DR-TB Services and Functions of Stakeholders
ContentEach of the stakeholder plays important role in DR-TB service delivery and has specific responsibility which is being monitored.
The flow diagram below depicts the processes involved in the delivery of drug-resistant tuberculosis (DR-TB) services and specific functions of various stakeholders.
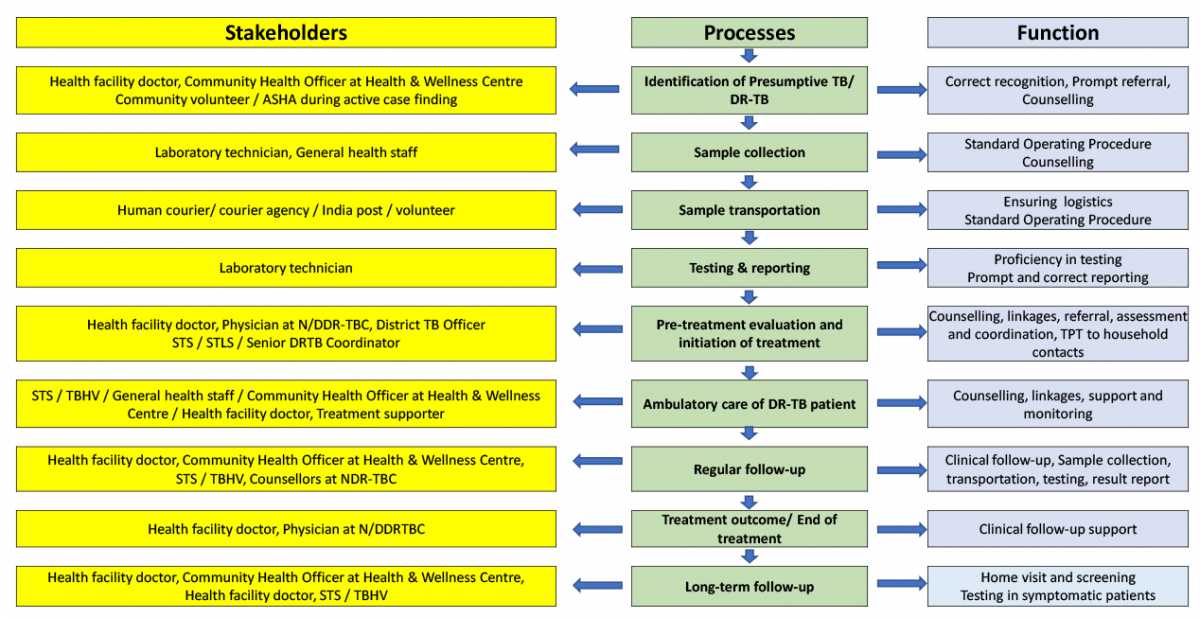
Figure 1: Cascade of DR-TB services and functions of various stakeholders
Source: Guidelines for PMDT in India, 2021, p.8
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
PMDT structure and roles
ContentThe National TB Elimination Programme (NTEP) in India has established well-organised Drug-resistant TB (DR-TB) management structures at the national, state and district level.
Image
Figure: Diagrammatic representation of the organisational structure of Programmatic Management of DR-TB (PMDT)
Abbr: NDR-TB: Nodal Drug-resistant TB; NAAT: Nucleic Acid Amplification Test; LPA: Line Probe Assay; CDST: Culture and Drug Sensitivity Test; DDR-TB: District DR-TB
The organisational structure and functions at different levels are described in the table below.
