-
DR-TB HIV Coordinator: TB & TB Epidemiology
FullscreenTuberculosis
Content
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Pathogenesis of TB
ContentTuberculosis (TB) is an infectious, chronic, granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the body.
The pathogenesis of TB in a previously unexposed immunocompetent individual is centred on the development of cell-mediated immunity. This confers resistance to the organism and results in the development of tissue hypersensitivity to tubercular antigens.
The pathologic features of TB, such as caseating granulomas and cavitation, result from the destructive tissue hypersensitivity that is part and parcel of the host immune response.
The sequence of events from inhalation of the infectious droplets to the containment of the primary focus of infection is as follows:

Figure: Pathogenesis of Tuberculosis
In many individuals, the stage 5 response (from above) halts the infection before significant tissue destruction or illness occur (Latent TB Infection). In other individuals with immune deficits due to age or immunosuppression, the infection progresses to stage 5, and the ongoing immune response results in caseation necrosis (Active TB Disease). The figure above provides more details on the progression of TB disease.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Epidemiological Triad of TB
ContentThe Epidemiologic Triad is a model used in the field of epidemiology to study diseases and how they are spread. It consists of a triangle with three vertices or corners.
The three vertices for infectious diseases consist of:
1. Agent, or microbe that is the factor causing the disease.
2. Host, or organism harbouring the disease.
3. Environment, or those external factors that cause or allow disease transmission.
In the Epidemiological Triad of TB (Figure), the agent is the TB causing bacteria Mycobacterium tuberculosis; the host refers to humans that are susceptible to TB. Susceptibility or the risk factors for acquiring TB can be:
- Close contact with a person having TB disease
- Nutritional status of the host
- Existing co-morbidities
- Low immunity.
Susceptibility of the host can also vary due to age, gender, genetic composition, race, ethnicity, etc.
As TB is an airborne disease, environmental factors come into play for the transmission of TB. These include crowding, poor ventilation, bad sanitation, indoor air pollution, etc.
The understanding between the interplay of agent, host and environment is essential to understanding the epidemiology of TB and taking measures to control it. The risk of TB due to environmental factors can be reduced by practising airborne infection prevention measures like good ventilation, hand hygiene and cough etiquette.

Figure: Epidemiological Triad of TB
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The three vertices of the Epidemiological Triad are agent, host and environment.
TRUE FALSE 1 The three vertices of the Epidemiological Triad are agent, host and environment.
Yes Yes Agent in TB
ContentMycobacterium tuberculosis (M. tuberculosis) belonging to the family Mycobacteriaceae cause Tuberculosis (TB).
These are rod shaped bacilli and require oxygen to survive (aerobic bacteria).
The following characteristics of these bacilli help them to survive in human body for a long time and resist the action of drugs:
- Slow growing bacteria (replicates every 12-24 hours)
- Tough, hydrophobic cell wall rich in mycolic acid that resists action of many drugs including antibiotics.
- Ability to remain in dormant stage inside host tissues for many years in conditions with limited oxygen and nutrition (facultative anaerobes). They can revert to active state when favourable conditions (reduced host immune response, undernutrition etc.) ensue. The persistence of the bacteria in the host tissue for long duration of time is responsible for prolonged incubation period and re-activation of infection.
- The multiple mechanisms of drug resistance by the bacteria give rise to multi-drug resistant and extensively drug-resistant tuberculosis.
These characteristics make tuberculosis a chronic granulomatous disease that requires special antibiotics for treatment.
Resources
- Antimicrobial Resistance in Mycobacterium tuberculosis: Mechanistic and Evolutionary Perspectives, FEMS Microbiology Reviews, May 2017.
- The Biology of Mycobacterium tuberculosis Infection, Mediterranean Journal of Hematology and Infectious Diseases, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation PageID Part of pre-test Part of post test M. tuberculosis bacilli can survive conditions with limited oxygen. This means they are: Strict aerobes Strict anaerobes Facultative anaerobes None of the above 3 M. tuberculosis requires oxygen. However, they can survive in limited oxygen conditions also and can enter a dormant stage. They revert to active state when favourable conditions ensue. Thus, they are facultative anaerobes. Yes Yes Host factors in TB
ContentHost factors in TB disease are various factors/attributes of the host(person who is developing TB disease/infection).
The various host factors are as follows:
- Age: TB can affect people of any age. Young adults (15-30 years of age) are seen to have high rates of disease in India. Children and the elderly are also high-risk groups for the contraction of the disease.
- Gender: TB affects all genders, but males have higher disease rates, probably owing to higher levels of exposure to the bacteria in occupational settings.
- Immunity status: Individuals with compromised immunity status, like those on corticosteroid therapy/ immunosuppressants after organ transplant, HIV infection, diabetes mellitus etc., are more prone to TB infection and disease.
- Nutritional status: Undernutrition causes weakening of the immune system and hence predisposes to TB. Risk of TB increases by about 14% with each unit reduction in Body Mass Index (BMI).
- Previous TB infection: Individuals who are close/ household contacts of confirmed pulmonary TB patients; individuals residing in TB high-prevalence regions; high-risk groups like healthcare workers, homeless people, HIV infected etc., have high chances of being already infected with TB and hence, would progress to disease.
Resources
- India TB Report 2021, Central TB Division, MoHFW, Government of India.
- TB Risk Factors, Centers for Disease Control and Prevention.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Pick the correct statement for the causation of TB disease. Undernutrition causes TB disease. HIV infection compromises the immune system and may lead to TB disease. Children do not develop TB disease. The elderly are not at high risk for developing TB disease. 2 - HIV infection weakens the immune system of an individual and predisposes him/her to TB infection and disease.
- Undernutrition, as such, is not a causative factor for TB, but it weakens the immune system and predisposes to the infection/ disease.
- Children and the elderly are at high risk for TB.
Yes Yes Environmental influences in TB
ContentEnvironmental conditions have a huge role in the development of TB disease and are an important component of the epidemiological triad for TB disease.
The various environmental factors influencing TB are:
- Poor housing and ventilation: Damp homes, often resulting from condensation due to inadequate ventilation, allow the growth of mold, fungi, and other microorganisms. This adversely affects the respiratory health of individuals and increases the chances of the spread of TB from a patient to his/her household contacts.
- Overcrowding: More people living within a single space restricts movement, gives scope for lack of privacy and limits hygiene. The extent and persistence of contact with an infected person increases. The droplet nuclei (due to coughing) from infected individuals can stay in the air for a long time and transmit the disease easily to contacts.
- Indoor air pollution: The use of traditional biomass fuels like cow dung, wood etc. for energy generation (especially for cooking) in poorly ventilated households pose serious risks to the lung health of individuals. Damaged lungs are more susceptible to TB infection/ disease.
- Occupational environment: Healthcare workers, miners etc. are at a high risk of TB. Inadequate air change rates, negative airflow and recirculation of air have been identified as occupational hazards in hospitals with respect to TB transmission.
Resources
- Role of Environmental Factors in Transmission of Tuberculosis, Dynamics of Human Health, 2015.
- Housing and Public Health, Annual Review of Public Health, 2004.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How does poor housing contribute to TB transmission?
Poor ventilation measures
Increased dampness in the ambient air
Indoor air pollution
All of the above
4
Poor housing usually arises as a result of poverty, wherein the nutritional status and hence immunity of inhabitants are already low, which predisposes them to TB. Adding to it, structural faults like poor ventilation, the resultant increase in droplets in the air and poor smoke escape from the burning of solid fuels also contribute to TB transmission.
Yes Yes TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Natural History of TB
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
Development of Drug Resistance in Mtb.
ContentDrug resistance in Mycobacterium tuberculosis occurs when there is acquisition of mutations in genes that code for anti-TB drug targets or drug-activating enzymes.
Drug resistance in Tuberculosis (TB) occurs through two main mechanisms shown in the figure below.
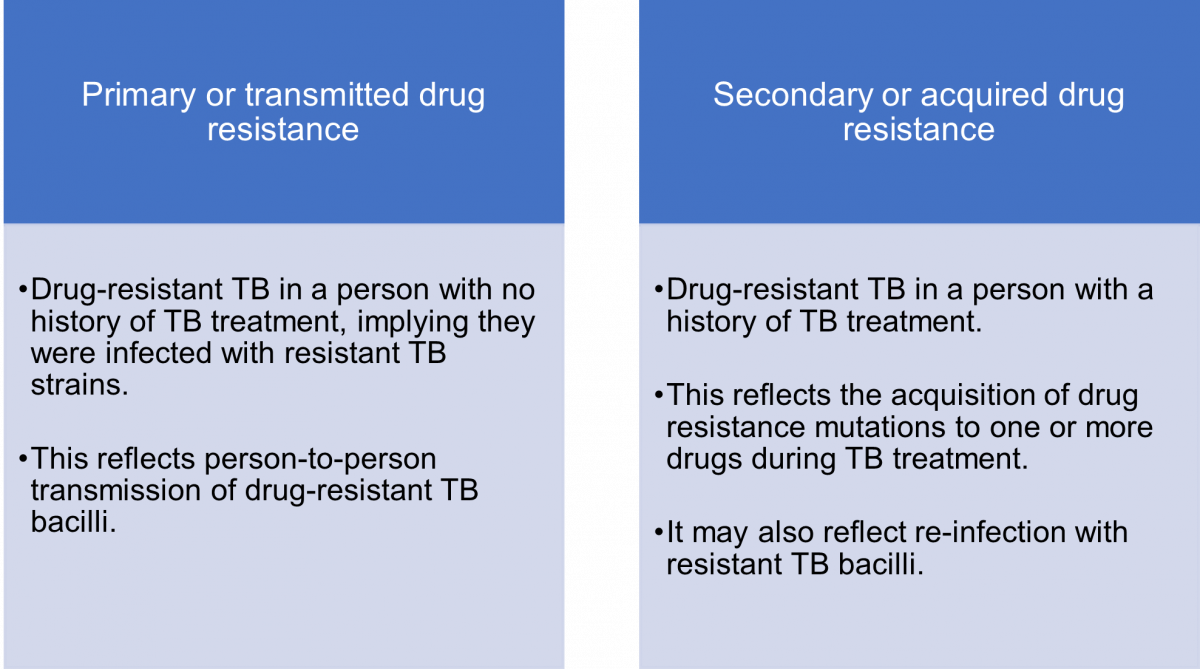
Figure: Mechanisms or Types of Drug Resistance in TB
The mechanism of transmission of drug-resistant (DR) and drug-sensitive (DS) TB is the same i.e., via infectious aerosols.
Acquired drug resistance is multi-factorial, and may be due to:
- Lack of access to quality-assured anti-TB drugs for proper treatment
- Lack of adherence to the regimen or interrupted therapy which could be due to complex dosing strategies, serious adverse drug reactions and drug–drug interactions
- Inappropriate regimens
- Sub-therapeutic dosing
- Use of expired or substandard anti-TB drugs
- Malabsorption of oral anti-TB drugs which can be seen, for example, in HIV patients.
