop TB.
Yes Yes Pregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
-
-
CHO-M4: Adherence Managament
Fullscreen-
CHO-CH14: General Concepts in Adherence Managament
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
Treatment supporter to TB Patient
ContentA Treatment Supporter can be any person such as a Medical Officer, MPWs, community volunteers working with the program etc. Even a patient’s relative or family member can be a Treatment Supporter.
As per NTEP guidelines, salaried NTEP/General Health System staff may also be assigned as treatment supporters for a patient. However, they will not be eligible for any honorarium.
A patient can only be linked to one treatment supporter at a time in Nikshay.
Role of TS
-
CHO-CH15: Adherence Support
FullscreenRecording Adherence in Treatment card
Recording missed doses in Nikshay
ContentMissed Dose recording in Nikshay:
For recording missed doses in Nikshay, following steps should be followed:
Recording manual doses in Nikshay
ContentManual recording of Adherence in Nikshay:
in Nikshay, Adherence can only be recorded only if there is corresponding dispensation being issued to a Patient
Figure: Steps to record manual dose in Nikshay
Recording in Patient Treatment Card:
Figure: Filled Treatment card for TB Patient
-
CHO-CH16: 99 DOTS
Fullscreen99 DOTS- Features and Benefits
ContentVideo fileVideo: Features of 99 DOTS
Video fileVideo: Benefits of 99 DOTS
99 DOTS- Envelopes
ContentThe 99DOTS product consists of customised envelopes (see Figure 1) that fit around the tuberculosis medication blister pack distributed to patients.

Figure 1: 99DOTS Envelope
Universal Envelopes (Figure 2): Each adult patient gets the same sleeve, regardless of their weight band.
These are new envelopes that are currently being introduced by the program. Weight band wise envelopes will be used while the stock lasts, but new requirements by the state will be fulfilled by providing universal envelopes.
There are 2 types of these envelopes: 1 envelope for IP: Intensive Phase, and 1 envelope for CP: Continuation Phase, for both Macleods and Lupin Fixed-dose Combinations (FDCs). These envelopes are only to be used for adult patients on anti-TB treatment using FDCs.
Figure 3: Universal 99DOTS Envelopes 

Using the Universal Envelope
- The counsellor/ pharmacist/ treatment supporter write the number of pills per day the patient should take on the envelope.
- Every day, the patient will take the prescribed number of pills and reveal 1, 2, or 3 hidden phone numbers. The patient calls any one of the numbers they reveal that day.
- The patient should start at pill 1 and move in sequence (1,2,3…28), completing each column, and starting from the top of each row.
- The district should always have sufficient stock, which can be calculated as:
- Number of IP strips = Number of IP envelopes + some buffer
- Number of CP strips = Number of CP envelopes + some buffer
Advantages of the Universal Envelopes
- There is no need to estimate the requirements of weight band wise envelopes.
- Less space is required to store the envelopes.
- Stock-outs of envelopes for a particular weight band will not occur.
- It is easy for patients to follow the top to down arrow mark pattern while dispensing and ingesting medicines.
- Counselling time and dispensing time by pharmacists reduce per patient, thus increasing efficiency.
Resources:
- Nikshay 99DOTS Training Manual, 2021.
- Nikshay 99DOTS Universal Envelope Training Manual, 2021.
- 99 DOTS Website.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is correct about 99DOTS envelopes? The envelopes have medicine inside them. The envelopes have hidden numbers that can be called by the patient. There are weight-band wise envelopes. All of the above 4 99DOTS envelopes have anti-TB medicines with hidden toll-free numbers that patients call. These envelopes can be weight-band wise or universal envelopes. For weight-band wise 99DOTS envelopes, background colours differ for each weight band. True False 1 For weight-band wise 99DOTS envelopes, background colours differ for each weight band.
-
CHO-CH17: Medicine Event Reminder Monitor [MERM]
FullscreenMedication Event Reminder Monitor [MERM] Boxes
ContentThe Medication Event Reminder Monitor (MERM) is a digital pillbox that has been designed to monitor Multidrug-resistant TB (MDR-TB) treatment in resource-constrained settings, using relatively affordable technology and drugs provided by the National TB Elimination Programme (NTEP).

Figure: MERM Container for Shorter/ Longer Oral MDR-TB Regimen; Source: Guidelines for PMDT in India, 2021, p143.
- This system is specifically designed to be used with multiple blister-packaged TB medications in Drug-resistant TB (DR-TB) regimens.
- The MERM provides programmable visual and audible reminders of daily dosing and monthly refill by capturing data on pillbox opening as a proxy for dose ingestion.
- It transmits these data to a server so that Healthcare Providers (HCPs)/ treatment supporters can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
- In addition, by providing near real-time adherence data, the MERM can facilitate the identification of high-risk patients and prompt early intervention by HCPs to reduce non-adherence.
- When compared to facility-based Directly Observed Therapy (DOT) in which patients travel to clinics to be observed taking their medications, monitoring using the MERM may also reduce the required frequency of patient visits to TB clinics.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Standard Operating Procedure Manual - Procurement & Supply Chain Management, MOHFW, GOI.
Kindly provide your valuable feedback on the page to the link provided HERE
MERM Box: Components
ContentVideo fileVideo: MERM Box: Components
MERM Box: MERM Allocation in Nikshay
ContentVideo fileVideo: MERM Box: MERM Allocation in Nikshay
-
CHO-CH18: Adherence Monitoring and follow-up Action
FullscreenMonitoring of Adherence by NTEP Staff
Monitoring of Adherence by Pateint/TS
Adherence Summary Dashboard
ContentThe Adherence Summary dashboard is designed primarily for treatment supporters and field staff to help them monitor the day to day adherence statistics of their patients and incorporate necessary actions wherever required. This dashboard enables staff at district level hierarchies and below to view real-time adherence information of all patients on treatment.
The adherence summary dashboard is available in both Ni-kshay web portal as well as the mobile application.
Image
Figure 1: Adherence Summary Dashboard; Source: Ni-kshay Web Portal (L) and Ni-kshay Mobile Application (R)
Image
Figure 2: Adherence Summary Dashboard; Source: Ni-kshay Web Portal
Image
Figure 3: Adherence Summary Dashboard (contd.); Source: Ni-kshay Web Portal
Image
Figure 4: Adherence Summary Dashboard; Source: Ni-kshay Mobile Application
This dashboard provides a summary of the following:
- The Number of Patients currently enrolled on various Digital Adherence Technologies (99DOTS, MERM, VOT)
- Graph representing % of 'Average Adherence' of all patients on treatment
- Graph representing the % 'Digital Adherence' of all patients on treatment
- Real time update on the number of patients who have reported a dose (Digital + Manual) for the day and the number of patients who are yet to report a dose.