Level Organisational Structure Type of Organisation Function National-level Central TB Division (CTD), Ministry of Health and Family Welfare (MoHFW), Government of India (GoI) Administrative Providing resources/ devising policies/ issuing guidelines/ monitoring and evaluation/overall administration of the programme National Technical Expert Group Advisory Reviewing evidence Recommendation in guidelines National Reference Laboratory (NRL) Operational Providing laboratory-related expertise, External Quality Assurance (EQA) guidelines, Accreditations, a centre of excellence in diagnostics State-level State TB Cell, Health Department Administrative Providing resources, implementing guidelines, monitoring and evaluation/ overall administration of the programme State PMDT Committee Advisory Overseeing implementation as per guideline, taking strategic decisions, reviewing the progress in implementation and feedback/ suggestion to NTEP Nodal DR-TB Committee Advisory Guiding treatment of difficult to treat DR-TB cases, reviewing the progress of treatment and Adverse Drug Reaction (ADR) management, providing technical expertise for decisions at the State PMDT Committee, etc. Intermediate Reference Laboratory (IRL) Operational Providing laboratory-related services and expertise at the State level, EQA, and capacity building for diagnostic services Nodal DR-TB Centres Operational Providing treatment services to difficult-to-treat DR-TB cases, a centre of excellence in DR-TB treatment District-level District TB Cell Administrative Providing resources, implementing guidelines, monitoring and evaluation/ overall administration of the programme District TB Forum Advisory Overseeing implementation as per guideline, reviewing the progress in implementation, facilitating and monitoring the involvement of communities District Comorbidity Committee Advisory Review and rectify TB-comorbidity components with regard to HIV, diabetes, addiction and other review coordination with other health programmes like Rashtriya Bal Swasthya Karyakram (RBSK), Rashtriya Kishorethe Swasthya Karyakram (RKSK), Reproductive Maternal Newborn Child plus Adolescent Health (RMNCH+A) etc. District DR-TB Committee Advisory Guiding treatment of DR-TB cases, reviewing progress of treatment and ADR management, etc. NAAT/ LPA/ CDST Laboratories Operational Providing diagnostic services to detect DR-TB in the district (at more than one district) District DR-TB Centre Operational Providing treatment services to DR TB cases, ADR management etc. DR-TB services integration into the general health system
Block-level/ Ward-level Block Medical Officer/ Medical officer in office Operational Implementation of guidelines/ monitoring and evaluation of feedback Health facility-level Health facility doctor, Master in Public Health Skills (MPHS), Multipurpose Health Worker (MPHW), Accredited Social Health Activist (ASHA) Operational Implementation and review Health & Wellness Centre, Sub-Centre Community Health Officer (CHO) Operational TB screening and community intervention, coordination amongst various health programmes for TB-related activities Community ASHA, Panchayati Raj Institutions (PRI), Anganwadi Workers (AWW), other volunteers and community leaders Operational Implementation , community engagement through PRI, Village Health and Nutrition Day (VHND) , Community meetings, peer educators/TB champions/adolescent groups and Anganwadi sessions The organisational structure based on functional roles can be classified into diagnosis, treatment and drugs.
Diagnosis:
Name of Facility
Functions
Health Facility
- To identify presumptive cases/collect and transport specimen
- To communicate results to patients
- Collect and refer follow-up specimen
NAAT Site
- Diagnose TB and Rifampicin-resistant (RR) patients at district/ sub-district level
- Maintain records for Ni-kshay
- Transport the second sample to C&DST lab for First-line Line Probe Assay (FL-LPA) and Second-line Line probe Assay (SL-LPA)
C&DST Lab
- Receive diagnosis and follow-up samples
- Performs FL-LPA, SL-LPA, Liquid Culture (LC) and LC-DST
- Maintain records for Ni-kshay (LIMS)
- Provide rapid results to district , field and DR-TB centre
Treatment:
Name of Facility
Functions
Health Facility
- Identify treatment supporter
- To support and supervise DR-TB patients during treatment
- Manage Minor side effects
- Refer patients for treatment initiation
District DR-TB Centre
- Initiate DR-TB regimen
- Manage and record ADR
- Consult for complications
- Maintain records and Ni-kshay
- Coordinated with Nodal DR-TB centre/Field
- Monitor DR-TB treatment
Nodal DR-TB Centre
- Maintain ward and Airborne Infection Control (AIC)
- Undertake pretreatment evaluation and initiate treatment
- Manage major ADR
- Mentor and supervise concerned DDR-TBC
Drugs:
Name of Facility
Functions
District Drug
Store
- Coordinate test results.
- Refer patients to N/DDR-TBC
- Coordinate the drug flow from the district drug store to the field level
- Maintain records, Ni-kshay, monitor and supervision
State Drug Store
- Prepare and ship drug boxes to the district level
- Manage supply chain for diagnostics and drugs
- Maintain records in Ni-kshay Aushadhi
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page id Part of Pre-Test Part of Post-Test Which of the following is part of the PMDT structure under NTEP? NACP NACO District Comorbidity Committee None of the above 3 The district comorbidity committee is part of the PMDT district-level structure. The committee reviews and rectifies TB-comorbidity components with regard to HIV, diabetes, addiction and other review coordination with other health programmes like RBSK. Yes Yes The PMDT organisational structure is based on functional roles that can be classified into diagnosis, treatment and drugs. True False 1 The PMDT organisational structure is based on functional roles that can be classified into diagnosis, treatment and drugs. Yes Yes - To identify presumptive cases/collect and transport specimen
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Nodal DR-TB Centre
ContentNodal Drug-resistant Tuberculosis Centres (NDR-TBCs) are established to manage all forms of DR-TB, including complicated cases. Therefore, the centre should have:
- Advanced general laboratory
- Allied investigation facilities for Pre-treatment Evaluation (PTE)
- Intensive Care Unit (ICU)
- Ventilator backup
- In-house lab/ linkages for PTE laboratory tests
The NDR-TBC is established as per the need and is generally in a tertiary care setting where expertise and facilities for the management of DR-TB are available.
