-
IEC-CH10: Counselling
FullscreenTB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
IEC-CH11: Social Inclusion and Wellness activity
FullscreenDeterminants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Socio economic factors affecting TB patients
ContentSocio-economic factors affecting TB patients are:
1. General socioeconomic conditions of the society, culture and environment. This includes:
-
Gross Domestic Product (GDP)
-
Immigration
-
Urbanisation
-
Incidence of TB in the country
-
Labour policy
-
Access to healthcare
2. Socioeconomic position of the individual. This includes:
-
Income
-
Education
-
Occupation
-
Social class/ caste
-
Indigenous/ tribal population
-
Gender
3. Living and working conditions. This includes:
-
Housing conditions (overcrowding and poor ventilation especially in night shelters, de-addiction centres, old age homes, prisons)
-
Employment conditions - Occupation with risk of developing TB (mines, coal industry, sand blasting industries, weaving & glass industries, stone-crushers, cotton mill workers, tea garden workers, rice mill workers, etc.,)
-
Homelessness
-
Hard to reach areas
-
Urban slums
3. Psychosocial risk factors, such as:
-
Social exclusion
-
Depression
4. Individual lifestyle risk factors, such as:
-
Smoking
-
Alcohol abuse
-
Tobbaco use
-
Drug abuse
-
Nutrition (malnutrition)
-
Co-morbidities like diabetes mellitus, malignancies, patients on dialysis and on long term immunosuppressant therapy HIV, past history of TB
Resources
- NTEP Training Modules (1 to 4) for Programme Managers & Medical Officers, CTD, 2020.
- Social Determinants of Tuberculosis Context Framework and the Way Forward to Ending TB in India, IPH, India, 2020.
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Socio-economic factors affecting TB patients are:
-
Housing
-
Income
-
Access to healthcare
-
Alcohol abuse
1,2
2,3,4
1,2,3,4
1,2,4
3
TB is one of the few diseases which reflects and expresses social inequalities. Living conditions, economic conditions, lifestyle, and access, affordability, and availability of healthcare are factors which affect TB patients.
-
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
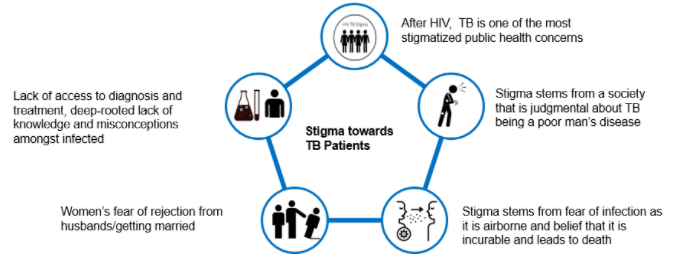
Stigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Rehabilitation service to TB patients
ContentThe holistic management of Tuberculosis (TB) patients can improve their life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
Table: Rehabilitation services for TB patients Rehabilitation Services for TB Patients Care Providers Key Components Nutritional Rehabilitation 1. Senior Treatment Supervisor
2. TB Health Visitors
3. Accredited Social Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at Peripheral Health Centre (PHC), Community Health Centre (CHC) level
-
Supporting nutritional needs of TB patients through Ni-kshay Poshan Yojana
-
Management of undernutrition in nutrition rehabilitation centres (NRCs)
-
Linkages for extra nutritional support for TB patients like the public distribution system (PDS) or food security act.
Pulmonary Rehabilitation
1.Physiotherapists (preferable one male and one female)
2. Nurses
3. Attendant
Management of physical and psychological impairment due to the disease to lower the handicap. Physical Rehabilitation -
therapists (preferable one male and one female)
-
Nurse Doctors
-
Surgeons
-
Physio
-
Attendant
-
Management of post-treatment sequelae by early identification and periodic assessment.
-
Comorbidity management
Social Rehabilitation 1. TB Health Visitors
2. Accredited Social
3. Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at PHC, CHC level
7. Ni-kshay Mitra
-
Linkage for vocational rehabilitation e.g., Skill India
-
Synergy between social welfare support systems like:
-
Rashtriya Swasthya Bima Yojana (RSBY)
-
TB pension schemes
-
National rural employment guarantee scheme
-
National Health Protection Scheme (NHPS) for palliative care and rehabilitation
Mental Rehabilitation 1. Psychiatrist
2. Psychologists / Counsellors
3. TB Health Visitors
4. Accredited Social
5. Health Activists (ASHAs)
6. Auxiliary Nurse Midwife (ANM)
7. TB treatment supporter
8. Medical officers at PHC, CHC level
-
Psychological counselling to the patient and caregivers.