- Adherence Task Lists: This tab gives information on the number and proportion (%) of treatment interrupting patients based on the no. of doses missed, which helps the NTEP staff to undertake immediate actions to bring such patients back on treatment.
Resources
- Adherence Summary View, v5, Nikshay Knowledge base, India, 2022
- Ni-kshay 2.0 App User Guide, CTD, MoHFW, India, 2018.
- Adherence Monitoring in Ni-kshay Version-2.0, CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Identify the correct statement from the options below Adherence summary dashboard allows viewing only digital adherence of the patients Adherence summary dashboard allows viewing only average adherence of the patients Adherence summary dashboard allows viewing both digital and average adherence of the patients. None of the above 3 Adherence summary dashboard allows viewing both digital and average adherence of the patients. Yes Yes
-
-
CHO-M5: Public Health Action
Fullscreen-
CHO-CH19: Patient Support
FullscreenPublic Health Actions
ContentPublic Health Action is conducted under the NTEP programme to support and prevent further health complications among TB patients after diagnosis.
Figure: Various activities under Public Health Action
Nutritional Support
ContentNutrition constitutes an important part of TB Treatment. Undernutrition increases the risk of Tuberculosis (TB), and in turn, TB can lead to malnutrition. It has been demonstrated that undernutrition is a risk factor for progression from TB infection to active TB disease, and undernutrition at the time of diagnosis of active TB is a predictor of increased risk of death and TB relapse. There is, as yet, little evidence showing that additional nutrition support improves TB-specific outcomes, but low body mass index, as well as lack of adequate weight gain during TB treatment, are associated with an increased risk of TB relapse and death.
The following table illustrates the effect of undernutrition on outcomes in TB.
Effects on disease
- Increased severity of disease
- Increased risk of death
Effects on treatment
- Delayed sputum conversion
- Risk factor for drug-induced hepatotoxicity
- Malabsorption of rifampicin
- Reversion of positive cultures in Multidrug-resistant (MDR) -TB
Effects on long-term outcomes
- Increased rate of relapse
Effects on contacts
- Increased incidence in undernourished contacts
The basic recommendations to address the nutritional needs of TB patients are discussed below.
- Conducting an initial nutrition assessment of TB patients with further monitoring
- Providing ongoing counselling for patients on their nutritional status; Diet for TB patients starting treatment should include: cereals (maize, rice, sorghum, millets, etc.), pulses (peas, beans, lentils, etc.), oil, sugar, salt, animal products (canned fish, beef and cheese, dried fish), and dried skimmed milk
- Managing severe acute malnutrition according to national guidelines and WHO recommendations
- Managing moderate undernutrition for TB patients who fail to regain normal Body Mass Index (BMI) after two months of TB treatment or appear to lose weight during TB treatment and evaluating for proper treatment adherence and other comorbidities. If indicated, these patients should be provided with locally available nutrient-rich or fortified supplementary foods.
- Special categories of TB patients, such as:
- Children who are less than 5 years of age should be managed as any other children with moderate undernutrition.
- Pregnant women with active TB and patients with MDR-TB should be provided with locally available nutrient-rich or fortified supplementary foods.
6. Micronutrient supplementation for all pregnant women as well as lactating women with active TB. These women should be provided with iron and folic acid and other vitamin and minerals to complement their maternal micronutrient needs. In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
To achieve the above objectives, the guidelines for nutrition for TB patients are available and a mobile application (N-TB) is available for decision-making on nutritional support for TB patients.
Improving nutritional status at a population level is important for TB prevention which should be part of broader actions on social determinants. All efforts should be made to link TB patients for nutritional support which can be done through the existing public distribution system, local self-government or Non-governmental Organisations (NGOs)or donor agencies or through the corporate sector under Corporate Social Responsibility (CSR).
Resources
- Guideline: Nutritional Care and Support for Patients with Tuberculosis, WHO, 2013.
- Guidance Document: Nutritional Care and Support for Patients with Tuberculosis in India, MoHFW, WHO, CTD, 2017.
- Training Modules (1-4) For Programme Managers & Medical Officer NTEP, CTD, WHO, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, MoHFW, WHO, 2021.
Assessment
Question 1
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of Pre-Test
Part of Post-Test
Undernutrition doesn’t affect the outcomes of TB.
True
False
2
Undernutrition affects the outcomes of TB in terms of treatment.
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Support for deaddiction
ContentSubstance use has been one of the major reasons for non-adherence to TB treatment and therefore, the National TB Elimination Programme (NTEP) has implemented several initiatives for control and de-addiction of substance use in association with various other health programmes like the National Tobacco Control Programme (NTCP), Drug De-Addiction Programme (DDAP), etc.
NTEP has also included referral services to de-addiction facilities for TB patients as a part of the ‘Standards for TB Care in India (STCI)'.
Deaddiction Services and Linkages
- Brief substance use counselling during the pre-treatment, treatment initiation and regular follow-up counselling sessions by the trained NTEP staff.
- Referral to National Tobacco Quitline provides telephonic counselling via the toll-free number in English and Hindi languages 8 a.m. to 8 p.m. between Tuesday to Sunday.
- Referral to mCessation Programme provides evidence-based behavioural change Short Text Messages (SMSs) in English and Hindi languages on mobile phones, which include health information on tobacco use hazards, tips on quitting, and encouragement for those attempting to do so.
- Referral to nearest Tobacco cessation clinics/ centres in the government facilities.
- Referral under the Drug De-Addiction Programme (DDAP) wherein affordable, easily accessible and evidence-based treatment for all substance use disorders are provided through the government health care facilities of the Ministry of Health and Family Welfare, viz., All India Institute of Medical Sciences (AIIMS), New Delhi; Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh; National Institute of Mental Health and Neuro-Sciences (NIMHANS), Bengaluru; Dr Ram Manohar Lohia (RML) Hospital, New Delhi; AIIMS, Bhubaneswar; and Central Institute of Psychiatry (CIP), Ranchi.
Resources
- National Strategic Plan 2017-2025 for TB Elimination in India, MoHFW, India, 2017.
- National Framework for Joint TB-tobacco Collaborative Activities, MoHFW, India, 2017.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What service does the National Tobacco Quitline provide?