Resources
- Navisha Dookie et al. Evolution of Drug Resistance in Mycobacterium tuberculosis: A Review on the Molecular Determinants of Resistance and Implications for Personalized Care, Journal of Antimicrobial Chemotherapy, Volume 73, Issue 5, May 2018.
- Bento J, Duarte R, Brito MC, et al. Malabsorption of Antimycobacterial Drugs as a Cause of Treatment Failure in Tuberculosis, BMJ, September 2010.
- Biadglegne F, Sack U, Rodloff A. Multidrug-resistant Tuberculosis in Ethiopia: Efforts to Expand Diagnostic Services, Treatment and Care. Antimicrobial Resistance Infection Control, 2014.
Causes for Drug-resistant Tuberculosis
ContentDrug resistance is caused by a genetic mutation that makes the drug ineffective against the mutant bacilli.
The causes of drug-resistant TB can be enumerated as follows:
1. Providers/ Programme Related Causes:
- Inadequate or poorly administered TB treatment regimen
- Unavailability or poor quality of anti-TB drugs
- Poor monitoring of TB treatment
- Delay in detection and management of DR-TB
2. TB Patient/ Host Related Causes:
- Clinical characteristics of TB patients leading to suboptimal drug levels in blood (e.g. Malabsorption syndrome)
- Irregular anti-TB treatment due to any reason (e.g. socio-economic barriers, substance abuse, Adverse Drug Reactions (ADRs), psychological and other factors)
There are two principal causal pathways leading to the development of drug-resistant TB:
- Primary drug resistance: It means that a person has been infected with a drug-resistant TB strain.
-
Acquired (Secondary) drug resistance: It is the result of inadequate, incomplete or poor treatment quality that allows the selection of mutant resistant strains.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Chemotherapy and its implication in TB control
ContentChemotherapy for TB is the use of an anti-TB drugs to kill, or prevent the replication of, TB mycobacteria in the patient’s body. Effective anti-TB chemotherapy renders the patient non-contagious and cures the patient, thereby interrupting the chain of transmission. Mortality rates of TB range from 50-80% in untreated smear-positive individuals and drop to lower than 5% under chemotherapy.
Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment. TB disease must be treated for at least 6 months and in some cases even longer. The use of multi-drug therapy reduces the incidence of drug-resistant cases and increases the overall effectiveness of treatment.
If treatment is interrupted, any surviving bacteria may cause the patient to later become ill and infectious again, potentially with drug-resistant disease.
How infectious are tuberculosis patients under chemotherapy?
Under effective chemotherapy, there is a substantial decline in infectiousness in two weeks time, and may not be a major source of risk to any contacts. This decline is indicated by the rapid fall in the number of viable organisms in the sputum, and reduced frequency of coughing.
Types of Chemotherapy in TB
- Preventive Chemotherapy: Regimen for healthy but TB infected persons with a high risk of developing TB, in order to prevent them from developing TB.
- Standard Chemotherapy: Two-phased chemotherapy for an average of 6-8 months based on the combination of at least four major drugs (HRZE) given for 2 months during the initial intensive phase of treatment and followed by a combination of at least 2 drugs given for at least 4 months during the continuation phase of treatment.
- Chemotherapy for Drug-resistant TB: Two-phased chemotherapy varying from 9 - 24 months in patients having demonstrated resistance to drugs used in standard chemotherapy. The regimen varies with the drug to which the resistance is present, however, each regimen contains a mix of second-line anti-TB drugs including injectables.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Infectiousness and Host Susceptibility, The Journal of Infectious Diseases, Vol. 216, suppl_6, 2017.
- Tuberculosis chemotherapy: Current Drug Delivery Approaches, Respiratory Research 7, Article no. 118, 2006.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which type of chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB? First-line anti-TB drugs Preventive Chemotherapy Standard Chemotherapy Chemotherapy for Drug Resistant-TB 2 Preventive chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB. Yes Yes Incidence of TB Disease
ContentIncidence is an epidemiological measure of the occurrence of new cases of a disease in a population over a specified period of time. Tuberculosis (TB) incidence is the number of new cases of active TB disease during a certain time period (usually a year), and is better expressed as a rate, as shown in the figure below.


Figure: Deriving the Incidence of TB Disease for a Given Population
Tuberculosis incidence varies considerably in different populations and population segments.
In 2021, the Global TB incidence was 134 (125-143) per 100,000. The TB Incidence rate of India is - 210 (178-244) per 100,000 in 2021 according to WHO Global TB Report 2022.
Resources
- India TB Report, 2022.
- Epidemiologic Basis of Tuberculosis Control, Hans L. Rieder, 1999.
- Morbidity Frequency Measures, Centers for Disease Control and Prevention.
- Global Tuberculosis Report 2022.
Prevalence of TB Disease
ContentPrevalence is an epidemiological measure of the proportion of a population with a disease or a particular health condition at a specific point in time (point prevalence) or over a specified period of time (period prevalence).
Tuberculosis (TB) prevalence refers to the number of people with TB that are present in a particular population at a given time. Calculation of the TB prevalence rate is shown in the figure below.

Figure: Deriving the Prevalence of TB Disease for a Given Population
TB prevalence rate is derived by adding the number of persons that develop new TB disease (i.e., incident cases) and those who already have the disease (i.e., existing cases), and dividing the sum by the total population from which the cases arose.
TB prevalence varies widely and is affected by a number of factors such as age, gender, population density, rural/urban settings, as well as socioeconomic factors.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
TB Notification rate
ContentTB notification rate is the number of TB cases notified over a specified time period for a specified population, usually per lakh. It indicates how many cases have been diagnosed and informed to the National TB Elimination Program.
It is mostly calculated annually, and the calculation formula is as follows:

Figure: Deriving the Annualized TB Case Notification Rate
The National TB Elimination Program calculates TB notification rates based on TB cases notified using the digital surveillance system called Nikshay. Each state/district is provided with an annual target for TB case notification, the progress of which is measured periodically to understand efforts taken for the detection of TB cases.
Example
If the number of TB patients diagnosed in District X one year is 1000, and the mid-year population of District X is 10,00,000, then the annualized TB case notification rate is calculated as follows:
100 cases/100 000/year
Resources
TB deaths
ContentWhen an HIV-positive person dies from TB, the underlying cause is classified as HIV with TB as a contributory cause. However, the milestones and targets for reductions in TB deaths set at the End TB Strategy are for the combined total of deaths in HIV-positive and HIV-negative people.
Estimates of TB deaths in India:
Estimates of TB burden, 2020 Number (Rate per 100 000 population) HIV-negative TB mortality 493 000 (453 000-536 000) 36 (33-39) HIV-positive TB mortality 11 000 (9 800-12 000) 0.78 (0.71-0.84) In 2020, India accounted for 38% of global TB deaths among HIV-negative people, and for 34% of the combined total number of TB deaths in HIV-negative and HIV-positive people.
Note: The International Classification of Diseases (ICD) defines TB deaths as ‘death from TB among HIV-negative people'.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the definition of TB mortality rate?
Number of TB deaths per one thousand population per month
Number of TB deaths per 10 thousand population per year
Number of TB deaths per one lakh population per year
Number of TB deaths per one crore population per year
3
TB mortality rate is defined as the number of TB deaths per one lakh population per year.
Yes
Yes
-
DR-TB HIV Coordinator: NTEP
FullscreenEnd TB strategy
ContentThe World Health Organisation End TB Strategy, adopted by the World Health Assembly in 2014, aims to end the global TB epidemic. The strategy draws on the opportunities presented by the Sustainable Development Goals (SDGs), especially those goals aimed at achieving universal health coverage and social protection from disease.
The table given below provides information on the vision, goal, milestones and targets for the End TB Strategy.
Table: Details on the End TB Strategy; Source: The End TB Strategy, World Health Organisation, 2015, p2. Vision of the End TB Strategy A world free of TB:
- Zero TB deaths
- Zero TB disease cases
- Zero suffering due to TB
Goal of the End TB Strategy To end the global TB epidemic by 2035 End TB Milestones for 2025 - 75% reduction in tuberculosis deaths (compared with 2015)
- 50% reduction in tuberculosis incidence rate (less than 55 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
End TB Targets for 2035 - 95% reduction in tuberculosis deaths (compared with 2015)
- 90% reduction in tuberculosis incidence rate (less than 10 tuberculosis cases per 100 000 population)
- No affected families facing catastrophic costs due to tuberculosis
The National Strategic Plan (2017-2025) proposes bold strategies with commensurate resources to rapidly decline TB in the country by 2030 in line with the global End TB targets to attain the vision of a TB-free India.
Resources
- National Strategic Plan for Tuberculosis Elimination 2017–2025.
- The End TB Strategy, World Health Organisation, 2015.
Sustainable Development Goals [SDGs] related to TB
Content
Figure: Summary of the Sustainable Development Goals
- Goal 3 is related to Good Health and Well-being. It mentions that 'Each nation needs to ensure healthy lives and promote the well-being of all ages'.
- The United Nations Sustainable Development Goals (SDGs) include ending the TB epidemic by 2030 under Goal 3.
- Goal 3.3: By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.
India is a signatory of the United Nations Sustainable Development Goals and has targeted TB elimination by 2025, five years ahead of the SDG timeline.
Resources
Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes History of Programmatic Management of Drug Resistant TB in India
Content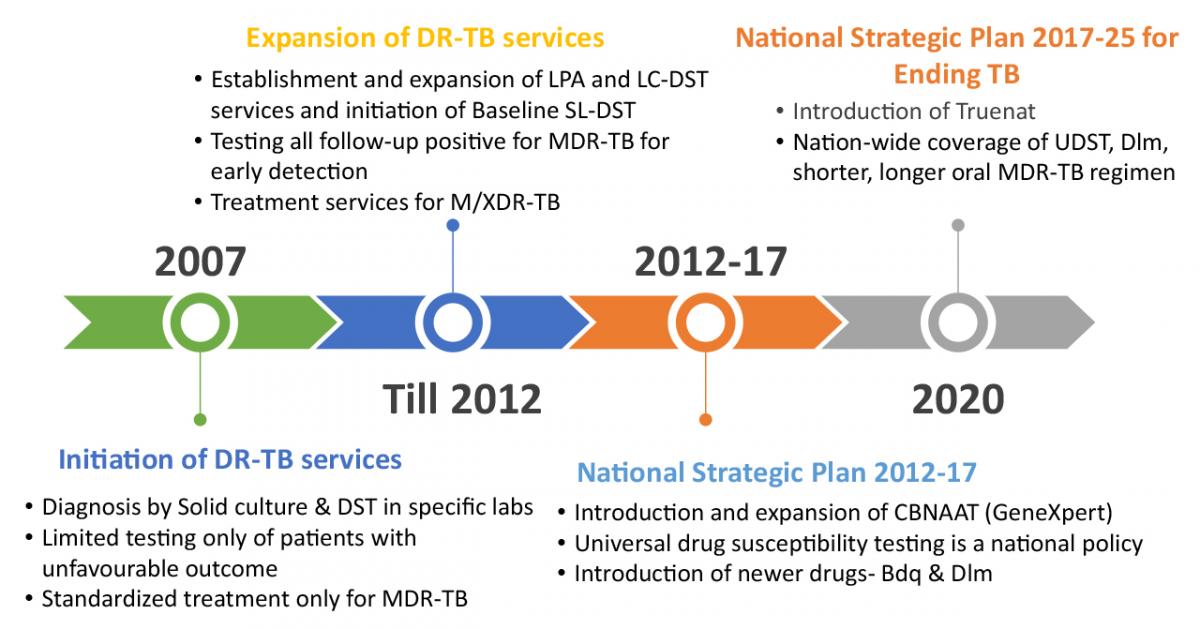
Figure 1: History of PMDT in India (2007 to 2020).; Source: Guidelines for PMDT in India, 2021 p.02
- Programmatic Management of Drug-resistant Tuberculosis (PMDT) services were rolled out in India in 2007.