The figure below shows an overview of services offered at the NDR-TBC.
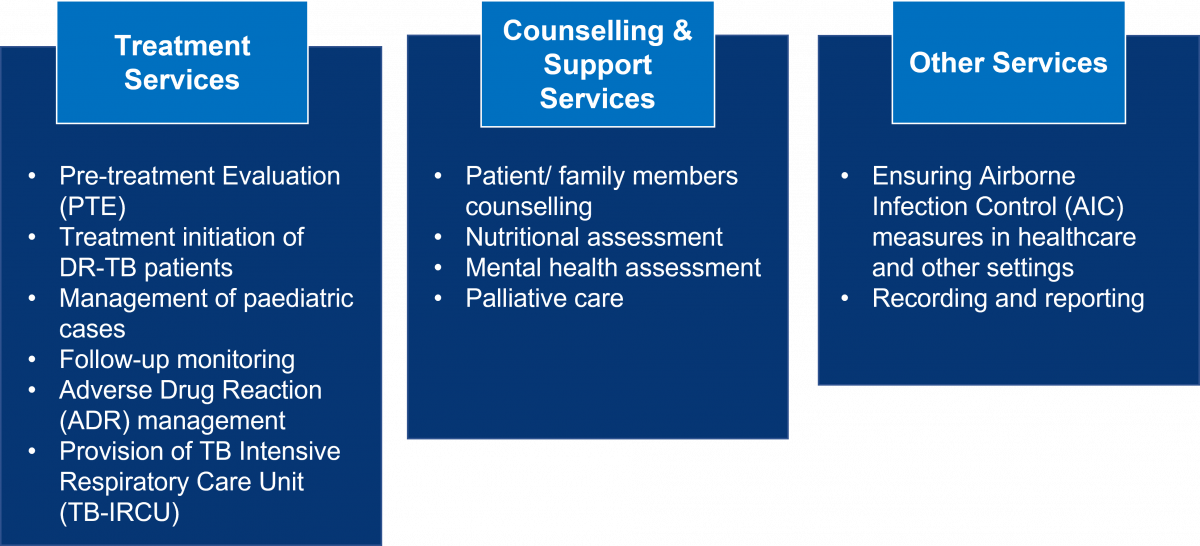
Figure: Range of Services Available at NDR-TBCs
District DR-TB Centres (DDR-TBCs) are linked with the NDR-TBC for the referral and management of complicated DR-TB patients like those who have:
- Additional resistance to second-line drugs, drug intolerance, serious adverse drug reactions, and contraindications
- Failing regimen, or patients returning after treatment interruption of more than 1 month
- The emergence of any exclusion criteria for a standard regimen for rifampicin-resistant TB or H mono/ poly DR-TB regimen
- Non-TB mycobacterial infections
- Need for palliative care or surgical interventions
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Requirements from Institutions for the Establishment of Nodal DR-TB Centre
ContentThe requirements from institutions for establishing Nodal Drug-resistant Tuberculosis Centres (NDR-TBCs) are as follows:
- It should preferably be a tertiary care institute.
- Separate wards for male and female patients (including children) should be available with at least 10 beds in each NDR-TBC.
- An outpatient clinic and a separate well-ventilated waiting area in an open-air, shaded area should be made available as per the Airborne Infection Control (AIC) guidelines.
- Administrative, environmental, and personal protective measures for airborne infection control should be placed in all indoor and outdoor facilities.
- All investigations under Pre-treatment Evaluation (PTE) and other Programmatic Management of Drug-resistant Tuberculosis (PMDT) services should be provided free of cost to the patient.
- Ancillary drugs should be provided for the management of Adverse Drug Reactions (ADRs) as per the NDR-TBC committee`s advice at no cost to patients.
- Oxygen and ventilators should be available for patients needing critical care support.
- The NDR-TBC committee should be formally established with the required set of experts as per the guidelines.
- All experts at NDR-TBC must be trained in the latest PMDT guidelines.
- Doctors, nursing and support staff should be available from the institute.
- Records and reports should be maintained for PMDT. Nikshay entries must be done on a real-time basis with regular electronic updates.
- Financial requirements must be availed through the institute/ state budgets or under National Health Mission (NHM).