-
Assisting patients in the planning of decisions related to the end-of-life stage.
Patient rehabilitation is ensured by:
-
1. IT-based monitoring via Ni-kshay platform
-
2. Community-based monitoring
-
3. Surveillance: A comprehensive surveillance system for TB patients and their providers built into eNikshay. This is supported by a call centre for user-friendly private reporting and patient monitoring.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Rehabilitation services to TB patients comprise Nutritional, Physical, Pulmonary, Social and Mental Rehabilitation.
False
True
2
The holistic management of tuberculosis (TB) patients can improve life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
-
Palliative Care in TB patients
ContentPalliative care is specialised medical care for people living with a serious illness.
- This type of care is focused on providing relief from the symptoms and stress of the illness.
- The goal is to improve the quality of life for both the patient and the family.
- Palliative care is based on the needs of the patient, not on the patient’s prognosis.
Need for Palliative Care for TB Patients
TB is, and should be, a curable disease; however, each year an increasing number of patients acquire or develop drug-resistant TB (DR-TB), which has a much lower cure rate.
While the expectations are to have increasing numbers of treatment success rates, DR-TB remains a life-threatening condition with high mortality.
The life-threatening nature of DR-TB and the burden of disease management in terms of symptoms, adverse treatment effects, adherence, stigma and subsequent discrimination and social isolation, clearly show the need for care that addresses physical, social and emotional suffering by patients.
Thus, the need for palliative care is being increasingly recognised as an important part of the continuum of care for DR-TB patients.
Challenges in Palliative Care
At present, there is a scarcity of trained health workers and local community-based palliative care resources in the settings that are most in need. Although clinical expertise in palliative care for patients who die in respiratory distress has developed considerably, individuals with DR-TB are yet to see the benefits.
Services under Palliative Care for TB
- Addressing pain and symptom control (including respiratory insufficiency)
- Nutritional support
- Medical intervention after treatment cessation
- Ensuring the appropriate place of care, preventive care, infection control and end-of-life care
Supportive Measures in Palliative Care
Image
Resources
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Palliative care is based on a patient’s prognosis.
True
False
2
Palliative care is based on the needs of the patient, not on the patient’s prognosis.
YES
YES
Patients' charter for TB care
ContentThe Patients’ Charter for Tuberculosis Care (the Charter) outlines the rights and responsibilities of people with TB. It empowers people affected by TB and their communities through this knowledge. Initiated and developed by persons affected by TB from around the world, the Charter makes the relationship with healthcare providers a mutually beneficial one.
The Charter sets out ways in which people affected by TB, the community, health providers (both private and public), and governments can work as partners in a positive and open relationship with a view to improve TB care and enhance the effectiveness of the healthcare process.
It allows for all parties to be held more accountable to each other, fostering mutual interaction and a positive partnership.
Principles of the Patients’ Charter for TB Care
- The charter practices the principle of Greater Involvement of People with TB (GIPT).
- This affirms that the empowerment of people with the disease is the catalyst for effective collaboration with health providers and authorities and is essential to victory in the fight to end TB.
Parts of the Patients’ Charter for TB Care
There are two main parts in the patients’ charter for TB care which cover:
- Patients’ rights
- Patients’ responsibilities
These parts are further delineated in Tables 1 and 2 below.
Table 1: Patient's Rights According to the Patient's Charter for TB Care Rights Explanation of rights: You, as the patient, have the right to: Care - Free and equitable TB quality care meeting the International Standards of Tuberculosis Care (ISTC)
- Benefit from community-care programmes
Dignity - Be treated with respect and dignity
- Social support of the family, community and national programmes
Information - Information about available care services — be informed about condition and treatment, know drug names, dosage and side-effects
- Access your medical records in the local language
- Have peer support and voluntary counselling
Choice - A second medical opinion, with access to medical records
- Refuse surgery if drug treatment is at all possible
- Refuse to participate in research studies
Confidence - Have your privacy, culture and religious beliefs respected
- Keep your health conditions confidential
- Care in facilities that practice effective infection control
Justice - File a complaint about care, and have a response
- Appeal unjust decisions to a higher authority
- Vote for accountable local and national patient representatives
Organization - Join or organise peer support groups, clubs and Non-governmental Organisations (NGOs)
- Participate in policy-making in TB programmes
Security - Job security, from diagnosis through to cure
- Food coupons or supplements, if required
- Access to quality-assured drugs and diagnostics
Table 2: Patients' Responsibilities According to the Patients' Charter for TB Care Responsibilities Explanation of responsibilities: You, the patient, have the responsibility to: Share information - Inform healthcare staff all about your condition
- Tell staff about your contacts with family, friends, etc.