- From 2007 to 2012, services were expanded in terms of diagnostic and treatment facilities.
- Country-wide geographical coverage of PMDT services was achieved in 2013.
- From 2012 to 2017, major policy shifts under PMDT were observed like introduction and expansion of Cartridge Based Nucleic Acid Amplification Test (CBNAAT), Universal Drug Susceptibility Testing (UDST), and introduction of newer drugs.
- In 2017 to 2020, introduction and expansion of Truenat till sub-district level, national-wise coverage of UDST, shorter and longer oral multi-drug resistant tuberculosis (MDR-TB) regimen were achieved.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
TB Arogya Saathi Application
ContentTB Aarogya Sathi empowers Citizens (including TB Patients under NTEP) and to serve as a Direct interface with the national TB program.
Citizen: The App is aimed at increasing awareness among the citizens. It is available for all Citizens using the App (no login required to access this content)
- Information on TB (Symptoms, Side Effects)
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Nutritional Advice
Patient: Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
- Patients registered under Nikshay get access to their TB health record additional information (after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code


Figure: TB Aarogya Sathi Application snapshot
Resources:
-
DR-TB HIV Coordinator: DR-TB Management under NTEP
FullscreenDR-TB Services and Functions of Stakeholders
ContentEach of the stakeholder plays important role in DR-TB service delivery and has specific responsibility which is being monitored.
The flow diagram below depicts the processes involved in the delivery of drug-resistant tuberculosis (DR-TB) services and specific functions of various stakeholders.
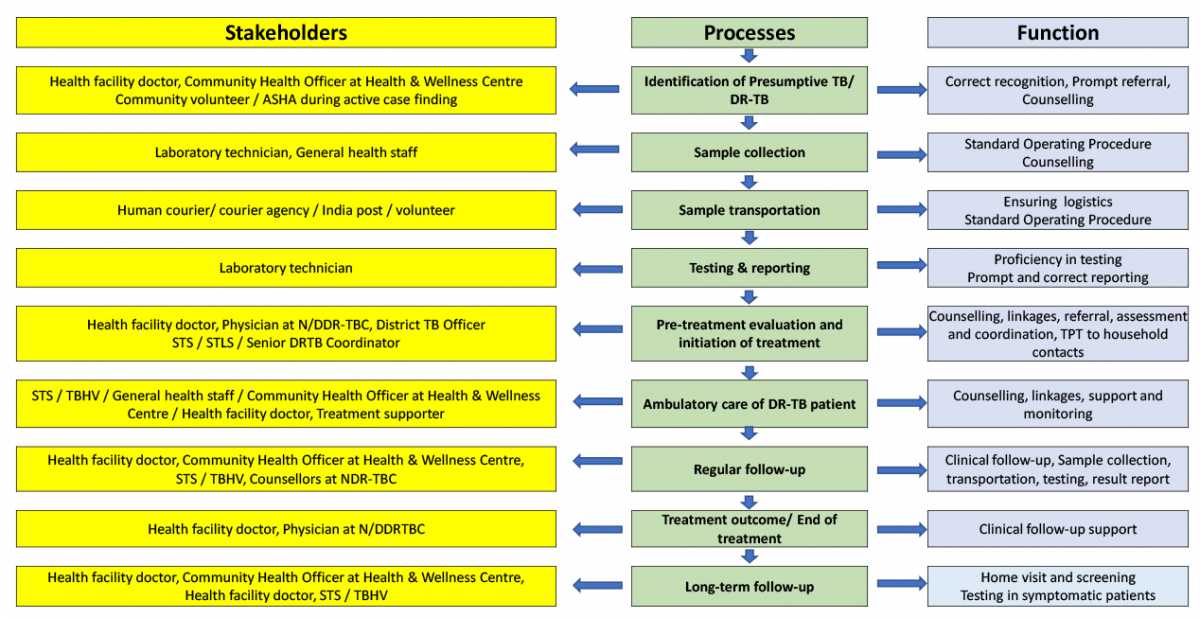
Figure 1: Cascade of DR-TB services and functions of various stakeholders
Source: Guidelines for PMDT in India, 2021, p.8
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
PMDT structure and roles
ContentThe National TB Elimination Programme (NTEP) in India has established well-organised Drug-resistant TB (DR-TB) management structures at the national, state and district level.
Image
Figure: Diagrammatic representation of the organisational structure of Programmatic Management of DR-TB (PMDT)
Abbr: NDR-TB: Nodal Drug-resistant TB; NAAT: Nucleic Acid Amplification Test; LPA: Line Probe Assay; CDST: Culture and Drug Sensitivity Test; DDR-TB: District DR-TB
The organisational structure and functions at different levels are described in the table below.
Level Organisational Structure Type of Organisation Function National-level Central TB Division (CTD), Ministry of Health and Family Welfare (MoHFW), Government of India (GoI) Administrative Providing resources/ devising policies/ issuing guidelines/ monitoring and evaluation/overall administration of the programme National Technical Expert Group Advisory Reviewing evidence Recommendation in guidelines National Reference Laboratory (NRL) Operational Providing laboratory-related expertise, External Quality Assurance (EQA) guidelines, Accreditations, a centre of excellence in diagnostics State-level State TB Cell, Health Department Administrative Providing resources, implementing guidelines, monitoring and evaluation/ overall administration of the programme State PMDT Committee Advisory Overseeing implementation as per guideline, taking strategic decisions, reviewing the progress in implementation and feedback/ suggestion to NTEP Nodal DR-TB Committee Advisory Guiding treatment of difficult to treat DR-TB cases, reviewing the progress of treatment and Adverse Drug Reaction (ADR) management, providing technical expertise for decisions at the State PMDT Committee, etc. Intermediate Reference Laboratory (IRL) Operational Providing laboratory-related services and expertise at the State level, EQA, and capacity building for diagnostic services Nodal DR-TB Centres Operational Providing treatment services to difficult-to-treat DR-TB cases, a centre of excellence in DR-TB treatment District-level District TB Cell Administrative Providing resources, implementing guidelines, monitoring and evaluation/ overall administration of the programme District TB Forum Advisory Overseeing implementation as per guideline, reviewing the progress in implementation, facilitating and monitoring the involvement of communities District Comorbidity Committee Advisory Review and rectify TB-comorbidity components with regard to HIV, diabetes, addiction and other review coordination with other health programmes like Rashtriya Bal Swasthya Karyakram (RBSK), Rashtriya Kishorethe Swasthya Karyakram (RKSK), Reproductive Maternal Newborn Child plus Adolescent Health (RMNCH+A) etc. District DR-TB Committee Advisory Guiding treatment of DR-TB cases, reviewing progress of treatment and ADR management, etc. NAAT/ LPA/ CDST Laboratories Operational Providing diagnostic services to detect DR-TB in the district (at more than one district) District DR-TB Centre Operational Providing treatment services to DR TB cases, ADR management etc. DR-TB services integration into the general health system
Block-level/ Ward-level Block Medical Officer/ Medical officer in office Operational Implementation of guidelines/ monitoring and evaluation of feedback Health facility-level Health facility doctor, Master in Public Health Skills (MPHS), Multipurpose Health Worker (MPHW), Accredited Social Health Activist (ASHA) Operational Implementation and review Health & Wellness Centre, Sub-Centre Community Health Officer (CHO) Operational TB screening and community intervention, coordination amongst various health programmes for TB-related activities Community ASHA, Panchayati Raj Institutions (PRI), Anganwadi Workers (AWW), other volunteers and community leaders Operational Implementation , community engagement through PRI, Village Health and Nutrition Day (VHND) , Community meetings, peer educators/TB champions/adolescent groups and Anganwadi sessions The organisational structure based on functional roles can be classified into diagnosis, treatment and drugs.
Diagnosis:
Name of Facility
Functions
Health Facility
- To identify presumptive cases/collect and transport specimen
- To communicate results to patients
- Collect and refer follow-up specimen
NAAT Site
- Diagnose TB and Rifampicin-resistant (RR) patients at district/ sub-district level
- Maintain records for Ni-kshay
- Transport the second sample to C&DST lab for First-line Line Probe Assay (FL-LPA) and Second-line Line probe Assay (SL-LPA)
C&DST Lab
- Receive diagnosis and follow-up samples
- Performs FL-LPA, SL-LPA, Liquid Culture (LC) and LC-DST
- Maintain records for Ni-kshay (LIMS)
- Provide rapid results to district , field and DR-TB centre
Treatment:
Name of Facility
Functions
Health Facility
- Identify treatment supporter
- To support and supervise DR-TB patients during treatment
- Manage Minor side effects
- Refer patients for treatment initiation
District DR-TB Centre
- Initiate DR-TB regimen
- Manage and record ADR
- Consult for complications
- Maintain records and Ni-kshay
- Coordinated with Nodal DR-TB centre/Field
- Monitor DR-TB treatment
Nodal DR-TB Centre
- Maintain ward and Airborne Infection Control (AIC)
- Undertake pretreatment evaluation and initiate treatment
- Manage major ADR
- Mentor and supervise concerned DDR-TBC
Drugs:
Name of Facility
Functions
District Drug
Store
- Coordinate test results.