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Mandatory Establishment of DR-TB Centres in All Medical Colleges
ContentIn view of the availability of expertise in medical colleges, there is a felt need to leverage their strength to improve clinical, Adverse Drug Reactions (ADRs) and comorbidity management of patients with Drug-resistant Tuberculosis (DR-TB) across India.
- Expansion of DR-TB services in the medical colleges will be helpful for enhancing the quality of care, treatment success and survival of these difficult-to-treat patients.
- National Medical Commission (NMC) issued a gazette notification in October 2020, mandating all medical colleges to establish a facility for the management of DR-TB by the time of 3rd renewal (admission of 4th batch of MBBS students).
- Private and Non-government Organisation (NGO) medical college hospitals are considered to serve as Nodal (N)/ District DR-TB Centre (DDR-TBC) at places where there is a need, either due to additional workload, non-availability of an appropriate public facility or preference of patients in the area.
- Terms and conditions for establishing that centre may be arrived at the local level as per the prevailing market rates in concurrence of the state/ district health society of the National Health Mission (NHM).
Resources
- Guidelines for Programmatic Management of Drug Resistant TB in India, 2021.
- Guidance Document of Partnerships, 2019.
- National Medical Commission, Gazette Notification, Government of India, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District DR-TB Centre
ContentDistrict Drug-resistant TB Centres (DDR-TBCs) are dedicated centres for providing DR-TB services for patients and can be established at the district or sub-district level.
- It may be established in institutes like medical colleges, district hospitals, TB hospitals and private or corporate institutes, trust hospitals or other sector hospitals, with the availability of required clinical expertise.
- There should be at least one DDR-TBC available in each district. However, more than one DDR-TBC can be established to improve the access and preference of patients to seek care.
- DDR-TBC can be established on an Outpatient Department (OPD) basis as well.
- Central TB Division (CTD) should be informed about the up-gradation of any institute to a DDR-TBC.
- Requirements for infrastructure and Human Resources (HR) may be proposed in the annual Programme Implementation Plan (PIP).
TB Services Available at the DDR-TB Centre
Pre-treatment Evaluation (PTE): Basic investigations required for initiating DR-TB regimens, examples include:
- Complete Blood Count (CBC)
- Thyroid-stimulating Hormone (TSH) tests
- Renal function tests
- Liver function tests
- Electrocardiogram, etc.
Treatment Services: Trained experts can initiate all DR-TB regimens at the DDR-TBC.
Resources
Functions of District DR-TB Centre
ContentThe following functions and package of services should be offered at each District Drug-resistant Tuberculosis Centre (DDR-TBC):

Figure: Functions of DDR-TBCs
Abbr: NDR-TBC: National Drug-resistant TB Centre; AIC: Airborne Infection Control
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Requirements for Establishing District DR-TB Centres
ContentThe following are requirements from institutions for establishing the district Drug-resistant Tuberculosis Centre (DDR-TBC):
Structural requirements:
- It should preferably be a secondary care institute.
- Separate wards for male and female patients (including children) should be available with at least two beds in each for DDR-TBC.
- An outpatient clinic and a separated well-ventilated waiting area in an open-air, shaded area to be made available as per the Airborne Infection Control (AIC) guidelines.
- Administrative, environmental and personal protective measures for airborne infection control should be placed in all indoor and outdoor facilities.
Infrastructure requirements:
- All investigations under Pre-treatment Evaluation (PTE) and other Programmatic Management of Drug-resistant Tuberculosis (PMDT) services should be provided free of cost to the patient.
- Availability of oxygen and ventilators for patients needing critical care support.
- Ancillary drugs must be provided for the management of Adverse Drug Reactions (ADRs) at no cost to patients, as per the DDR-TBC committee's advice.
Human resource requirements:
- The DDR-TBC committee should be formally established with the required set of experts as per guidelines.
- Services of specialists, if not available in the public facility, may be hired from the private sector under National Health Mission (NHM).
- All experts at DDR-TBC must be trained in the latest PMDT guidelines.
- Doctors, nursing and support staff should be available from the institute.
- Records and reports to be maintained for PMDT. Nikshay entries must be done on a real-time basis with regular electronic updates.
- Financial requirements should be availed through institute/ state budgets or under the NHM.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Nodal DR-TB Centre Committee
ContentThe Nodal Drug-resistant Tuberculosis Centre (NDR-TBC) committee is a clinical committee that is responsible for taking decisions regarding the management of DR-TB patients at the NDR-TBC.
The composition of the NDR-TBC committee is provided in the table below.
Table: Composition of the NDR-TBC Committee; Source: PMDT Guidelines for India, p205.