Telephonic counselling
Face-to-face counselling
None of the above
Both 1 & 2
1
National Tobacco Quitline: Telephonic counselling via the toll-free number in English and Hindi languages.
Yes
Yes
Support for Rehabitilation
Travel support for TB Patient
ContentEliminating the catastrophic expenditure on TB patients and their families has been an important goal of the World Health Organisation's (WHO’s) END TB strategy.
The National TB Elimination Programme (NTEP) has also attempted the same through various partnerships and one of the action plans under this strategy was to provide transport allowance to cover the TB treatment-related travel costs of the TB patients as well as their attendants.
Travel cost for Drug-resistant TB (DR-TB) patients
- Travel costs are reimbursed for DR-TB patients travelling to District or Nodal DR-TB Centre for initiation/ follow-ups/ adverse reaction management during the treatment, along with one accompanying person/ attendant.
- The reimbursement is as per actual cost per visit through public transport with a limit of up to Rs. 400 per visit within the district and up to Rs. 1000 per visit for outside district travel.
Travel cost for TB Patients in tribal/ hilly/ difficult areas
- TB Patients from tribal /hilly/difficult areas are provided with an aggregate amount of Rs. 750 as transport allowance to cover patients and the attendants' travel costs.
- Rs. 750 as a one-time payment at the time of notification.
Travel cost for Presumptive TB patients to visit District TB Centres (DTC)/ collection centres for testing
- Presumptive TB patients travelling to DTC/ collection centre are reimbursed as per actual cost with public transport.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
- Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme. Central TB Division, Ministry of Health & Family Welfare, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How much amount is provided as transport allowance to tribal/ hilly area patients and their attendants during their TB treatment
Rs.250
Rs.500
Rs.750
Rs.1000
3
Rs. 750 is provided as transport allowance to Tribal/ hilly area patients and their attendants during their TB treatment.
Yes
Yes
Nikshay Poshan Yojana
ContentNikshay Poshan Yojana (NPY) is one of the four initiative-based support schemes which provides financial support to TB patients for their nutrition. A financial incentive of Rs. 500 per month will be provided to patients on anti-TB treatment till the completion of treatment.
- All TB patients who are registered/ notified (from both public/ private sectors) on the Nikshay Portal on or after 1st April 2018 are beneficiaries of the scheme.
- The incentive is paid in cash and will be deposited to the Aadhaar enabled bank account of the patient. In the case of paediatric TB patients, money will be deposited in parents'/ guardians’ accounts.
- The first instalment of Rs. 1000 total for the first 2 months is expected to be disbursed immediately after starting treatment. To ensure treatment adherence, after the first instalment, the conditionality of follow-up examination is applicable.
- Each month of treatment extension, Rs. 500 will be transferred to the patient's DBT account, till the treatment is continued.
- In some states, where the incentive is transferred in-kind, they should provide food baskets with a total value not less than the corresponding eligible benefit.

Figure: Aims of Nikshay Poshan Yojana
The health volunteer/ Treatment supporter, Multi-purpose Health worker in-charge, or the Senior Treatment Supervisor (STS), are responsible to collect the bank details of the patient from the field level and enter it on the Ni-kshay.
Resources
Nutritional Support DBT Scheme Details, CTD.
Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, CTD, 2020.
Guidelines for Programmatic Management of Drug-resistant TB in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Only patients seeking treatment in public hospitals are eligible for Nikshay Poshan Yojana. True False 2 All patients who are receiving treatment from both public and private sectors and are notified on the Nikshay platform are eligible to receive the benefit. Linkages to Social Welfare Schemes
ContentThe government of India introduced Direct Benefit Transfer (DBT) to ensure that the benefits and subsidies are reaching the beneficiaries directly and to fasten the process. Through the process, money is directly transferred to the beneficiaries' bank account keeping the intermediary agencies and stakeholders only to manage the process of payment.
National TB Elimination Programme (NTEP) transfers all benefits to patients using the two systems:
- Nikshay
- Public Finance Management System (PFMS)
DBT Schemes available in the NTEP
Nikshay Poshan Yojana (NPY)
Objective: To provide nutritional support to TB patients at the time of notification and subsequently during the course of treatment.
Beneficiary: All unique TB patients notified on or after 1st April 2018 (including all existing TB patients under treatment for at least one month from this date).
Benefit Amount: Rs. 500 for a treatment month paid in instalments of up to Rs. 1000 as an advance.
Transport Support for TB patients in Notified Tribal Areas
Objective: To provide financial support as transport allowance for TB patients belonging to notified tribal areas (in addition to the nutritional support provided under NPY).
Beneficiary: All notified TB patients from notified tribal areas.
Benefit Amount: Rs. 750 as a one-time payment at the time of notification.
Incentives for Private Sector Providers and Informants
Objective: To provide financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by a private provider.
Beneficiary: Private providers (private practitioner, hospital, laboratory and chemist) who notify TB patients to NTEP on Nikshay.
Incentive Amount: Rs. 500 as a one-time payment on notification and Rs. 500 to a private practitioner or hospital for updating the patient’s treatment outcome.
Treatment Supporters’ Honorarium
Objective: To provide an honorarium to the treatment supporters for supporting TB patients.
Beneficiary: Community Treatment Supporters who support patients during treatment, leading to a successful outcome (cured or treatment completed).
Incentive Amount: Rs. 1,000 as a one-time payment on the update of outcome for drug-sensitive TB patients and Rs. 2,000 on completion of Intensive Phase (IP) and Rs. 3,000 on completion of Continuation Phase (CP) of treatment for drug-resistant TB patients.
Criteria/ Pre-requisites for Availing the Benefits in NTEP
- All benefits are processed for the respective beneficiary base on the rules and eligibility criteria defined above except for the treatment supporter, which needs to be manually uploaded by the TB Unit (TU) level staff.
- Beneficiary ID in Nikshay will be assigned to all patients which are unique. The benefits processed will be tracked under this ID. All beneficiaries need to register their bank details in Nikshay to enable DBT.
Treatment Supporter
A trained treatment supporter, who can be a health worker or community volunteer, will assist the patient to adhere to the drugs, provide counselling support, nutritional support, screen for adverse reactions, psycho-social support, comorbidity management and follow-up laboratory investigations.
The Treatment Support Honorarium is available as per the following eligibility:
- The treatment Supporter must be registered in Nikshay and designated as the primary Treatment Supporter.