- Refer patients to N/DDR-TBC
- Coordinate the drug flow from the district drug store to the field level
- Maintain records, Ni-kshay, monitor and supervision
State Drug Store
- Prepare and ship drug boxes to the district level
- Manage supply chain for diagnostics and drugs
- Maintain records in Ni-kshay Aushadhi
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page id Part of Pre-Test Part of Post-Test Which of the following is part of the PMDT structure under NTEP? NACP NACO District Comorbidity Committee None of the above 3 The district comorbidity committee is part of the PMDT district-level structure. The committee reviews and rectifies TB-comorbidity components with regard to HIV, diabetes, addiction and other review coordination with other health programmes like RBSK. Yes Yes The PMDT organisational structure is based on functional roles that can be classified into diagnosis, treatment and drugs. True False 1 The PMDT organisational structure is based on functional roles that can be classified into diagnosis, treatment and drugs. Yes Yes - To identify presumptive cases/collect and transport specimen
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Nodal DR-TB Centre
ContentNodal Drug-resistant Tuberculosis Centres (NDR-TBCs) are established to manage all forms of DR-TB, including complicated cases. Therefore, the centre should have:
- Advanced general laboratory
- Allied investigation facilities for Pre-treatment Evaluation (PTE)
- Intensive Care Unit (ICU)
- Ventilator backup
- In-house lab/ linkages for PTE laboratory tests
The NDR-TBC is established as per the need and is generally in a tertiary care setting where expertise and facilities for the management of DR-TB are available.
The figure below shows an overview of services offered at the NDR-TBC.
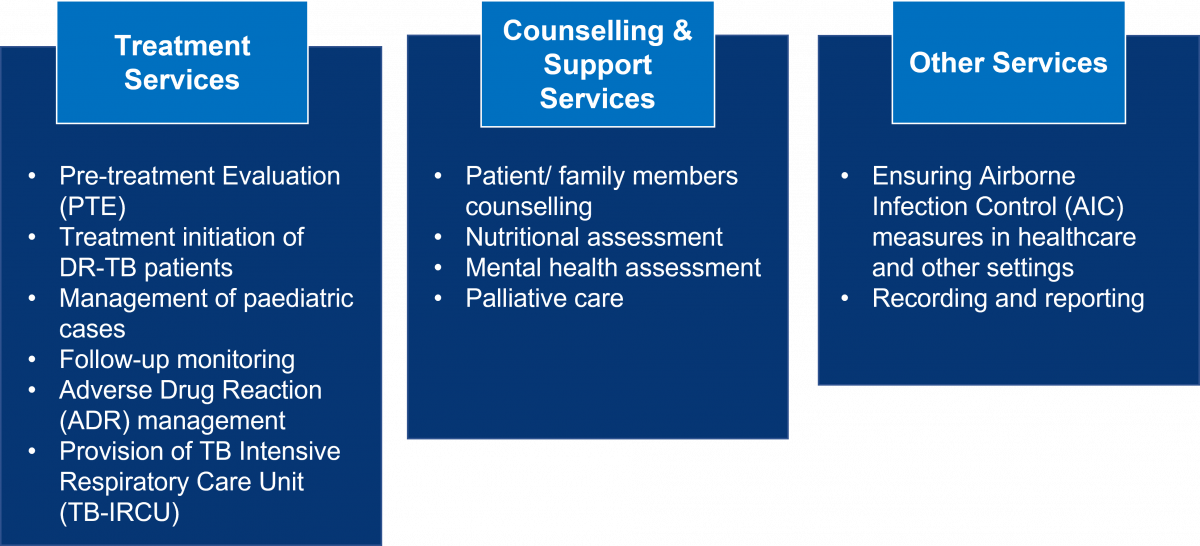
Figure: Range of Services Available at NDR-TBCs
District DR-TB Centres (DDR-TBCs) are linked with the NDR-TBC for the referral and management of complicated DR-TB patients like those who have:
- Additional resistance to second-line drugs, drug intolerance, serious adverse drug reactions, and contraindications
- Failing regimen, or patients returning after treatment interruption of more than 1 month
- The emergence of any exclusion criteria for a standard regimen for rifampicin-resistant TB or H mono/ poly DR-TB regimen
- Non-TB mycobacterial infections
- Need for palliative care or surgical interventions
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Requirements from Institutions for the Establishment of Nodal DR-TB Centre
ContentThe requirements from institutions for establishing Nodal Drug-resistant Tuberculosis Centres (NDR-TBCs) are as follows:
- It should preferably be a tertiary care institute.
- Separate wards for male and female patients (including children) should be available with at least 10 beds in each NDR-TBC.
- An outpatient clinic and a separate well-ventilated waiting area in an open-air, shaded area should be made available as per the Airborne Infection Control (AIC) guidelines.
- Administrative, environmental, and personal protective measures for airborne infection control should be placed in all indoor and outdoor facilities.
- All investigations under Pre-treatment Evaluation (PTE) and other Programmatic Management of Drug-resistant Tuberculosis (PMDT) services should be provided free of cost to the patient.
- Ancillary drugs should be provided for the management of Adverse Drug Reactions (ADRs) as per the NDR-TBC committee`s advice at no cost to patients.
- Oxygen and ventilators should be available for patients needing critical care support.
- The NDR-TBC committee should be formally established with the required set of experts as per the guidelines.
- All experts at NDR-TBC must be trained in the latest PMDT guidelines.
- Doctors, nursing and support staff should be available from the institute.
- Records and reports should be maintained for PMDT. Nikshay entries must be done on a real-time basis with regular electronic updates.
- Financial requirements must be availed through the institute/ state budgets or under National Health Mission (NHM).
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Mandatory Establishment of DR-TB Centres in All Medical Colleges
ContentIn view of the availability of expertise in medical colleges, there is a felt need to leverage their strength to improve clinical, Adverse Drug Reactions (ADRs) and comorbidity management of patients with Drug-resistant Tuberculosis (DR-TB) across India.
- Expansion of DR-TB services in the medical colleges will be helpful for enhancing the quality of care, treatment success and survival of these difficult-to-treat patients.
- National Medical Commission (NMC) issued a gazette notification in October 2020, mandating all medical colleges to establish a facility for the management of DR-TB by the time of 3rd renewal (admission of 4th batch of MBBS students).
- Private and Non-government Organisation (NGO) medical college hospitals are considered to serve as Nodal (N)/ District DR-TB Centre (DDR-TBC) at places where there is a need, either due to additional workload, non-availability of an appropriate public facility or preference of patients in the area.
- Terms and conditions for establishing that centre may be arrived at the local level as per the prevailing market rates in concurrence of the state/ district health society of the National Health Mission (NHM).
Resources
- Guidelines for Programmatic Management of Drug Resistant TB in India, 2021.
- Guidance Document of Partnerships, 2019.
- National Medical Commission, Gazette Notification, Government of India, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District DR-TB Centre
ContentDistrict Drug-resistant TB Centres (DDR-TBCs) are dedicated centres for providing DR-TB services for patients and can be established at the district or sub-district level.
- It may be established in institutes like medical colleges, district hospitals, TB hospitals and private or corporate institutes, trust hospitals or other sector hospitals, with the availability of required clinical expertise.
- There should be at least one DDR-TBC available in each district. However, more than one DDR-TBC can be established to improve the access and preference of patients to seek care.
- DDR-TBC can be established on an Outpatient Department (OPD) basis as well.
- Central TB Division (CTD) should be informed about the up-gradation of any institute to a DDR-TBC.
- Requirements for infrastructure and Human Resources (HR) may be proposed in the annual Programme Implementation Plan (PIP).
TB Services Available at the DDR-TB Centre
Pre-treatment Evaluation (PTE): Basic investigations required for initiating DR-TB regimens, examples include:
- Complete Blood Count (CBC)
- Thyroid-stimulating Hormone (TSH) tests
- Renal function tests
- Liver function tests
- Electrocardiogram, etc.
Treatment Services: Trained experts can initiate all DR-TB regimens at the DDR-TBC.
Resources
Functions of District DR-TB Centre
ContentThe following functions and package of services should be offered at each District Drug-resistant Tuberculosis Centre (DDR-TBC):

Figure: Functions of DDR-TBCs
Abbr: NDR-TBC: National Drug-resistant TB Centre; AIC: Airborne Infection Control
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Requirements for Establishing District DR-TB Centres
ContentThe following are requirements from institutions for establishing the district Drug-resistant Tuberculosis Centre (DDR-TBC):
Structural requirements:
- It should preferably be a secondary care institute.
- Separate wards for male and female patients (including children) should be available with at least two beds in each for DDR-TBC.
- An outpatient clinic and a separated well-ventilated waiting area in an open-air, shaded area to be made available as per the Airborne Infection Control (AIC) guidelines.
- Administrative, environmental and personal protective measures for airborne infection control should be placed in all indoor and outdoor facilities.
Infrastructure requirements:
- All investigations under Pre-treatment Evaluation (PTE) and other Programmatic Management of Drug-resistant Tuberculosis (PMDT) services should be provided free of cost to the patient.
- Availability of oxygen and ventilators for patients needing critical care support.
- Ancillary drugs must be provided for the management of Adverse Drug Reactions (ADRs) at no cost to patients, as per the DDR-TBC committee's advice.
Human resource requirements:
- The DDR-TBC committee should be formally established with the required set of experts as per guidelines.
- Services of specialists, if not available in the public facility, may be hired from the private sector under National Health Mission (NHM).
- All experts at DDR-TBC must be trained in the latest PMDT guidelines.
- Doctors, nursing and support staff should be available from the institute.
- Records and reports to be maintained for PMDT. Nikshay entries must be done on a real-time basis with regular electronic updates.
- Financial requirements should be availed through institute/ state budgets or under the NHM.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Nodal DR-TB Centre Committee
ContentThe Nodal Drug-resistant Tuberculosis Centre (NDR-TBC) committee is a clinical committee that is responsible for taking decisions regarding the management of DR-TB patients at the NDR-TBC.
The composition of the NDR-TBC committee is provided in the table below.
Table: Composition of the NDR-TBC Committee; Source: PMDT Guidelines for India, p205.
TITLE DESIGNATED OFFICIALS Chairperson Medical Superintendent or Director of the institute Vice-chairperson HoD Respiratory Medicine or General Medicine Nodal officer Senior Doctor from the department hosting the NDR-TBC Member secretary Senior Medical Officer- DR-TB centre Member HoD Microbiology or IRL Microbiologist Member HoD Psychiatry* Member HoD Ob&Gy* Member HoD ENT* Member HoD Dermatology* Member HoD Pharmacology Member Cardiologist* or Physician Member 1 Eminent Pulmonologist from NGO/ private sector Member WHO NTEP Consultant Member DTO of the district where NDR-TBC is located Special invitees DTOs of the districts linked (as and when needed) *To be consulted physically or virtually as and when required.
Abbr: HoD: Head of Department; IRL: Intermediate Reference Laboratory; Ob&Gy: Obstetrics and Gynaecology; ENT: Ear, Nose and Throat surgeon; NGO: Non-governmental Organisation, WHO: World Health Organisation, NTEP: National TB Elimination Programme, DTO: District TB Officer
Note: The chairperson can co-opt other specialists as required. The routine clinical decisions can be taken by the available doctor and informed to the NDR-TBC in subsequent meetings.
