-
IEC-CH6: DSTB Treatment and Care
FullscreenDS-TB Treatment – Patient Flow
ContentCommunity Health Volunteers(CHVs) have to refer the presumptive cases identified based on the r symptom screening to the nearest NTEP health facility for further investigation. Once Diagnosed with TB, the TB patients are initiated on the first-line TB treatment. Patients are also offered NAAT within a maximum of 15 days to rule out any drug resistance. If no drug resistance is detected, then the patient continues on the first-line TB treatment. TB patients are then clinically evaluated every month to check the progress of TB treatment.
The treatment duration of TB is divided into two phases - The Intensive Phase(IP) and the Continuation Phase(CP). Post-treatment completion, patients are then evaluated at intervals of 6,12,18 and 24 Months to ensure a relapse-free TB cure for the patient.
Figure: DSTB Treatment Flow
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
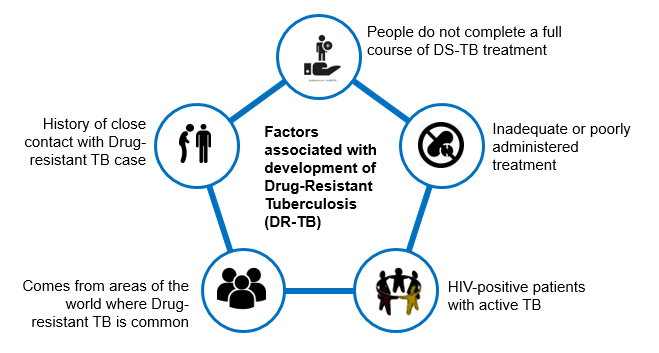
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
-
IEC-CH7: Treatment Adherence
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
-
IEC-CH8: TB infection and TPT
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
TB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes
-
IEC-CH9: TB Comorbidity
FullscreenComorbidity & special situation with TB
ContentSeveral medical conditions are risk factors for TB and poor TB treatment outcomes. Similarly, TB can complicate the course of some diseases. Therefore, it is important to identify these comorbidities in people diagnosed with TB to ensure early diagnosis and improved outcomes. When these conditions are highly prevalent in the general population, they can significantly contribute to the TB burden. Consequently, reducing the prevalence of these conditions can help prevent TB.
TB shares underlying social determinants with many of these conditions. Addressing the social determinants of health is a shared responsibility across disease programmes and other stakeholders within and beyond the health sector.
Figure: Various comorbid and special situation related with tuberculosis
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Pregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
Fullscreen