- The linked patient must complete treatment or has to be cured.
- The treatment Supporter should not be a salaried government employee.
Resources
Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, CTD, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Only patients and treatment supporters seeking treatment in the public sector are eligible for DBT benefits.
True
False
2
Private providers are eligible for financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by them.
PMJAY
Content
Figure: Components of Ayushman Bharat Yojana
Pradhan Mantri Jan Arogya Yojana (PM-JAY) is one of the two key components of the Ayushman Bharat Yojana launched by the Government of India as part of the National Health Policy 2017. It is one significant step toward achieving Universal Health Coverage (UHC) and Sustainable Development Goal - 3 (SDG3): Good health and well-being.
Aim
To provide health protection cover to poor and vulnerable families against financial risk arising from catastrophic health episodes.
Provisions
- Financial protection (Swasthya Suraksha) to 10.74 crore poor, deprived rural families and identified occupational categories of urban workers’ families as per the latest Socio-Economic Caste Census (SECC) data (approx. 50 crore beneficiaries). It will offer a benefit cover of Rs. 5,00,000 per family per year (on a family floater basis).
- Cover medical and hospitalisation expenses for almost all secondary care and most of the tertiary care procedures. PM-JAY has defined 1,350 medical packages covering surgery, medical and daycare treatments, including medicines, diagnostics and transport.
- To ensure that nobody is left out (especially girl child, women, children and the elderly), there will be no cap on family size and age.
- Cashless & paperless at public hospitals and empanelled private hospitals.
- Beneficiaries are not required to pay any charges for hospitalisation expenses.
- Benefit also includes pre and post-hospitalisation expenses.
- The scheme is entitlement based; the beneficiary is decided based on the family being figured in the SECC database.
Benefits for the Health Care System of the Country
- Helps to achieve UHC and SDG.
- Ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially the not-for-profit providers.
- Significantly reduces out-of-pocket expenditure for hospitalisation. Mitigates financial risk arising out of catastrophic health episodes and consequent impoverishment for poor and vulnerable families.
- Acts as a steward, align the growth of the private sector with public health goals.
- Promotes the use of evidence-based health care and cost control for improved health outcomes.
- Strengthens public health care systems through the infusion of insurance revenues.
- Enables the creation of new health infrastructure in rural, remote and under-served areas.
- Increases health expenditure by the government as a percentage of Gross Domestic Product (GDP).
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
PM-JAY benefits can be redeemed only from government hospitals.
True
False
2
PM-JAY provides cashless & paperless benefits at public hospitals and empanelled private hospitals. It ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially not-for-profit providers.
Yes
Yes
-
CHO-CH20: TB Arogya Sathi App
FullscreenTB Aarogya Sathi
ContentTB Aarogya Sathi empowers Citizens(including TB Patients under NTEP) and to serve as a Direct interface with the healthcare system. The App is aimed at augmenting the initiatives of the Central TB Division, Government of India in proactively increasing awareness among the citizens and ensuring availability of free and quality assured drugs and diagnostics to all citizens in the country.
Citizens using the TB Aarogya Sathi App will have access to common FAQs regarding TB, Information on the symptoms of TB and Side effects of Anti TB drugs. Using the app, any user will be able to find the closest health facilities that can assist in diagnosis of TB.
Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
Citizen:
- Informative Content available for all Citizens using the App(no login required to access this content)
- Information on TB
- Symptoms of TB
- Side Effects of TB
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Motivational Videos
- Nutritional Advice
Patient:
- Patients registered in Nikshay get access to additional information(after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code
Figure: TB Aarogya Sathi Application snapshot
- Informative Content available for all Citizens using the App(no login required to access this content)
Download the Tb Arogya Sathi App and Steps to Login
ContentVideo fileVideo: Download the Tb Arogya Sathi App and Steps to Login
Health Facilities
ContentVideo fileVideo: Health Facilities
Summary and Treatment Progress View
ContentVideo fileVideo: Summary and Treatment Progress View
View Adherence Details
ContentVideo fileVideo: Adherence Details and DBT Details View
View DBT Details
ContentVideo fileVideo: DBT Details View
Adding bank details in the Arogya Sathi App
ContentVideo fileVideo: Adding bank details in the Arogya Sath App
Symptom Checker-Overview
ContentVideo fileVideo: Symptom Checker-Overview
Screening for Self and Others
ContentVideo fileVideo: Screening for Self and Others
Post enrolment follow-up cycle in Nikshay
ContentVideo fileVideo: Post enrolment follow-up cycle in Nikshay
-
CHO-CH21: Contact Investigation
FullscreenContact Tracing and Investigation
ContentContact tracing is a process to identify people who are at a high risk of developing TB due to their contact with a known TB case.
The aim of contact tracing is to find other people with TB disease and those infected with TB
All close contacts, especially household contacts of a Pulmonary TB patient, should be screened for TB.
In paediatric TB patients, reverse contact tracing for the search of any active TB case in the child's household must be undertaken.
Particular attention should be paid to contacts with the highest susceptibility to TB infection.
Figure: Contacts to be Prioritized for contact TB screening
Importance of Contact tracing
How to do contact tracing
ContentIndex TB patient: Initially identified person of any age with new or recurrent TB in a specific household or other comparable settings in which others may have been exposed. The Index TB patient is the person on whom a contact investigation is centred, but is not necessarily the source/ primary case.
Contact: Any individual who was exposed to a person with active TB disease
Household Contact (HHC): Person who shared the same enclosed living space as the index TB patient for one or more nights or for frequent or extended daytime periods during the three months before the start of current TB treatment.
Close contact: Person who is not in the household but shared an enclosed space, such as at a social gathering, workplace or facility, for extended periods during the day with the index TB patient during the three months before the commencement of the current TB treatment episode.
Contact tracing: Contact tracing is the process of listing out all the contacts (household contacts and close contacts) of the index TB patient. Contact tracing has to be done for all Index TB cases, whether pulmonary (sputum positive or negative) or Extra-pulmonary (EPTB). As per the current policy, it is compulsory to trace household contacts but it is desirable to trace other close contacts (workplace, social gathering etc) also.
Why Contact Tracing is done: Contact tracing is followed by contact investigation to identify active TB cases and Tuberculosis Preventive Treatment (TPT) beneficiaries.
Contact investigation: This is a systematic process for identifying previously undiagnosed people with TB disease and TB infection, among the contacts of an index TB patient.