Functions of Nodal DR-TBC
- Periodically review the implementation status of PMDT in the respective nodal DR-TB centre to ensure that NTEP PMDT policies and guidelines are being followed.
- Coordinate with the IRL/ Culture and Drug Susceptibility Testing (C&DST) labs for Drug Susceptibility Testing (DST)/ Drug Resistance Testing (DRT) results and enter the details in Nikshay.
- Arrange for examination of DR-TB patients referred for their treatment eligibility, open treatment book and start PMDT regimen for all eligible patients.
- Admit DR-TB patients who may require the indoor facilities of the DR-TB centre.
- Arrange tele/ video consultation with relevant specialists on a case-to-case basis as well as with linked DDR-TBC to provide required clinical decision support.
- Empanel the private practitioners of various disciplines if the required specialist is not available in the public sector. In coordination with the respective State TB Officer (STO) and DTOs, ensure that drug ordering and distribution is managed in a timely and appropriate manner.
- Account for the review of record, report, Nikshay data entry.
- Monitor performance of DR-TB and PMDT in catchment geography using analysis of data from downloadable Nikshay reports and dashboard.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
District DR-TB Centre Committee Composition and Functions
ContentThe district drug-resistant tuberculosis centre (DDR-TBC) committee is a clinical committee where the dean/principal/ director of the institute is the chairperson.
- The Head of the Department (HoD) or a senior faculty member from the department of pulmonary medicine/general medicine is the nodal officer of the committee.
- The HoDs or senior faculty members of other specialties are the members of the committee.
- The clinical function of these committees must be adequately supported by the administrative or management committees of the institution in which district TB officer (DTO) is an ex-officio member.
- The composition of the DDR-TBC committee is shown in Figure 1.
Table 1: Composition of DDR-TBC committee; Source: Guidelines for PMDT, India 2021, p. 206 TITLE DESIGNATED OFFICIALS Chairperson Chief Medical Officer Co-chairperson Medical Superintendent/Director/Head of the institute Nodal person Physician in-charge of DDR-TBC Member Secretary DTO of the district Members Specialists* from pulmonologist, microbiologist, psychiatrist, Ob & Gy, cardiologist, ENT, dermatologist, pharmacologist etc. Member MO medical college, if placed Member Medical consultant (concerned), WHO NTEP TSN Member Any other invited member, if required *specialist available in-house, outsourced from private sector or linked with NDR-TBC Ob&Gy: Obstetrics and Gynaecology, ENT: Ear, nose and throat surgeon; MO: Medical Officer, WHO: World Health Organisation, NTEP: National TB Elimination Programme, TSN: Technical Support Network
Resources
District DR-TB Centre Committee: Terms of Reference [ToR]
ContentThe Terms of Reference (ToR) for the District DR-TB Centre (DDR-TBC) committee are:
- Ensure arrangements for patient treatment initiation as per the Programmatic Management of Drug-resistant Tuberculosis (PMDT) guidelines.
- Periodic review of treatment initiation, active Drug Safety Monitoring and Management (aDSM) and patient monitoring activities carried out at the DDR-TBC.
- Coordinate with the District TB Officer (DTO), TB Unit (TU), Health Facility (HF), other departments and Non-governmental Organisations (NGOs) to ensure the patient is linked with all essential services required.
- Empanel the private practitioners of various disciplines which are not available in the committee and are required for the management of DR-TB.
- Arrange tele/ video consultation with a relevant specialist on a case-to-case basis as well as with the linked nodal DR-TB centre to seek guidance required for clinical decision support. The DDR-TBC should also arrange tele/ video consultation with HFs on a case-to-case basis to provide required clinical decision support.
- Account for review of record, report, and Nikshay data entry.
- Monitor performance of DR-TB and PMDT in the catchment geography using analysis of data from downloadable Nikshay reports and dashboard.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Referral mechanisms for DR-TB services
ContentPresumptive Drug-resistant TB (DR-TB) is identified by the health facility doctor during passive screening or by health staff/ community volunteers during Active Case Finding (ACF).
Prompt referral and sample collection is an important step after identifying presumptive TB/ DR-TB.
After detection, referrals should be made promptly by the Community Health Officer (CHO) at Health and Wellness Centre (HWC)/ Senior Treatment Supervisor (STS)/ Tuberculosis Health Visitor (TBHV) to the health facility or Nodal/ District DR-TB Centre (N/DDR-TBC) for pre-treatment evaluation and treatment initiation. Every district has DDR-TBC for the treatment of DR-TB cases. However, for complicated DR-TB cases,that need either super-speciality or complex medical equipment and intensive care (like invasive ventilators), such patients are referred to Nodal DDR-TBCs.
Referral linkages for further domiciliary treatment are to be ensured by health facility doctor, N/DDR-TBC, senior DR-TB TB-HIV supervisor, STS, TBHV, CHO and general health staff.
Identification of suitable treatment supporters by CHO/ STS/ TBHV is essential, and the periodic follow-up of clinical/ bacteriological examination is to be managed.
The cascade of referral mechanism and function of various stakeholders is described below.
Image
Figure: Cascade of referral mechanism and function of various stakeholders; Source: Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, NTEP, CTD, WHO, MoHFW, 2021, p48.
Resources
Assessment
Question 1 Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page id Part of Pre-Test Part of Post-Test The patients are referred to N/DDR-TBC for pre-treatment evaluation. True False 1 After detection of DR-TB, referrals should be made promptly by the CHO at HWC/ STS/ TBHV to the health facility or N/DDR-TBC. Yes Yes Who ensures referral linkages for domiciliary treatment of patients? Senior DR-TB coordinator TB Health Visitor Community health officers All of the above 4 Referral linkages for domiciliary treatment are to be ensured by the health facility doctor, N/DDR-TBC, senior DR-TB coordinator, TB-HIV supervisor, STS, TBHV, CHO and general health staff. Yes Yes Difficult-to-Treat TB Clinic [DT3C]
ContentThe Difficult-to-treat TB clinic (DT3C) is an initiative to support Drug-resistant TB Centres (DR-TBCs) for better patient management.
The DT3C structure is intended to handhold and mentor District DR-TB centres (DDR-TBCs) for the effective management of Drug-resistant TB (DR-TB) cases.
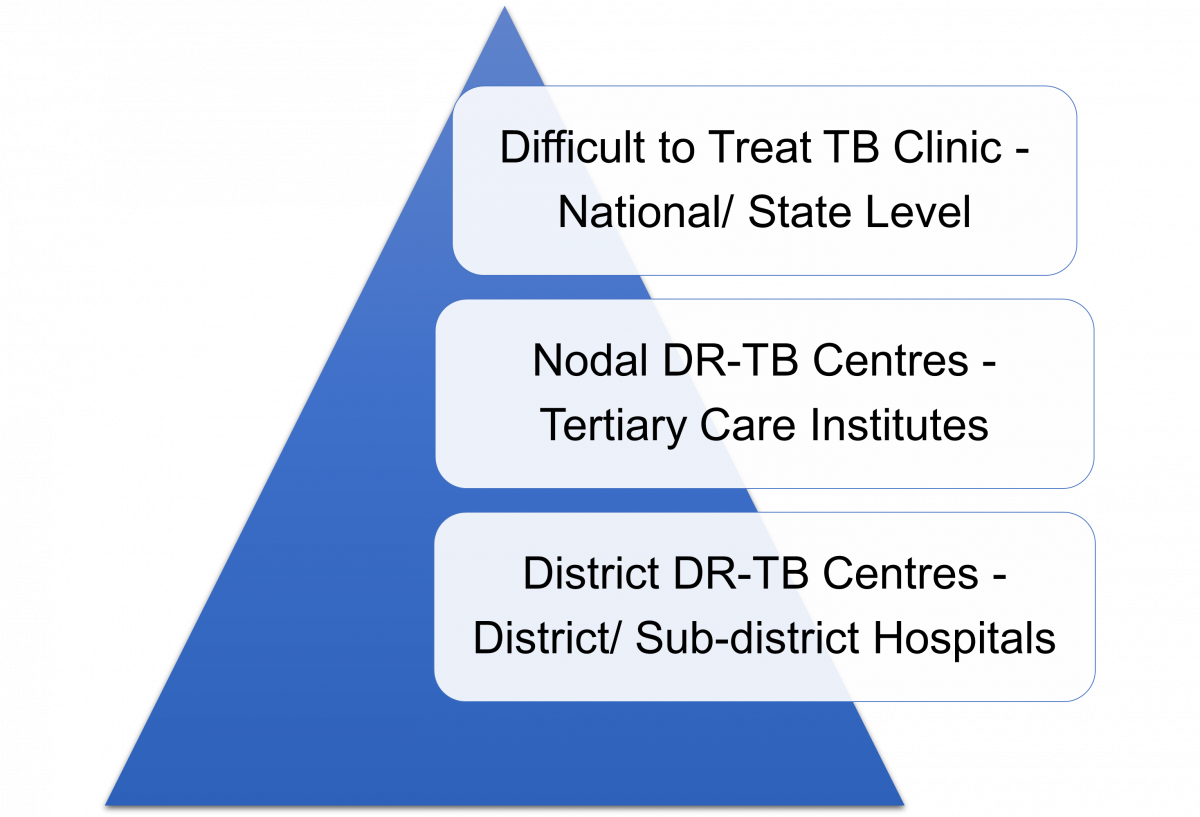
Figure: Difficult-to-treat TB Clinic: Three-tier Structure
The DT3C operates via a three-tier structure which is intended to improve the quality of DR-TB care:
- The DT3C is functional at the national level through the collaboration of the National Institute for Tuberculosis and Respiratory Diseases (NITRD), Central TB Division (CTD) and the National Task Force (NTF).
- Experts involving various specialties are included in the team as mentors at state-level D3TC.
- Information/ queries regarding the patient are shared in a standardized format by the DDR-TBC beforehand to facilitate discussions through the state nodal officer.
All states should have at least one (more than one in larger states) DT3C established.
Resources
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB HIV Coordinator and their role
ContentThe roles of the Drug-resistant TB (DR-TB) HIV Coordinator are:
1. Providing technical assistance to District TB Officer (DTO) for:
- Organising Programmatic Management of Drug-resistant TB (PMDT) services in the district
- Supporting District DR-TB Centre (DDR-TBC) for data management in Ni-kshay and their coordination with Anti-retroviral Therapy (ART) centre in the districts
- Organising TB-HIV coordination activities in the district
- Providing training to the staff of health facilities (public and private) under his/her jurisdiction to carry out PMDT and TB-comorbidity-related activities
- Conducting monthly reviews with TB Unit, National AIDS Control Programme (NACP), and Health and Wellness Centre (HWC) staff using dashboards and analysis of data from Ni-kshay periodically to address implementation and management gaps
- Activities related to drug and logistics supply chain management of drugs for PMDT, Cotrimoxazole Preventive Therapy (CPT) and Isoniazid Preventive Therapy (IPT) and modified TB regimen for People Living with HIV/AIDS (PLHA) with TB on second-line ART
- Coordinating regular sharing of the information related to TB-HIV coordination by assisting the nodal officer
- Mapping, prioritising, and engaging health facilities and laboratories in the private sector, Non-government Organisations (NGOs) and other sectors to improve access and quality of DR-TB care for all as per guidelines
- Preparing and maintaining a directory of Integrated Counselling and Testing Centres (ICTCs), ART centres/ Link ART Centres (LACs), community care centres, Non-communicable Disease (NCD) clinics, private health facilities and NGOs working for HIV, NCD in the district and the collaborating National TB ELimination Programme (NTEP) centres
- Providing a monthly activity report to the DDR-TBC committee and DTO.