- Inform family and friends and share your TB knowledge
Contribute to community health - Encourage others to be tested for TB if they show symptoms
- Be considerate of care providers and other patients
- Assist family and neighbours to complete treatment
Follow treatment - Follow the prescribed plan of treatment
- Tell staff of any difficulties with treatment
Solidarity - Show solidarity with all other patients
- Empower yourself and your community
- Join the fight against TB in your country
Resources
- The Patients’ Charter for Tuberculosis Care, The Global Plan to Stop TB 2006-2015.
- Capacity-building of Affected Communities for Accelerated Response to Drug-resistant Tuberculosis in the South-east Asia Region, WHO, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test According to the Patients' Charter for TB Care, it is not the patient’s responsibility to support other patients. True False 2 According to the Patients' Charter for TB Care, patients have a responsibility to support other patients, show solidarity and empower their communities. Yes Yes
-
IEC-CH12: Linkages to Social Support Schemes
FullscreenDirect Benefit Transfer(DBT) under NTEP
ContentDirect Benefit Transfer (DBT) is a major initiative of Government of India (GoI) whereby any government subsidy or benefit is to be transferred directly into the beneficiary's bank accounts. Intermediary government agencies only manage the process of payments, without handling actutal money.
NTEP is one of the first health programmes in India to use a fully adopt DBT. It uses an end to end electronic system, to digitise beneficiary information and transfer monetary benefits. In NTEP to process benefits, two electronic systems are used, Ni-kshay (operated by NTEP) and PFMS (Public Finance Management System, operated by the Ministry of Finance). Ni-kshay enables Direct Benefit Transfer by digitizing the beneficiaries(bank account details of patients, treatment supporters and providers) and calculates of incentives/ benefits (eligible payment) and processes them for payment through PFMS under various schemes. The various schemes operational under NTEP are:
- Nikshay Poshan Yojana(NPY)
- Tribal Support Scheme
- Treatment supporter’s Honorarium
- Incentive for Notification and Outcome
DBT Schemes in Nikshay
Other Local DBT Schemes
ContentThere may be other Central or State government schemes and programmes that beneficiaries related to the TB program are eligible for, over and above the 4 schemes provided by the central government through NTEP. Some examples are:
- State Illness Relief Fund (can serve seriously ill TB patients)
- Chief Minister’s Farmers Security Scheme
- Nutritional Support to DR-TB Patients
- Sanjay Gandhi Niradhar Yojana
- Surakhaya Yojana
- Pridhar Parasar Yojana
- Scheme for treatment of critical disease for schedule caste/schedule Tribe and people below poverty line (BPL).
- Rastriya Swasthiya Bhima Yogana (RSBY) reimbursement for those TB patients who required hospitalisation
- Sudurvarti Sahayaks from CM's Sudurvarti Gram Yojana involved TB services
These schemes are paid through their respective payment processing channels and not through Ni-kshay.
Criteria for availing DBT Scheme benefits under NPY
Content- All TB patients notified on or continues treatment after 1st April 2018 including all existing TB patients under treatment are eligible to receive incentives.
- For availing DBT scheme benefits under NTEP Programme, TB patients have to provide their bank details to the nearest NTEP Health facility.
- The patient must be registered\notified on the NIKSHAY portal.
- Each beneficiary can be linked to unique savings bank account belonging to him/her. Beneficiaries without bank accounts need to be facilitated to open bank accounts in any bank as convenient.
- If a Beneficiary does not have a bank account and is unable to open a new bank account, his/her relative’s bank account may be used(immediate family member such as parents, spouse, siblings).
- If a relative’s bank account is used, written consent should be taken from beneficiary.
- If a bank account has already been used for another beneficiary, it cannot be re-used for another beneficiary. If a new Bank account needs to be opened, it’s easy to open a zero-balance account with Indian Post Payments Bank.
Fullscreen