TITLE DESIGNATED OFFICIALS Chairperson Medical Superintendent or Director of the institute Vice-chairperson HoD Respiratory Medicine or General Medicine Nodal officer Senior Doctor from the department hosting the NDR-TBC Member secretary Senior Medical Officer- DR-TB centre Member HoD Microbiology or IRL Microbiologist Member HoD Psychiatry* Member HoD Ob&Gy* Member HoD ENT* Member HoD Dermatology* Member HoD Pharmacology Member Cardiologist* or Physician Member 1 Eminent Pulmonologist from NGO/ private sector Member WHO NTEP Consultant Member DTO of the district where NDR-TBC is located Special invitees DTOs of the districts linked (as and when needed) *To be consulted physically or virtually as and when required.
Abbr: HoD: Head of Department; IRL: Intermediate Reference Laboratory; Ob&Gy: Obstetrics and Gynaecology; ENT: Ear, Nose and Throat surgeon; NGO: Non-governmental Organisation, WHO: World Health Organisation, NTEP: National TB Elimination Programme, DTO: District TB Officer
Note: The chairperson can co-opt other specialists as required. The routine clinical decisions can be taken by the available doctor and informed to the NDR-TBC in subsequent meetings.
Functions of Nodal DR-TBC
- Periodically review the implementation status of PMDT in the respective nodal DR-TB centre to ensure that NTEP PMDT policies and guidelines are being followed.
- Coordinate with the IRL/ Culture and Drug Susceptibility Testing (C&DST) labs for Drug Susceptibility Testing (DST)/ Drug Resistance Testing (DRT) results and enter the details in Nikshay.
- Arrange for examination of DR-TB patients referred for their treatment eligibility, open treatment book and start PMDT regimen for all eligible patients.
- Admit DR-TB patients who may require the indoor facilities of the DR-TB centre.
- Arrange tele/ video consultation with relevant specialists on a case-to-case basis as well as with linked DDR-TBC to provide required clinical decision support.
- Empanel the private practitioners of various disciplines if the required specialist is not available in the public sector. In coordination with the respective State TB Officer (STO) and DTOs, ensure that drug ordering and distribution is managed in a timely and appropriate manner.
- Account for the review of record, report, Nikshay data entry.
- Monitor performance of DR-TB and PMDT in catchment geography using analysis of data from downloadable Nikshay reports and dashboard.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
District DR-TB Centre Committee Composition and Functions
ContentThe district drug-resistant tuberculosis centre (DDR-TBC) committee is a clinical committee where the dean/principal/ director of the institute is the chairperson.
- The Head of the Department (HoD) or a senior faculty member from the department of pulmonary medicine/general medicine is the nodal officer of the committee.
- The HoDs or senior faculty members of other specialties are the members of the committee.
- The clinical function of these committees must be adequately supported by the administrative or management committees of the institution in which district TB officer (DTO) is an ex-officio member.
- The composition of the DDR-TBC committee is shown in Figure 1.
Table 1: Composition of DDR-TBC committee; Source: Guidelines for PMDT, India 2021, p. 206 TITLE DESIGNATED OFFICIALS Chairperson Chief Medical Officer Co-chairperson Medical Superintendent/Director/Head of the institute Nodal person Physician in-charge of DDR-TBC Member Secretary DTO of the district Members Specialists* from pulmonologist, microbiologist, psychiatrist, Ob & Gy, cardiologist, ENT, dermatologist, pharmacologist etc. Member MO medical college, if placed Member Medical consultant (concerned), WHO NTEP TSN Member Any other invited member, if required *specialist available in-house, outsourced from private sector or linked with NDR-TBC Ob&Gy: Obstetrics and Gynaecology, ENT: Ear, nose and throat surgeon; MO: Medical Officer, WHO: World Health Organisation, NTEP: National TB Elimination Programme, TSN: Technical Support Network
Resources
District DR-TB Centre Committee: Terms of Reference [ToR]
ContentThe Terms of Reference (ToR) for the District DR-TB Centre (DDR-TBC) committee are:
- Ensure arrangements for patient treatment initiation as per the Programmatic Management of Drug-resistant Tuberculosis (PMDT) guidelines.
- Periodic review of treatment initiation, active Drug Safety Monitoring and Management (aDSM) and patient monitoring activities carried out at the DDR-TBC.
- Coordinate with the District TB Officer (DTO), TB Unit (TU), Health Facility (HF), other departments and Non-governmental Organisations (NGOs) to ensure the patient is linked with all essential services required.
- Empanel the private practitioners of various disciplines which are not available in the committee and are required for the management of DR-TB.