2. Coordinating for smooth programme implementation
- Coordinate with all health staff and facilitate to subject all TB patients to universal Drug Susceptibility Testing (DST) at the linked decentralised Nucleic Acid Amplification (NAAT) sites and NTEP certified laboratories in the public and private sectors.
- Ensure that initial home visits are conducted by health workers to all newly diagnosed DR-TB patients of the district.
- Ensure that staff organises treatment support, all public health actions, follow-up reminders and transportation support for DR-TB patients.
- Help staff in proactive reach out to patients for follow-up cultures/ investigations as per schedule for every patient.
- Coordinate with and support TB Units, HWCs staff and private doctors to regularly update the directory of treatment supporters for DR-TB patients at the district level and facilitate their training.
- Facilitate the DR-TB treatment initiation at DDR-TBC.
- Ensure PMDT treatment books are updated for all patients at DDR-TBC, TB Units (TUs) and HWCs.
- Ensure and monitor the PMDT data completion in Ni-kshay and give periodic TU/ Peripheral Health Institute (PHI)-wise feedback to the DTO about the same.
- Liaise with respective Nodal Drug-resistant TB Centres (NDR-TBCs) for updating information on Ni-kshay and patient care.
- Ensure complete, correct and timely compilation and transmission of PMDT/ TB- HIV information.
- Establish linkages with the District TB Centre (DTC), District AIDS Prevention Control Unit (DAPCU), collaborating NGOs and hospitals of the district.
- Facilitate change management with respect to the use of Information, Communication and Technology (ICT) tools, Ni-kshay, Ni-kshay-Aushadhi for concerned data entry, validation & its use for public health action.
- Support DDR-TBC in updating the template with information to be shared with difficult-to-treat TB clinic for selected patients as per directions from the DDR-TBC committee and management of the patient based on recommended actions from the clinic.
3. Supervising and monitoring
- Monitor time to treatment of DR-TB patients and provide feedback on a periodic basis.
- Supervise all DR-TB patients and treatment support centres along with concerned TB Units, HWCs staff and private providers.
- Evaluate referral systems between ICTCs, ART centres, NCD, and NTEP and promote providing feedback to the referring centre.
- Field visits in the districts for at least 15 days a month, including Joint TB-Comorbidity visits on a tour programme approved by DTO.
4. Capacity building and imparting skills
- Train and supervise the pharmacists/ responsible staff of district/ TB Unit/ HWC drug stores in maintaining adequate stock of second-line drugs.
- Train staff for preparation of monthly patient-wise boxes by regimen and weight band as well as initialisation of Medication Event Reminder Monitor (MERM) devices, as available, for every patient initiated on DR-TB treatment at the NDR-TBC as per guidelines.
Resources
DO Letter - TOR and Needs Norms for NTEP Staff, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of pre-test
Part of post-test
DR-TB HIV coordinator should coordinate with all health staff and facilitate to subject all TB patients to universal DST.
True
False
1
DR-TB HIV coordinator should coordinate with all health staff and facilitate to subject all TB patients to universal DST at the linked decentralised NAAT sites and NTEP-certified laboratories in public and private sector treatment.
Interaction of DR-TB Coordinator with the TB Patient Care Ecosystem
ContentThe DR-TB HIV coordinator interacts with the TB patient care ecosystem as follows:
Patients: UDST at linked NAAT sites, treatment initiation, adherence monitoring and follow-up, ADR identification and management, contact tracing, linking with welfare schemes, linkage with the TB care ecosystem.
Treatment supporters: To ensure initial home visits, treatment support, and all public health actions.
STLS: To subject all TB patients to universal DST at the NAAT sites, to ensure complete DST and the laboratory follow-up of all the patients.
STS: Treatment initiation of DR-TB patients, necessary treatment support, Public health actions, and coordinate for follow-up cultures and investigations.
Medical officers: Facilitating DR-TB treatment initiation and management of ADR.
DR-TB Committee: Support DDR-TBC in providing the information about the DR-TB patients, and coordinate with the different staff to execute the decision of N/DDR-TBC. Updating the template with the information to be shared with difficult-to-treat TB clinic for supported patients.
Pharmacists/responsible staff of district/TB Unit/HWC drug stores: Maintaining adequate stock of second line drugs, preparation of monthly patient wise boxes by regimen and weight bands initialization of MERM devices.
Ni-kshay and Ni-kshayAushadhi: Use of ICT tools, Ni-kshay, Ni-kshay-Aushadhi for concerned data entry, validation and its use for public health action and monitoring the PMDT data completion in Ni-kshay and give periodic TU/PHI-wise feedback to the DTO about the same.
DTO/ Programme Managers: Seek overall guidance from DTO/Program managers for executing their duties and responsibilities. They also provide with necessary data and information about the PMDT facilitating supervision and monitoring and discuss and implement various solutions for the identified issues.
Resources
Assessment
Question 1
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of Pre-Test
Part of Post-Test
DR-TB HIV coordinator should coordinate with all health staff and facilitate subjecting all TB patients to universal DST.
True
False
1
DR-TB HIV coordinator should coordinate with all health staff and facilitate subjecting all TB patients to universal DST at the linked decentralised NAAT sites and NTEP-certified laboratories in public and private sector treatment.
Yes
Yes
-
DR-TB HIV Coordinator: Integration of NTEP with the Health System
FullscreenOrganisational Structure of Health System
ContentOverview of the organisational structure of the health system in relation to the National TB Elimination Programme (NTEP) is shown in the figure below.
Image
- Sub-centre: Most peripheral units under the public health system are designed to bring about behavioural change and provide preventive health care services.
- Primary Health Centre (PHC): First contact point between the village, community and the medical officer envisaged to provide integrated, curative and preventive health care.
- Community Health Centre/ Sub-district Hospitals: Serve as a referral centre for four PHCs and provides facilities for obstetric care and specialist consultations.
- Peripheral Health Institute (PHI): Most Peripheral Unit under the NTEP provides TB treatment and diagnostic services to the population.
- Tuberculosis Units: Nodal point for TB elimination activities in the sub-district level and are also responsible for stacking and supply of drugs to the PHI.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, CTD, MoHFW, India, 2020.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Where are Tuberculosis Units present under the NTEP? At the central level At the state level At the district level At the sub-district/ block level 4 Tuberculosis Units are present at the sub-district level under the NTEP. Yes Yes Need for integration of NTEP with Health System
Content-
The public health system in India through the National Health Mission (NHM) visualises the attainment of Universal Health Coverage (UHC) for all its citizens, which provides access to equitable, affordable and quality health care services, which is also accountable and responsive to the needs of the people.
-
Under the umbrella of NHM, the National TB Elimination Programme (NTEP) ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI).
-
Furthermore, the NHM, under the Ayushman Bharat initiative has taken measures to strengthen the primary care facilities including Primary Health Centres (PHCs) and Sub Health Centres (SHCs) in the Ayushman Bharat Health & Wellness Centres (AB-HWCs).
Need for integration of NTEP with the Health System at Different Levels
- Closer to community TB Services: The integration of TB services with the health system provides an opportunity for the TB programme to leverage the resources under the Ayushman Bharat initiative to take TB interventions closer to the community which were otherwise provided at the primary care level.
- Improved population coverage: Active empanelment and HWC database will help to monitor and identify the left-out population and contribute significantly to the NTEPs case finding activity coverage.
- Improved population health outcomes: Improved availability, access and utilisation of advanced TB treatment services under the ambit of UHC is essential in reducing morbidity and mortality from TB which may in turn also contribute to overall equitable health outcomes.
- Reduced out-of-pocket expenditure: The integration will improve the access to TB services, assure within-reach TB medicines and diagnostic services, provide linkages for care coordination with Medical Officers/ specialists across various levels of care, etc., all of which will reduce the catastrophic expenditures faced by the patients and their families.
- Decreased crowding at the secondary and tertiary health facilities: A strong network of peripheral level TB care services would facilitate in reduction of the overcrowding and the case burden at the secondary and tertiary facilities, which could be utilised for cases with follow-up referral to higher level facilities.
- Increased responsiveness and addressal of social determinants of TB: Provision of TB treatment at the nearest point of care for the communities and engaging the most peripheral workers from the health system like the Accredited Social Health Activists (ASHA) in the TB programme may lead to comfort in accessing the care by the patients and also enable addressing psycho-social determinants of TB.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, CTD, MoHFW, India, 2020.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). True False 1 Under the umbrella of NHM, the NTEP ensures the provision of free TB services (diagnostics and drugs) and management of TB as per the Standards for TB Care in India (STCI). Yes Yes -
National Health Mission [NHM]
ContentThe National Health Mission (NHM) was launched by the Government of India in 2013, subsuming the National Rural Health Mission (NRHM) and National Urban Health Mission (NUHM). Figure 1 shows the history of the NHM.
The vision of NHM is “Attainment of Universal Access to Equitable, Affordable and Quality health care services, accountable and responsive to people's needs, with effective intersectoral convergent action to address the wider social determinants of health.”
Image
Figure 1: History and Make-up of the NHM; Source: Annual Report 2015-16, Ministry of Health and Family Welfare (MoHFW)
NHM further aims to support the existing national programmes of health and family welfare (Figure 2) including reproductive and child health, malaria, blindness control, iodine deficiency, filariasis, kala-azar, tuberculosis (TB), leprosy, and integrated disease surveillance.
Image
Figure 2: Health Programs Supported by NHM NHM and the National Tuberculosis Elimination Program (NTEP)
Integrating the NTEP with the health system increases the effectiveness and efficiency of TB care and control. India's TB control programme has been mainstreamed efficiently with the NHM.
The overall responsibility for the financial management of the NTEP is with the MoHFW, Director General of Health Services (DGHS) through the NHM.
At the state level, the State Health Society or its equivalent under the NHM of the state manages the financing of the TB Control Programme.
At the sub-district level, the TB Unit (TU) is the nodal point for TB control activities. TUs are based mainly in NHM health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
Resources
Delivery of TB Care in Private Sector
ContentThe private sector for tuberculosis (TB) care is everything outside the ambit of government-run public health initiatives. It consists of a wide range of providers from individual medical practitioners of many different systems of medicine, including:
- Modern medicine
- Indian systems of medicine
- Homeopathy
- Paramedics
- Traditional healers
- Private hospitals and nursing homes
- Non-governmental organization-run hospitals
- Corporate sector health care institutions
As per the National Sample Survey Organization report of the 75th round, more than 70% of patients seek care in private clinics or hospitals.