Conducting Contact Tracing and Contact Investigation
Once a new/ recurrent TB case is diagnosed (ideally within 1 week), a healthcare worker (usually the Multipurpose Worker (MPW) from the nearby public health facility visits/ tele calls the patient’s household, interviews the patient about his/her contacts in the household and other settings such as workplace or social gatherings. The contacts’ details are recorded in a standardised format and entered in Ni-kshay contact tracing module. Each contact's details enter the workflow as a presumptive TB case or TPT beneficiary.
The traced contacts are screened for TB using a symptom checklist and if found to have any symptoms suggestive of TB, they are tested using X-ray/ sputum microscopy/ Cartridge-based Nucleic Acid Amplification Test (CBNAAT) as required.
Outcome of Contact Tracing and Contact Investigation
- Those contacts diagnosed with active TB are initiated TB treatment.
- As per the current policy, those HHC of sputum-positive Pulmonary TB (PTB), in whom active TB disease is ruled out, are considered for TB Preventive Therapy (TPT)
References
- Guidelines for Programmatic Management of TB Preventive Treatment in India, 2021.
- Technical and Operational Guidelines for Tuberculosis Control in India, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements are true?
Contact tracing should always be followed by contact investigation.
Household contacts of Extrapulmonary TB are offered TPT.
The index case is always the primary source of infection in the household.
Contact tracing and investigation need to be done only during ACF campaigns.
1
2- Only HHC of Sputum positive PTB cases are offered TPT.
3 – The index case need not be the primary source of infection in the household.
4 – Contact tracing and investigation are to be done routinely for all TB cases. ACF campaigns are only an added measure.
Yes
Yes
Recording and Reporting Contact Tracing [Ni-kshay]
ContentContact Tracing plays an important role in the detection of all those who are secondarily infected for proper diagnosis and prompt treatment. This process can be recorded and reported in Ni-kshay under the ‘contact tracing’ option. The process of recording contact tracing in Ni-kshay is given below.
Process Overview
Image
Detailed Step-wise Procedure
Step 1: Login to the Ni-kshay ecosystem and enter the patient ID for which the contact tracing details are being recorded.
Step 2: Click on the ‘Contact tracing’ tab to reach the contact tracing window.
Image
Step 3: Click on the 'Edit' tab and fill in the relevant information in the fields provided.
Image
Step 4: Once the details are entered, click on the ‘update’ tab present at the upper right corner of the window to finish the process. A message will be displayed by the system once the details are updated successfully.
Image
Step 5: Once the details are updated successfully, an option to add the contact will appear at the upper right corner of the contact tracing window. This option can be used to add contacts as Beneficiaries (Presumptive TB/ TB Preventive Treatment (TPT) beneficiaries) in the system.
Image
Step 6: Selecting the 'Add contact' tab will take the user to the enrollment window. The process of entering information in this window is similar to adding a New presumptive TB case in Ni-kshay, except that the option of “Contact of Known TB Patient” is automatically selected for the field “Key Population”.
Once the contact is added as a beneficiary (Presumptive TB/ TPT beneficiary) in the system, the contact details can be seen in the contact tracing tab.
Video fileVideo: Recording Contact tracing in Ni-kshay (Web)
Video fileVideo: Recording Contact tracing in Ni-kshay (Mobile App)
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Pre-test Contact tracing plays an important role in the detection of all those who are secondarily infected. False True 2 Contact tracing plays an important role in the detection of all those who are secondarily infected for proper diagnosis and prompt treatment. Yes Yes
-
CHO-CH22: Counselling and education
FullscreenTB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
-
CHO-M6: DBT
Fullscreen-
CHO-CH23: General Concepts
FullscreenDirect Benefit Transfer(DBT) under NTEP
ContentDirect Benefit Transfer (DBT) is a major initiative of Government of India (GoI) whereby any government subsidy or benefit is to be transferred directly into the beneficiary's bank accounts. Intermediary government agencies only manage the process of payments, without handling actutal money.
NTEP is one of the first health programmes in India to use a fully adopt DBT. It uses an end to end electronic system, to digitise beneficiary information and transfer monetary benefits. In NTEP to process benefits, two electronic systems are used, Ni-kshay (operated by NTEP) and PFMS (Public Finance Management System, operated by the Ministry of Finance). Ni-kshay enables Direct Benefit Transfer by digitizing the beneficiaries(bank account details of patients, treatment supporters and providers) and calculates of incentives/ benefits (eligible payment) and processes them for payment through PFMS under various schemes. The various schemes operational under NTEP are:
- Nikshay Poshan Yojana(NPY)
- Tribal Support Scheme
- Treatment supporter’s Honorarium
- Incentive for Notification and Outcome
Stakeholders/Systems for DBT under NTEP
Content- Beneficiary: These are the individuals who get benefits from payments under a particular scheme. E.g., all notified TB patients are beneficiaries under the Ni-kshay Poshan Yojana. An individual may be eligible for multiple payments under one scheme or may be eligible for multiple schemes. Only individuals with bank accounts will receive these benefits. Also, beneficiaries and their bank accounts need to be approved by a district-level authority to receive any of the benefits from Ni-kshay.
- Processing authorities: The DBT maker and checker are designated personnel in the health system for in processing benefits. They are responsible for the two levels of verification in Ni-kshay; confirming and approving each benefit under their jurisdiction. Both maker and checker are roles that are assigned to any personnel in NTEP as decided by the District TB Officer. They perform their role through a special staff login in Ni-kshay with the designation “DBT Maker” or “DBT Checker,” created under the staff management module of Ni-kshay.
- DBT Maker: Maker acts at the TU level. All benefits created are assigned to the maker, who has to reconfirm the eligibility manually, update necessary details if required and send the benefit to the checker for approval.DBT maker is created by the District Tuberculosis Officer (DTO) upon request from the Medical Officer Tuberculosis Center (MOTC).
- DBT Checker: DBT checker acts at the district level. Checker is responsible for approving all beneficiaries under the district once it has been created by the DBT makers at TU levels. DBT checker role in Ni-kshay app is created by the State TB Officer (STO).
Resources
- Introduction to DBT, Ni-kshay Knowledge Base.
- https://tbcindia.gov.in/WriteReadData/NTEPTrainingModules5to9.pdf
- Direct Benet Transfer Manual for National Tuberculosis Elimination Programme; MoHFW, Government of India, 2020.