- Arrange tele/ video consultation with a relevant specialist on a case-to-case basis as well as with the linked nodal DR-TB centre to seek guidance required for clinical decision support. The DDR-TBC should also arrange tele/ video consultation with HFs on a case-to-case basis to provide required clinical decision support.
- Account for review of record, report, and Nikshay data entry.
- Monitor performance of DR-TB and PMDT in the catchment geography using analysis of data from downloadable Nikshay reports and dashboard.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Referral mechanisms for DR-TB services
ContentPresumptive Drug-resistant TB (DR-TB) is identified by the health facility doctor during passive screening or by health staff/ community volunteers during Active Case Finding (ACF).
Prompt referral and sample collection is an important step after identifying presumptive TB/ DR-TB.
After detection, referrals should be made promptly by the Community Health Officer (CHO) at Health and Wellness Centre (HWC)/ Senior Treatment Supervisor (STS)/ Tuberculosis Health Visitor (TBHV) to the health facility or Nodal/ District DR-TB Centre (N/DDR-TBC) for pre-treatment evaluation and treatment initiation. Every district has DDR-TBC for the treatment of DR-TB cases. However, for complicated DR-TB cases,that need either super-speciality or complex medical equipment and intensive care (like invasive ventilators), such patients are referred to Nodal DDR-TBCs.
Referral linkages for further domiciliary treatment are to be ensured by health facility doctor, N/DDR-TBC, senior DR-TB TB-HIV supervisor, STS, TBHV, CHO and general health staff.
Identification of suitable treatment supporters by CHO/ STS/ TBHV is essential, and the periodic follow-up of clinical/ bacteriological examination is to be managed.
The cascade of referral mechanism and function of various stakeholders is described below.
Image
Figure: Cascade of referral mechanism and function of various stakeholders; Source: Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, NTEP, CTD, WHO, MoHFW, 2021, p48.
Resources
Assessment
Question 1 Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page id Part of Pre-Test Part of Post-Test The patients are referred to N/DDR-TBC for pre-treatment evaluation. True False 1 After detection of DR-TB, referrals should be made promptly by the CHO at HWC/ STS/ TBHV to the health facility or N/DDR-TBC. Yes Yes Who ensures referral linkages for domiciliary treatment of patients? Senior DR-TB coordinator TB Health Visitor Community health officers All of the above 4 Referral linkages for domiciliary treatment are to be ensured by the health facility doctor, N/DDR-TBC, senior DR-TB coordinator, TB-HIV supervisor, STS, TBHV, CHO and general health staff. Yes Yes Difficult-to-Treat TB Clinic [DT3C]
ContentThe Difficult-to-treat TB clinic (DT3C) is an initiative to support Drug-resistant TB Centres (DR-TBCs) for better patient management.
The DT3C structure is intended to handhold and mentor District DR-TB centres (DDR-TBCs) for the effective management of Drug-resistant TB (DR-TB) cases.
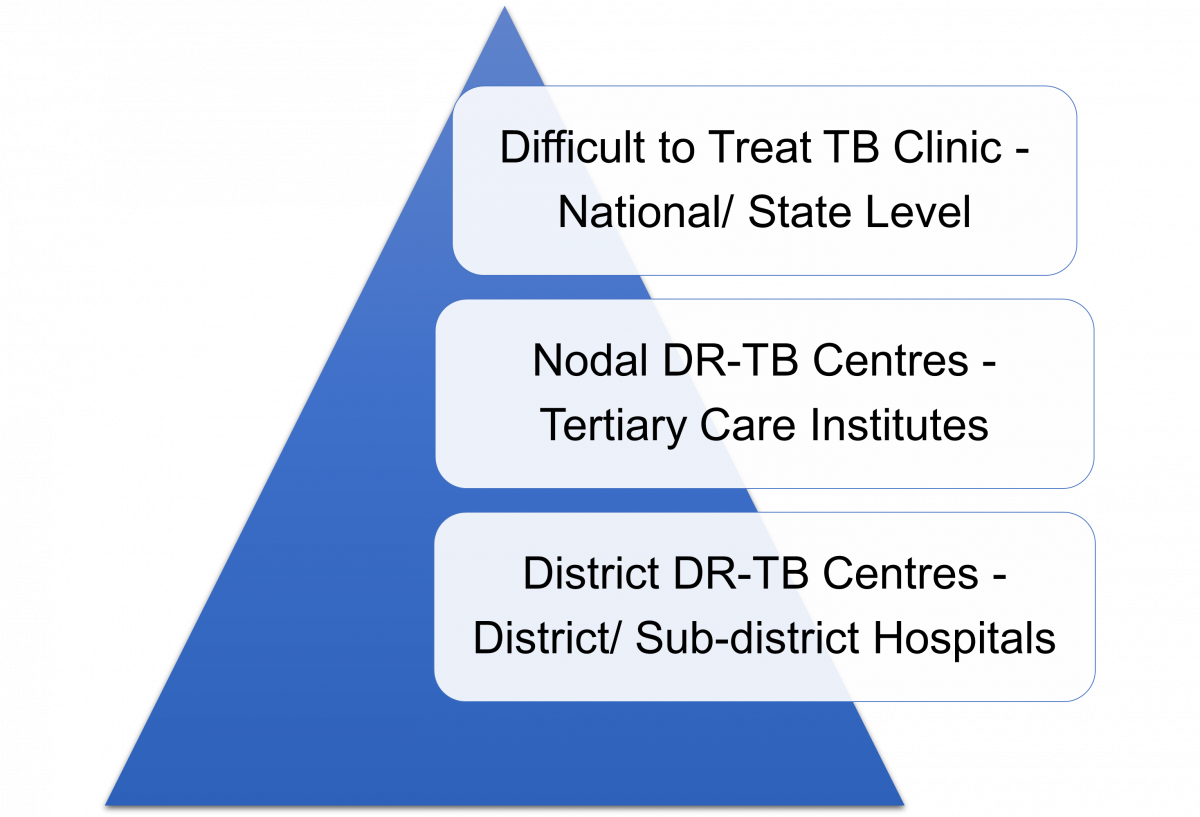
Figure: Difficult-to-treat TB Clinic: Three-tier Structure
The DT3C operates via a three-tier structure which is intended to improve the quality of DR-TB care:
- The DT3C is functional at the national level through the collaboration of the National Institute for Tuberculosis and Respiratory Diseases (NITRD), Central TB Division (CTD) and the National Task Force (NTF).
- Experts involving various specialties are included in the team as mentors at state-level D3TC.
- Information/ queries regarding the patient are shared in a standardized format by the DDR-TBC beforehand to facilitate discussions through the state nodal officer.
All states should have at least one (more than one in larger states) DT3C established.
Resources
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB HIV Coordinator and their role
ContentThe roles of the Drug-resistant TB (DR-TB) HIV Coordinator are:
1. Providing technical assistance to District TB Officer (DTO) for:
- Organising Programmatic Management of Drug-resistant TB (PMDT) services in the district
- Supporting District DR-TB Centre (DDR-TBC) for data management in Ni-kshay and their coordination with Anti-retroviral Therapy (ART) centre in the districts
- Organising TB-HIV coordination activities in the district
- Providing training to the staff of health facilities (public and private) under his/her jurisdiction to carry out PMDT and TB-comorbidity-related activities
- Conducting monthly reviews with TB Unit, National AIDS Control Programme (NACP), and Health and Wellness Centre (HWC) staff using dashboards and analysis of data from Ni-kshay periodically to address implementation and management gaps
- Activities related to drug and logistics supply chain management of drugs for PMDT, Cotrimoxazole Preventive Therapy (CPT) and Isoniazid Preventive Therapy (IPT) and modified TB regimen for People Living with HIV/AIDS (PLHA) with TB on second-line ART
- Coordinating regular sharing of the information related to TB-HIV coordination by assisting the nodal officer
- Mapping, prioritising, and engaging health facilities and laboratories in the private sector, Non-government Organisations (NGOs) and other sectors to improve access and quality of DR-TB care for all as per guidelines
- Preparing and maintaining a directory of Integrated Counselling and Testing Centres (ICTCs), ART centres/ Link ART Centres (LACs), community care centres, Non-communicable Disease (NCD) clinics, private health facilities and NGOs working for HIV, NCD in the district and the collaborating National TB ELimination Programme (NTEP) centres
- Providing a monthly activity report to the DDR-TBC committee and DTO.
2. Coordinating for smooth programme implementation
- Coordinate with all health staff and facilitate to subject all TB patients to universal Drug Susceptibility Testing (DST) at the linked decentralised Nucleic Acid Amplification (NAAT) sites and NTEP certified laboratories in the public and private sectors.
- Ensure that initial home visits are conducted by health workers to all newly diagnosed DR-TB patients of the district.
- Ensure that staff organises treatment support, all public health actions, follow-up reminders and transportation support for DR-TB patients.
- Help staff in proactive reach out to patients for follow-up cultures/ investigations as per schedule for every patient.
- Coordinate with and support TB Units, HWCs staff and private doctors to regularly update the directory of treatment supporters for DR-TB patients at the district level and facilitate their training.