Challenges with TB care in the private sector:
- Delays in diagnosis
- Over-diagnosis of TB due to an over-dependence on X-rays
- Use of multiple non-standard regimens for inappropriate durations
- Lack of a mechanism to ensure the full course of treatment and to record treatment outcomes
Regulatory tools to improve TB care services: The following are existing regulatory tools to improve TB care services in the private sector:
- Standards for TB care in India
- Mandatory TB notification on Nikshay
- Ban on sero-diagnostics
- Amendments in H1 schedule
Regulatory tools, however, are limited, and partnership is preferred.
Steps/approaches to strengthen private sector engagement:
Partnership approaches include:
- An expanded acceptance by National TB Elimination Program (NTEP) of internationally approved diagnostic and treatment protocols
- Reliance on market forces rather than normative exhortation, that is, engaging and prioritising health care providers that offer the highest market value
- Increased use of accreditation and contracting
Other NTEP initiatives include:
- Outreach to private laboratories
- Increased control of TB drugs
- Innovative use of information and communication technologies for TB notification and treatment adherence monitoring
NTEP has systematically mapped private healthcare providers (single and multispecialty hospitals), private laboratories and chemists in the Nikshay online portal through which these health facilities can notify TB patients.
Resources
- Training Modules (1-4) for Programme Managers & Medical Officers, 2020.
- Key Indicators of Social Consumption in India: Health, NSS 75th Round Report, Ministry of Statistics and Programme Implementation, 2019.
- JEET Brochure.
Kindly provide your valuable feedback on the page to the link provided HERE
NTEP Integration into Public Health System
ContentIntegrated patient-centred care and prevention are one of the pillars of the End TB strategy. This requires TB services to be made affordable and accessible by integrating them with the general health system.
In 2005, the National Rural Health Mission (NRHM) was established and was merged with the National Urban Health Mission (NUHM) in 2013, to form the National Health Mission (NHM).The National TB Elimination Programme (NTEP) is a flagship programme under the NHM and fund allocation to NTEP occurs through the NHM.
NTEP integrates with the public healthcare system at various levels as follows:
- Community level – Accredited Social Health Activists (ASHA)/ Community Health Volunteers (CHVs)/ Multipurpose Workers (MPWs)
- Ayushman Bharath Health and Wellness Centre - Sub Health Centre (ABHWC - SHC)
- Ayushman Bharath Health and Wellness Centre - Primary Health Centre (ABHWC - PHC)
- Community Health Centre (CHC)
- District/ Taluka hospital
- Medical Colleges
- Other health institutions in the public sector – ESI, railways, ports and the ministries of mines, steel, coal, etc.
Note: As far as NTEP is concerned, a Peripheral Health Institution (PHI) is a health facility headed by a Medical Officer
TB services are provided free of cost through the public health system.
Services provided include:
- Advocacy, Communication and Social Mobilisation (ACSM) and Information Education and Communication (IEC)
- Screening for TB – Active Case Finding (ACF), Passive Case Finding (PCF), Intensified Case finding (ICF)
- Diagnosis of TB and drug resistance – Designated Microscopy Centre (DMC) or TB diagnostic centres. Some of the PHIs themselves act as DMCs or Sputum Collection Centres
- Treatment for DS-TB and H Mono/Poly DR-TB through PHIs
- Treatment for DR-TB through District/Nodal DR-TB Centres
- Treatment Support through out treatment course
- Clinical follow-up and comorbidity management
- Referral services for those with Adverse Drug Reactions (ADRs)
- Screening for Tobacco and Alcohol addiction and linkage to de-addiction services
- TB preventive therapy
- Data management in Ni-kshay
References
- Technical and Operational Guidelines for Tuberculosis, 2016.
- National Strategic Plan 2017-2025 for TB Elimination in India, CTD.
- Detect-Treat-Prevent-Build: Strategy for TB Elimination in India by 2025, Indian J Community Med., 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these is included in the TB services available at sub- centre level?
Providing treatment support and follow-up of TB cases in the sub- centre area
Conducting ACSM and IEC activities
Refering TB symptomatics to the nearby DMC/ TDC
All of the above
4
Services at ABHWC – SHC level include:
- Conduct ACSM and IEC activities
- Conduct case-finding activities in the catchment area of the centre – Active/ Passive/ Intensified
- Refer TB symptomatics to the nearby DMC/ TDC
- Linkage of positive DS-TB cases to the nearest PHC for initiation of TB treatment
- Referral of DR-TB cases to the nearest Nodal DR-TB Centre for treatment
- Treatment support and follow-up of TB cases in the sub- centre area
- Liasoning with the STS and MOTC for TB control activities in the area
- Facilitates data entry in Ni-kshay.
Yes
Yes
Ayushman Bharat Health and Wellness Centres
ContentAyushman Bharat (AB) is an attempt to move from a selective approach to health care to deliver comprehensive range of services spanning from preventive, promotive, curative, rehabilitative and palliative care. AB-HWCs are envisaged to deliver expanded range services that go beyond maternal and child health care services to include care for non-communicable diseases, palliative and rehabilitative care, oral, eye and ear nose and throat care, mental health and first level care for emergencies and trauma, including free essential drugs and diagnostic services.
It has two components which are complementary to each other.
- Under its first component, 1,50,000 Health and Wellness Centres (HWCs) will be created to deliver Comprehensive Primary Health Care, which is universal and free to users, with a focus on wellness and the delivery of an expanded range of services closer to the community.
- The second component is the Pradhan Mantri Jan Arogya Yojana (PM-JAY) which provides health insurance cover of Rs. 5 lakhs per year to over 10 crore poor and vulnerable families for seeking secondary and tertiary care.
On 14th April 2018, the Honorable Prime Minister of India launched the first Health and Wellness Centre at Jangla, Bijapur, Chhattisgarh. Health Sub-Center (HSC), PHC (Primary Health Center) and Urban PHCs are currently being upgraded to reach a goal of 1.5 lakhs AB-HWC by 2022.
The National TB Elimination Program (NTEP) has also integrated TB services as part of the health and wellness center service delivery package.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres, MoHFW, 2021.
- Ayushman Bharat - Health and Wellness Centre Website, Government of India.
Kindly provide your valuable feedback on the page to the link provided HERE
Medical Colleges
ContentMedical colleges in the country are integrated with the National TB Elimination Programme (NTEP) to widen access and improve the quality of TB services. Medical colleges provide specialized services for seriously ill TB patients.
The integration of medical colleges in the program is in a structured task force mechanism at different levels:
- National
- Zonal
- State
One national and six zonal task forces have been formed under the programme along with task forces for all states. A core committee is also formed in each medical college. These task forces are created with defined roles and responsibilities for the effective involvement of medical colleges in the programme.

Core Committee
Every medical college will have core committees representing various hospital departments and NTEP nodal officers. These committees meet quarterly and review the implementation of the program in the medical college.
Functions of the core committee:
- They organise sensitisation workshops and training for faculty members, postgraduates, undergraduates, interns, paramedical staff, etc.
- Ensure that teachings on TB/ NTEP form part of the curriculum for all medical colleges.
- Coordinate between various departments so that patients get the services under one roof.
- Coordinate with the district TB programme.
Role of Medical College in NTEP
- Medical colleges coordinate with the district TB programme for participation in quality assurance, supervision, monitoring, review and evaluation.
- Operational research is one of the important activities of medical colleges.
- Every medical college should have TB detection facility and treatment support centres. These centres are equipped with trained additional human resources such as medical officers, laboratory technicians and TB health visitors.
- The National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients.
- Medical colleges undertake advocacy for the programme.
- Medical colleges also functions as peripheral health institutes (PHI), maintain TB notification registers and submit monthly PHI reports: They have Nikshay user access and need to enter TB-related data on a real-time basis.
Resources
RNTCP Technical and Operational Guidelines for Tuberculosis Control in India, 2016.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Every medical college should have a DR-TB facility? True False 1 National Medical Commission insists that all Medical Colleges should also have facilities to manage DR-TB patients. ICTC
ContentIntegrated Counselling and Testing Centre (ICTC) is a hub where HIV Counselling and Testing Services (HCTS) are offered to an individual of his/her own will or as suggested by a medical care provider.
Types of ICTC
1. Standalone ICTC (SA - ICTC)
2. Facility integrated ICTC (F - ICTC)
The SA-ICTC facility is a confirmatory facility and it should be located at an easily accessible place with proper signages to direct and guide people to the location.
The SA-ICTC facility should consist of at least two rooms, one for counselling and the other for testing.
ICTC Type
Location Staff Pattern Services Standalone ICTC - Government medical colleges under centre, state and corporation
- General hospital
- District hospital
- Sub-district hospital and
- Community health centre
- Health facilities under public sector undertakings - Private medical colleges - Public-private partnership facilities
- Mobile SA-ICTC
- Targeted intervention (TI) -based SA-ICTC
- Medical Officer in charge
- Counsellor- One counsellor is appointed on a contractual basis. An additional counsellor may be appointed if there are more than 500 counsellings in a month
- Lab Technician (LT) - One LT appointed on a contractual basis, with less than 10,000 annual test load, every additional 5,000 annual tests, one additional LT and a maximum of up to 3.
- Pre-test counselling and informed consent
- HIV testing and sharing of test results
- Post-test counselling & disclosure
- Early Infant Diagnosis (EID)
- Testing of sexual partner/ spouse
- Screening for Sexually Transmitted Infections (STI)/ Respiratory Tract Infection (RTI), TB and other co-infections
- Linkages to care and treatment and other health services
- Linkage to social welfare schemes
- Outreach activity
- Follow-up testing and counselling
- Follow up of discordant couple
- Act as a nodal point for coordination, supportive supervision, capacity building and supply chain management of all F-ICTC
ICTCs are aligned to the National TB Elimination Programme (NTEP) diagnostic facilities.
- All individuals attending the ICTC are screened for the four symptoms of fever, cough, night sweats, and weight loss.
- Presumptive TB cases are referred for TB diagnosis to TB Detection centres(TDCs).
- Link the referred individual to the NTEP centre by providing a linkage form in Triplicate.
- Provide them with a duly filled NTEP referral form for diagnosis to fast track.
- Line list of all the Presumptive TB should be maintained and should be reviewed with NTEP monthly to ensure that all the cases have undergone testing.
Resources
Assessment
Question Option 1 Option 2 Option 3 Option 4 Correct Answer Explanation Page ID Pre-test Post-test Which of the following statement about ICTC is false? TB screening is done for all individuals at ICTC. Standalone ICTC is an HIV confirmatory facility.