Assessment
Question Answer 1 Answer 2 Answer3 Answer 4 Correct Answer Correct explanation An individual is only eligible for a benefit under NTEP at one point in time. True False 2 An individual may be eligible for multiple payments under one scheme or may be eligible for multiple schemes. DBT Schemes in NTEP
ContentSchemes Beneficiary Benefit Amount Nikshay Poshan Yojana(NPY) - All Notified TB Patients in Nikshay from the point of diagnosis
Rs. 1000 at the time of Notification and Rs 500 per treatment month there after paid in advance as installments. Tribal Support Scheme Confirmed TB Patients residing in Tribal TU Rs 750(one time) at the time of notification Treatment supporter’s Honorarium Treatment supporters of patients who have achieved outcome of treatment success - Rs 1,000 in the case of DS TB patients and Rs 5,000 in the case of patients, paid at the time of treatment completion.
Incentive for informants, Notification and Outcomes Private Health Facilities: including Practitioner /Clinic etc.(Single), Hospital/Clinic/Nursing Home etc.(Multi), Laboratories and Chemists
Any citizen reporting TB patients to public health facility or a self-reporting by patient may also be incentivized as an informant
- Rs 500 for Notification or informant
- Rs. 500 for Outcome declaration to health facilities.
-
-
CHO-M7: Private sector Engagement
Fullscreen-
CHO-CH24: Partnership Options
FullscreenPHA for patient notified from the private sector
ContentAs a public health responsibility to prevent transmission of TB infection and development of drug resistance it is essential to engage both the public and private sectors for effective TB prevention and control. A total of seven standards related to Public Health Actions (PHA) (Standard 12 to Standard 18) have been mentioned in the Standards for TB Care in India (STCI)-2014. All patients notified from the private sector also need to be offered all public health actions.
This could be achieved in collaboration with the local public health services and/or other agencies.
1) Provide Access to Correct and Complete Diagnosis for Private Sector Patients
- In this regard all private providers must be sensitized, and their capacities must be built with respect to early diagnosis, prompt referral for sputum smear examination to the National TB Elimination Programme (NTEP) diagnostic facilities / NTEP accredited private labs.
- All private providers and chemists/pharmacists must mandatorily notify the TB patients to the local health authorities – District Health Officer / District TB Officer.
2) Provide Support for Treatment Adherence
- A treatment support plan must be developed at the time of treatment initiation for all patients in the private sector too, in mutual consultation with patient and private provider.
- All patients receiving treatment from the private sector must also be eligible to receive counselling services and upon consent, home visit counselling sessions (or at the location convenient to the patient) may be provided to patients and their caregivers under the NTEP’s Public Private Mix (PPM) or in association with partner agencies providing counselling services under NTEP.
- Any instance of treatment interruption must be reported at the earliest through Ni-Kshay.
- The patients may also be linked to Ni-Kshay call-centers for adherence support.
- The NTEP has also partnered with Patient Provider Support Agency (PPSA) / Patient Provider Interface Agency (PPIA) wherein vouchers were provided to private sector TB patients for utilizing subsidized TB diagnostic and follow up investigation services and can be scale up in high burden districts across the country with support from state governments/ Corporate Social Responsibilities (CSR) agencies.
4) Contact Tracing and TB Preventive Treatment
- All private providers must hold a responsibility to ensure that persons in close contact with patients who have infectious tuberculosis are evaluated at the earliest and managed in line with NTEP recommendations. The district health officers and district TB officers must be responsible to ensure this is being done on a regular basis.
- Eligible contacts should also be counselled for initiation of TB preventive treatment.
5) Linkage to Social Welfare and Protection
- Upon notification by the private provider and initiation of appropriate TB treatment, all patients seeking treatment under the private sector become eligible to receive direct benefit transfer (DBT) under the government of India's Nikshay Poshan Yojana (NPY)
- In districts where PPSA is available, PPSA staff may perform the linkage of private sector patients to DBT services and in districts where PPSAs are not available, the TB Health Visitor/ Senior Treatment Supervisor (STS) needs to undertake the public health action under the supervision of the PPM Coordinator.
- The patients may also be guided and linked to various other social protection and welfare schemes available under central and state governments. The partner agencies with expertise in referral linkages shall help the NTEP in achieving this.
6) Liaison with Professional Bodies
- Professional bodies such as Indian Medical Association and Indian Pharmaceutical Association must be involved for advocacy regarding the services available under public health actions of NTEP for the private patients.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, GoI, 2021.
- Mandatory TB Notification Gazette for Private Practitioners, Chemists and Public Health Staff, RNTCP, 2018.
- Notification of TB Cases: Amendments, MoHFW, GoI, 2015.
- TB Notification Order, MoHFW, GoI, 2012.
- National Strategic Plan for Tuberculosis Elimination 2017-2025, RNTCP, CTD, MoHFW, 2017.
- Standards for TB Care in India, WHO, 2014.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Linkage of private sector TB patients to available social support schemes is a part of public health action. True False 1 Linkage of private sector TB patients to available social support schemes is a part of public health action Yes Yes Mandatory Notification of TB Diagnosis
ContentTB is a notifiable disease in India, and TB notification has been made mandatory at the point of diagnosis since May 2012. This means that when a case of TB is diagnosed and/or put on treatment it is to be reported to the NTEP.
- Every healthcare provider, i.e., clinical establishments run or managed by the Government (including local authorities), private or NGO sectors and/or individual practitioners, need to notify diagnosed or treated TB patient’s.
- Reporting is to be done on the online reporting system called Nikshay and should include details of patient identification, and TB diagnosis.
- This, apart from enabling essential public health actions such as Treatment initiation, and Contact Tracing, chemoprophylaxis, but also enables provisions of Direct beneficiary transfer for Nikshay Poshan Yojana
Points to Note:
As per MCI code of ethics a registered medical practitioner giving incorrect information on his name and authority about notification amounts to misconduct and such a medical practitioner is liable for deregistration. It is the duty of the registered medical to divulge this information to the authorized notification official as regards communicable and notifiable diseases.
Resources
Schedule H-1 Regulation
ContentUnder the Drugs & Cosmetics Rules 1945, drugs specified under Schedule H are required to be sold by retail on the prescription of a Registered Medical Practitioner (RMP) only. At present, Schedule H contains 510 drugs.
Recently, a new Schedule H1 has been introduced through gazette notification GSR 588 (E) dated 30-08-2013, which contains certain third and fourth-generation antibiotics, certain habit-forming drugs and anti-TB drugs.