- Facilitate the DR-TB treatment initiation at DDR-TBC.
- Ensure PMDT treatment books are updated for all patients at DDR-TBC, TB Units (TUs) and HWCs.
- Ensure and monitor the PMDT data completion in Ni-kshay and give periodic TU/ Peripheral Health Institute (PHI)-wise feedback to the DTO about the same.
- Liaise with respective Nodal Drug-resistant TB Centres (NDR-TBCs) for updating information on Ni-kshay and patient care.
- Ensure complete, correct and timely compilation and transmission of PMDT/ TB- HIV information.
- Establish linkages with the District TB Centre (DTC), District AIDS Prevention Control Unit (DAPCU), collaborating NGOs and hospitals of the district.
- Facilitate change management with respect to the use of Information, Communication and Technology (ICT) tools, Ni-kshay, Ni-kshay-Aushadhi for concerned data entry, validation & its use for public health action.
- Support DDR-TBC in updating the template with information to be shared with difficult-to-treat TB clinic for selected patients as per directions from the DDR-TBC committee and management of the patient based on recommended actions from the clinic.
3. Supervising and monitoring
- Monitor time to treatment of DR-TB patients and provide feedback on a periodic basis.
- Supervise all DR-TB patients and treatment support centres along with concerned TB Units, HWCs staff and private providers.
- Evaluate referral systems between ICTCs, ART centres, NCD, and NTEP and promote providing feedback to the referring centre.
- Field visits in the districts for at least 15 days a month, including Joint TB-Comorbidity visits on a tour programme approved by DTO.
4. Capacity building and imparting skills
- Train and supervise the pharmacists/ responsible staff of district/ TB Unit/ HWC drug stores in maintaining adequate stock of second-line drugs.
- Train staff for preparation of monthly patient-wise boxes by regimen and weight band as well as initialisation of Medication Event Reminder Monitor (MERM) devices, as available, for every patient initiated on DR-TB treatment at the NDR-TBC as per guidelines.
Resources
DO Letter - TOR and Needs Norms for NTEP Staff, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of pre-test
Part of post-test
DR-TB HIV coordinator should coordinate with all health staff and facilitate to subject all TB patients to universal DST.
True
False
1
DR-TB HIV coordinator should coordinate with all health staff and facilitate to subject all TB patients to universal DST at the linked decentralised NAAT sites and NTEP-certified laboratories in public and private sector treatment.
Interaction of DR-TB Coordinator with the TB Patient Care Ecosystem
ContentThe DR-TB HIV coordinator interacts with the TB patient care ecosystem as follows:
Patients: UDST at linked NAAT sites, treatment initiation, adherence monitoring and follow-up, ADR identification and management, contact tracing, linking with welfare schemes, linkage with the TB care ecosystem.
Treatment supporters: To ensure initial home visits, treatment support, and all public health actions.
STLS: To subject all TB patients to universal DST at the NAAT sites, to ensure complete DST and the laboratory follow-up of all the patients.
STS: Treatment initiation of DR-TB patients, necessary treatment support, Public health actions, and coordinate for follow-up cultures and investigations.
Medical officers: Facilitating DR-TB treatment initiation and management of ADR.
DR-TB Committee: Support DDR-TBC in providing the information about the DR-TB patients, and coordinate with the different staff to execute the decision of N/DDR-TBC. Updating the template with the information to be shared with difficult-to-treat TB clinic for supported patients.
Pharmacists/responsible staff of district/TB Unit/HWC drug stores: Maintaining adequate stock of second line drugs, preparation of monthly patient wise boxes by regimen and weight bands initialization of MERM devices.
Ni-kshay and Ni-kshayAushadhi: Use of ICT tools, Ni-kshay, Ni-kshay-Aushadhi for concerned data entry, validation and its use for public health action and monitoring the PMDT data completion in Ni-kshay and give periodic TU/PHI-wise feedback to the DTO about the same.
DTO/ Programme Managers: Seek overall guidance from DTO/Program managers for executing their duties and responsibilities. They also provide with necessary data and information about the PMDT facilitating supervision and monitoring and discuss and implement various solutions for the identified issues.
Resources
Assessment
Question 1
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of Pre-Test
Part of Post-Test
DR-TB HIV coordinator should coordinate with all health staff and facilitate subjecting all TB patients to universal DST.
True
False
1
DR-TB HIV coordinator should coordinate with all health staff and facilitate subjecting all TB patients to universal DST at the linked decentralised NAAT sites and NTEP-certified laboratories in public and private sector treatment.
Yes
Yes
Fullscreen