ICTC has a medical officer, a lab technician, and a counsellor. TB screening for HIV-positive cases is done at ICTC. 4 TB screening is done for all individuals at ICTC irrespective of their HIV status. F-ICTC
ContentFacility-integrated Integrated Counselling and Testing Centre (F-ICTC) takes HIV Counselling and Testing Services (HCTS ) closer to the people, increasing the uptake of services while reducing transportation costs and waiting times. F-ICTC s can be mobile or fixed.
Location Staff Pattern Services - 24-hour Primary Health Centres (PHCs)
- Private sector/ not-for-profit hospitals
- Private laboratories
- Public sector organisation-run hospitals or facilities
- In the NGO sector
- Existing staff of the institution is sensitised and trained to offer counselling and testing.
- The medical officer of the institution is in charge.
- Pre-test counselling and informed consent
- HIV screening
- Screening for Sexually Transmitted Infection (STI)/ Respiratory Tract Infection (RTI), TB and other co-infections
- Post-test counselling
- Linkages to Standalone ICTC (SA-ICTC) for confirmation of diagnosis and care and treatment
- Linkage to other health services
Proper signage should direct and guide people to reach the F- ICTC.
The health facility should earmark a suitable room to ensure privacy and confidentiality and with good cross-ventilation to prevent air-borne infection.
Any positive HIV results at F-ICTC are only provisional - The facility uses whole blood finger-prick test kits for HIV screening.
If found reactive on HIV screening, link the individual to the linked SA-ICTC for confirmation of HIV diagnosis and further necessary action, using the Linkage Form.
If found non-reactive on HIV screening, the laboratory report duly signed by the medical officer should be given to the individual during post-test counselling on the same day as the screening.
Verbal screening for the four symptom complex of TB is done for all the clients and appropriate referral to NTEP diagnostic facilities if indicated. The provisions for Presumptive TB testing is applicable for ICTCs too.
Resources
Assessment
Question Option 1 Option 2 Option 3 Option 4 Correct Answer Explanation Page id Pre-test Post-test Which of the following is a false statement related to F- ICTC? It can be a mobile F-ICTC or a fixed facility. It is an HIV confirmatory facility. No special staff recruitment for F-ICTC.
Verbal screening for TB symptoms is done here. 2 It's a screening facility. Those who tested positive are sent to SA-ICTC. ART Centre
ContentAnti-retroviral Therapy (ART) Centre is a facility to provide a comprehensive package of care, support and treatment services to persons living with HIV/AIDS (PLHIV).
Location Staff Pattern Services - Medical colleges
- District hospitals
- Non-profit charitable institutions providing care, support and treatment services to PLHIV
- Should ideally be located near Medicine OPD
- A minimum of 1000 square feet area for ART centre expecting on an average 500 patients on ART with an adequate number of rooms.
- Nodal officer
- Senior medical officer (postgraduate in medicine)
- Medical Officer (MBBS)
- Counsellors
- Staff nurse
- Data manager
- Lab technician
- Care coordinator
- Register and provide care, support and treatment services to all PLHIV and monitor patients in HIV care (Pre-ART) regularly
- Identify eligible PLHIV requiring ART and initiate them on ART in a timely manner as per the National AIDS Control Organisation (NACO) guidelines
- Provide ART & treatment of opportunistic infections to eligible PLHIV
- Provide Isoniazid (INH) prophylaxis for PLHIV for TB prevention
- Provide treatment adherence and counselling services before and during treatment to ensure drug adherence
- Counsel and educate PLHIV, caregivers, guardians and family members on nutritional requirements, hygiene, positive living and also on measures to prevent further transmission of infection
- Refer patients requiring specialised services (including admission) to other departments/ higher facilities/ centre of excellence
- Provide a comprehensive package of services including condoms and prevention education with a view towards “Positive Prevention”
ART Centre - TB Diagnosis and Treatment
Image
DR TB cases are referred to DR TB centre.
Referrals for TB diagnosis are documented in the HIV TB line list which will be updated with the help of Senior Treatment Supervisor (STS) according to the test reports.
TB HIV registers are maintained in the ART centres to document TB cases.
INH preventive Therapy (IPT) - is initiated for all eligible PLHIV at ART centre
Resources
- Operational Guidelines for ART Services, NACO, GoI, 2012.
- TB/ HIV Module for ART Centre Staff National AIDS Control Organisation and Central TB Division, Ministry of Health & Family Welfare, GoI, 2010.
Assessment
Question Option 1 Option 2 Option 3 Option 4 Correct answer Explanation Page ID Pre-test Post-test Which of the following is false with regard to the ART Centre? It is an HIV diagnostic facility. It provides treatment for PLHIV. It treats opportunistic Infection. It has TB screening facilities. 1 ICTC is the diagnostic facility. Link ART Centre
ContentLink ART Centre (LAC) aims for easy accessibility of treatment services for People Living with HIV (PLHIV) by reducing the distance, cost, and waiting hours for Anti-retroviral Treatment (ART) and thereby increasing treatment adherence. They are linked to a Nodal ART centre.
Link ART Centre Plus (LAC Plus) is LAC which performs pre-ART management also. This will help to bridge the gap between Integrated Counselling and Testing Centre (ICTC) and Care, Support & Treatment (CST) services. These patients shall be followed up at LAC plus till they become eligible for ART or are referred to the ART centre for any other reason.
In addition to the existing infrastructure of ICTC where LAC is being established, at least one additional room is required for the nurse provided by the institution, for record keeping and other LAC functions.
Facility Location Staff Pattern Services LAC ICTCs of:
- District hospital (which does not have ART)
- Subdistrict hospital
- CHCs
No new recruitment for LAC
Responsibilities are allotted to the existing staff of the institution with training in ART services
The team comprises:
- Medical officer (MBBS/ MD medicine)
- Counsellor- ICTC Counsellor
- Staff nurse
- Pharmacist
- Anti-retroviral (ARV) drug dispensing
- Monitoring of PLHIV on ART
- Counselling on adherence, nutrition & positive prevention
- Treatment of minor Opportunistic Infections (OIs)
- Identification of side–effects of ARVs
- Tracing of Missing (MIS)/ Lost to follow-up (LFU) cases
- Screening for TB symptoms on every visit
- Psychosocial support to PLHIV
- Back referral to nodal ART centre as per specified criteria
LAC Plus Selected LAC are upgraded to LAC plus - One additional staff nurse can be recruited for LAC
plus
The team comprises of existing:
- Medical officer
- Counsellor
- Pharmacist
- Lab Technician
- Staff nurse (newly recruited)
- All the services at LAC are offered
plus
- Enrolment of PLHIV in HIV care and treatment (Pre-ART care)
- Pre-ART management - basic investigations and CD4 testing through linkage
- Regular follow-up of pre-ART patients not eligible for ART
- Referral of eligible patients to nodal ART centre for ART initiation
- Line listing and reporting of HIV-TB cases to nodal ART centre
Only patients from the designated nodal ART centre shall be linked to the attached LAC/ LAC plus.
Patients satisfying all of the following conditions shall be linked out to Link ART centres:
1. PLHIV on ART for a minimum of six months at the nodal ART centre
2. Those who have exhibited an increase in CD4 count and clinical improvement after 6 months of initiating ART
3. Do not have any active OI
4. The patient is a resident of an area closer to the LAC than to the nodal ART centre
5. Those who are willing to be linked out and collect their ARV drugs from the LAC, once the above conditions are fulfilled
Copy of Link out/in format to be exchanged between nodal ART centre and LAC while linking out or linking in the patients and a soft copy of these are to be maintained by both nodal ART centre & LAC/ LAC plus in a separate folder.
LAC/ LAC plus shall not initiate/ modify ART in any patient at any time.
Resources
Assessment
Question Option1 Option2 Option3 Option4 Answer Explanation Page id Pre-test Post-test Which of the following is false regarding Link ART Centre (LAC)? Link ART centre increases the accessibility to care for PLHIV. It helps in treatment adherence. TB screening is done for PLHIV attending LAC. Can initiate ART. 4 LAC/ LAC plus cannot initiate ART.
ART Centre of Excellence
ContentCentres of Excellence (CoE) in HIV care were established with an objective to set up model treatment centres, impart high-quality training, and undertake operational and clinical research about HIV/ AIDS on a larger scale.
Structure and Activities of Centre of Excellence
Image
The Anti-retroviral Treatment (ART) CoE are located in medical colleges and tertiary care centres of high technical repute. The CoE ideally should have an environment that is comfortable for the care provider as well as the beneficiary to obtain optimal results.
- The ART centre of the institution should be an integral part of the CoE as the key centre providing clinical HIV care for persons infected/ affected by HIV.
- There should be a functional integration of the ART centre with CoE.
- Paediatric CoE/ paediatric department, Prevention of Parent to Child Child Transmission (PPTCT) services, laboratory services and inpatient care in the institution should be linked to the CoE to ensure comprehensive HIV care.
Manpower in CoE
- Programme Director - Faculty of the institution associated with the National AIDS Control Organisation (NACO) programme
- Deputy Programme Director- identified from the institution
Additionally recruited staff on a contract basis include:
- Research Fellow (Clinical) - 1
- Research Fellow (Non-clinical) - 1
- SACEP Coordinator -1
- Data Analyst – 1
- Training and Mentoring Coordinator – 1
- Laboratory Technician – 1
- Nutritionist – 1
- Outreach Workers/ Social Workers- 2
CoE Team - Multidisciplinary team headed by the Head of the institution. It should consist of trained faculty from the departments of Medicine, Microbiology, Obstetrics & Gynaecology, Paediatrics, Community Medicine, Dermatology and Venereology. This team reviews the functioning of the CoE. Members of this team will also be engaged as resource persons in various training programmes organised by NACO/ State AIDS Prevention and Control Societies (SACS) after their certification as national trainers.
Steering Committee - Headed by the head of the institution. Members of this Committee should include the Programme Director, Deputy Programme Director, Director of concerned SACS and a NACO representative. This committee should meet once in 3 months to review of the functioning of CoE and to sort out any issues related to its functioning.
State AIDS Clinical Expert Panel (SACEP ) consists of - 1) Programme Director of CoE/ Deputy Programme Director/ Nodal Officer of ART centre 2) External ART expert 3) Regional Coordinator/ Joint Director (Care Support and Treatment)/ Consultant (CST) at SACS.
Treatment Linkage to CoE
Patients from ART centres experiencing treatment failure with first-line ART or drug toxicity are referred to the CoE for further evaluation and second-line treatment/ Alternate first-line treatment as per the linkage plan.
Resources
Assessment
Question Option 1 Option 2 Option 3 Option 4 Answer Explanation Page id Pre-test Post-test Which of the following statement is false in relation to the Centre of Excellence ART centre? Has research facilities Has an expert panel to discuss referred cases Does not have a basic ART centre Located in a medical college 3 The ART centre of the institution should be an integral part of the CoE.
Fullscreen