These drugs are required to be sold in the country under the following conditions:
(1) The supply of a drug specified in Schedule H1 shall be recorded in a separate register at the time of the supply giving the name and address of the prescriber, the name of the patient, the name of the drug and the quantity supplied and such records shall be maintained for three years and be open for inspection.
(2) The drug specified in Schedule H1 shall be labelled with the symbol "Rx" which shall be in red and conspicuously displayed on the left top corner of the label, and shall also be labelled with the following words in a box with a red border:
“Schedule H1 Drug Warning:
-It is dangerous to take this preparation except in accordance with the medical advice.
-Not to be sold by retail without the prescription of a Registered Medical Practitioner.”
List of anti-TB drugs included in Schedule H1
- Ethambutol hydrochloride
- Ethionamide
- Isoniazid
- Levofloxacin
- Moxifloxacin
- Pyrazinamide
- Rifabutin
- Rifampicin
Obligations of Chemists with Regard to Sales of Anti-TB Drugs Under Schedule H1
- Mandatorily keep a copy of the prescription of drugs covered under Schedule H1 in a separate record and such record should be maintained for three years and be available for inspection.
- The supply of a drug specified under schedule H1 shall be recorded in a separate register at the time of supply giving the name and address of the prescriber, the name of the patient, the name of the drug and the quantity supplied and such record shall be maintained for three years and be open for inspection (Annexure IV).
Table: Annexure IV – Schedule H1 Drugs Record Format; Source: Frequently Asked Questions on Gazette on Mandatory TB Notification for Chemists/ Pharmacies. tbcindia.gov.in.
Sl No:
Date
Name of doctor/ prescriber
Address & Reg. No:
Name of patient & address
Name of drug
Batch number
Expiry
Quantity sold
Bill no.
Resources
- Rules for Selling of Drugs Under Schedule H1, Press release by MoHFW, 2013.
- The Drugs & Cosmetics Act and Rules, Ministry of Health & Family Welfare, Government of India, 2016.
- Frequently Asked Question on Gazette on Mandatory TB Notification for Chemists/ Pharmacies, Central TB Division.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Schedule H1 drugs can be sold without the prescription of a registered medical practitioner.
True
False
2
Schedule H1 Drug Warning:
-It is dangerous to take this preparation except in accordance with the medical advice.
-Not to be sold by retail without the prescription of a Registered Medical Practitioner.”
Yes
Yes
-
-
CHO-M8: ACSM and Community Engagement
Fullscreen-
CHO-CH25: Guidelines and Protocols for ACSM activities
FullscreenOrganising Community meetings
ContentCommunity meetings are organised by the Senior Treatment Supervisor (STS) or the partner Non-Government Organisation (NGO) under the supervision of the Medical Officer.
- These meetings are conducted to create awareness about TB among the general population, community leaders, people’s representatives, Self-help Groups (SHGs), community volunteers, traditional healers, etc.
- These meetings are organised in a community centre or any other suitable place at the village and slum level.
- To maximise the output, the community meetings should be planned appropriately.
Following are the steps involved in planning a community meeting:
Image
Resources
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who supervises the conduct of community meetings? DTO STO MO STLS 3 Community meetings are organised by the STS or the partner NGO under the supervision of the Medical Officer. YES YES Community mobilization strategies-Tribal areas
ContentTribal people (10.4 Cr, 8.6% of total population) have higher prevalence (703 per 100,000) of TB compared to national average (256 per 100,000).10.4% of all TB notified patients are from tribal communities. The National TB program has prioritized this subgroup of population through Tribal Action Plans since 2005.
As a part of the Multisectoral collaboration with various Ministries, a guidance note on the joint action plan was developed by Ministry of Health and Family Welfare (MoHFW) and Ministry of Tribal Affairs in October 2020 and shared with the Secretaries of all States/ UTs for field level implementation. Tribal TB initiative, a unique partnership between the Ministry of Health and Family Welfare and Ministry of Tribal Affairs was initiated to improve the cascade of TB care and support services among Tribal Populations in India. The technical assistance for this initiate will be provided by USAID.
Challenges in communities in tribal areas:
Access, availability, and utilization of TB care services of these communities are hindered by:
- Geographical barriers
- Poor state of social determinants
- High impact of malnutrition, insufficient community involvement
- Health system constraints including lack of trained human resources
- Cultural and communication gaps between the care provider and the community, etc.
- The COVID-19 pandemic has probably further worsened the situation.
Community mobilization strategies in tribal areas:
Image
Various departments which play a role in community mobilization in Tribal areas:
- National Program Management Unit (NPMU) provides technical assistance in monitoring and implementation of the Tribal TB Initiative.
- Coordination among National Tuberculosis Elimination Programme (NTEP), National Health Mission (NHM), Ministry of Development of Northeastern Region, Ministry of Tribal affairs at National, state and district levels through national level Technical Support Unit.
Image
- Coordination with ‘Centre of Excellence’ within the Ministry of Tribal Affairs, with a key focus on TB.
- Partnering with private sector players for leveraging resources for TB elimination in Tribal communities.
- Documenting best practices, and commission tribal health research studies in collaborations with identified government institutions.
- Various departments collaborate for improving the operational excellence of existing demand-side interventions such as Village Health Sanitation and Nutrition Days (and committees), Jan Arogya Samiti platforms, Jan Andolan initiatives, engaging TB-Champions, and training of faith healers and other community influencers.
Resource
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Community mobilization strategies in tribal areas include home visits. True False 1 Community mobilization is about seeking cooperation and support from different stakeholders in general and the community in specific.
Home visits will improve awareness on various government schemes, provisions, facilities available for TB patients and to improve treatment literacy and adherence among TB patients in tribal areas.
Community mobilization strategies-Rural areas
ContentRural populations have more limited access to primary care physicians than residents of urban areas, and are older, sicker, and poorer than urban counterparts. Travel to reach a primary care provider may be costly and burdensome for patients living in remote rural areas, with subspecialty care often being even farther away. These patients may substitute local primary care providers for sub specialists, or they may decide to postpone or forego care. Many social determinants act as barriers for rural communities to access health services.
Challenges faced by communities in rural areas are:
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
- Cultural and social norms surrounding health behaviors
- Low health literacy levels and incomplete perceptions of health
- Linguistic and educational disparities
- Limited affordable, reliable, or public transportation options
- Unpredictable work hours or unemployment
- Poor primary healthcare and infrastructure in rural areas
- Lack of access to tuberculosis testing and treatment centers in remote unreached areas
- Unregulated indigenous system of medicine
- Poor airborne infection control
- Poor nutrition and Malnourishment
Community mobilization strategies in rural areas include:
Image
Various committees which play a role in community mobilization in rural areas:
Image
- Village Health Sanitation and Nutrition Committees (VHSNCs) - In each Gram Panchayat, Village Health Sanitation and Nutrition Committees (VHSNCs) have been formed at the village level under National Health Mission (NHM). These committees are entrusted with community-level planning and implementation of health and sanitation, and have representation from the local government, local health centre, and the local community.
- Panchayat Raj Institution (PRI) - Members of PRI refers to local self-government at the village level. The village pradhan (head) and members of the Panchayat are elected members of the Gram Panchayat. They are the key people who can, after sensitization, mobilize the community for TB care and control and make allocations for TB patients’ nutrition and travel requirements.
- Yuva mandal/Mahila mandals (Youth/women’s clubs) - Community-level federations of young boys/girls/women, sometimes even comprising several women SHGs.
- Self-help groups (SHG) - An SHG is a group of individuals with a homogenous social and economic background, who voluntarily come together to regularly save small amounts of money and contribute to a local fund to meet the members’ emergency needs on a mutual help basis. These groups collectively manage their payments and ensure proper use of credits. Many NGOs currently engaged in the project are involved in formation/registration of these SHGs. It would be advisable to involve these NGOs for ease of implementation.
- Community-based organizations (CBO) - A CBO is a small group of people from a community, who come together for a particular purpose. It may be a local association of people mobilized around water conservation, mother and childcare, sustainable agriculture, education, or adolescent health; a group of social service persons; or any other such active group in a village.
Resource:
Assessment:
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Community mobilization strategies in rural areas includes empowering key decision-makers, people affected by TB, and marginalized and vulnerable populations.
True
False
1
This leads to raising awareness of services available and general health literacy surrounding TB.
More people accessing public health services will lead to better utilization of services.
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
-
CHO-CH26: Community Engagement
FullscreenCommunity Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
-
CHO-CH27: Social Inclusion and wellness activities
FullscreenSocio economic factors affecting TB patients
ContentSocio-economic factors affecting TB patients are:
1. General socioeconomic conditions of the society, culture and environment. This includes:
-
Gross Domestic Product (GDP)
-
Immigration
-
Urbanisation
-
Incidence of TB in the country
-
Labour policy
-
Access to healthcare
2. Socioeconomic position of the individual. This includes:
-
Income
-
Education
-
Occupation
-
Social class/ caste
-
Indigenous/ tribal population
-
Gender
3. Living and working conditions. This includes:
-
Housing conditions (overcrowding and poor ventilation especially in night shelters, de-addiction centres, old age homes, prisons)
-
Employment conditions - Occupation with risk of developing TB (mines, coal industry, sand blasting industries, weaving & glass industries, stone-crushers, cotton mill workers, tea garden workers, rice mill workers, etc.,)
-
Homelessness
-
Hard to reach areas
-
Urban slums
3. Psychosocial risk factors, such as:
-
Social exclusion
-
Depression
4. Individual lifestyle risk factors, such as:
-
Smoking
-
Alcohol abuse
-
Tobbaco use
-
Drug abuse
-
Nutrition (malnutrition)
-
Co-morbidities like diabetes mellitus, malignancies, patients on dialysis and on long term immunosuppressant therapy HIV, past history of TB
Resources
- NTEP Training Modules (1 to 4) for Programme Managers & Medical Officers, CTD, 2020.
- Social Determinants of Tuberculosis Context Framework and the Way Forward to Ending TB in India, IPH, India, 2020.
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Socio-economic factors affecting TB patients are:
-
Housing
-
Income
-
Access to healthcare
-
Alcohol abuse
1,2
2,3,4
1,2,3,4
1,2,4
3
TB is one of the few diseases which reflects and expresses social inequalities. Living conditions, economic conditions, lifestyle, and access, affordability, and availability of healthcare are factors which affect TB patients.
-
Stigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Rehabilitation service to TB patients
ContentThe holistic management of Tuberculosis (TB) patients can improve their life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
Table: Rehabilitation services for TB patients Rehabilitation Services for TB Patients Care Providers Key Components Nutritional Rehabilitation 1. Senior Treatment Supervisor
2. TB Health Visitors
3. Accredited Social Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at Peripheral Health Centre (PHC), Community Health Centre (CHC) level
-
Supporting nutritional needs of TB patients through Ni-kshay Poshan Yojana
-
Management of undernutrition in nutrition rehabilitation centres (NRCs)
-
Linkages for extra nutritional support for TB patients like the public distribution system (PDS) or food security act.
Pulmonary Rehabilitation
1.Physiotherapists (preferable one male and one female)
2. Nurses
3. Attendant
Management of physical and psychological impairment due to the disease to lower the handicap. Physical Rehabilitation -
therapists (preferable one male and one female)
-
Nurse Doctors
-
Surgeons
-
Physio
-
Attendant
-
Management of post-treatment sequelae by early identification and periodic assessment.
-
Comorbidity management
Social Rehabilitation 1. TB Health Visitors
2. Accredited Social
3. Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at PHC, CHC level
7. Ni-kshay Mitra
-
Linkage for vocational rehabilitation e.g., Skill India
-
Synergy between social welfare support systems like:
-
Rashtriya Swasthya Bima Yojana (RSBY)
-
TB pension schemes
-
National rural employment guarantee scheme
-
National Health Protection Scheme (NHPS) for palliative care and rehabilitation
Mental Rehabilitation 1. Psychiatrist
2. Psychologists / Counsellors
3. TB Health Visitors
4. Accredited Social
5. Health Activists (ASHAs)
6. Auxiliary Nurse Midwife (ANM)
7. TB treatment supporter
8. Medical officers at PHC, CHC level
-
Psychological counselling to the patient and caregivers.
-
Assisting patients in the planning of decisions related to the end-of-life stage.
Patient rehabilitation is ensured by:
-
1. IT-based monitoring via Ni-kshay platform
-
2. Community-based monitoring
-
3. Surveillance: A comprehensive surveillance system for TB patients and their providers built into eNikshay. This is supported by a call centre for user-friendly private reporting and patient monitoring.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Rehabilitation services to TB patients comprise Nutritional, Physical, Pulmonary, Social and Mental Rehabilitation.
False
True
2
The holistic management of tuberculosis (TB) patients can improve life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
-
-
Fullscreen