-
CDST_LT: Good laboratory practices
FullscreenGood Laboratory Practices
ContentGood laboratory practices help to maintain biosafety in TB lab settings. However, it is good to keep in mind that:
- NOTHING can totally eliminate the safety risk associated with the TB laboratory.
- Good laboratory practices with an emphasis on biosafety, significantly reduce the risk of laboratory-acquired infection.
- Specialized equipment aids good laboratory practice but does NOT replace it.
Good Laboratory Practices
- Biohazard signs (Figure 1) should be posted at the entrance to laboratories performing work on infectious agents and hazardous chemicals.
Figure 1: Biohazard Sign
- Laboratory access should be limited to essential staff.
- No eating, drinking, or smoking (Figure 2).
- No mouth pipetting (Figure 2).

Figure 2: No eating or mouth pipetting in lab
- No placing pencils or pens in the mouth.
- Keep hands away from eyes and face.
- Always wash hands before leaving the lab.
- Remove gloves before handling phones, instruments or computers.
- Minimize the use of mobile phones.
- Lab coats must be decontaminated and laundered regularly (never take them home for laundering!)
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Safety Precautions to be Followed in TB Laboratory Setting
ContentAs Tuberculosis (TB) infection spread in the form of droplet infection, healthcare workers in the TB laboratory setting need to follow standard safety precautions to prevent themselves from getting the TB infection.
Some of the safety precautions in the TB laboratory setting are as follows:
- Always allow proper ventilation by keeping all the windows open (Try to avoid sliding window doors, as most of the sliding doors open only half).
- Always wear proper Personal Protective Equipment (PPE) - Laboratory coat and gloves.
- Always have separate areas for administration, sample reception, smear preparation, staining and microscopic examination.
- Open the specimen bottle only when preparing slides.
- Avoid shaking or stirring of samples.
- Always spread the sample onto the slide gently in a regular motion.
- Always prepare slides in close proximity to a flame or in the biosafety cabinet to nullify the aerosols generated, if any.
- Always air-dry smears for 30 min before heat fixing.
- Always use wooden stick/ sterile loops for making smears.
- Always manage the laboratory waste correctly.
In case of other TB diagnostic settings like molecular labs, culture labs etc., follow the Standard Operating Procedure (SOP) properly (It is always advisable to display the SOP in all the TB diagnostic laboratories). The detailed SOPs of the procedures followed in the TB diagnostic facility should be displayed or placed wherever required, especially the BioMedical Waste guidelines, and all the SOPs should be updated regularly.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
CDST_LT: General concepts in IPC
FullscreenThe need for IPC
ContentInfection prevention and control (IPC) practices are important in maintaining a safe environment for everyone by reducing the risk of the potential spread of disease.
IPC is a practical, evidence-based approach which prevents patients and health workers from being harmed by avoidable infection. It is relevant to health workers and patients at every single health-care encounter.
Biosafety measures along with Universal Precautions like hand hygiene, personal protective equipment, safe injections, respiratory hygiene and cough etiquette is important in IPC to address the safe handling and containment of infectious microorganisms and hazardous biological materials.
IPC is essential in TB as:
1. specific population groups have a higher risk of acquiring TB infection and progressing to disease once infected; these groups include people living with HIV, health workers and others in settings with a high risk of transmission of M. tuberculosis
2. incident cases of TB among children (aged <15 years) reflect ongoing community transmission
3. primary person-to-person transmission of drug-resistant TB (as opposed to acquired resistance) is the dominant mechanism sustaining the global transmission of drug-resistant TB
4. to prevent TB transmission, interventions are needed that reduce the concentration of infectious particles in the air and the exposure time of susceptible individuals
Resources
1. Guidelines on Airborne Infection Control in Healthcare and Other Settings.
2. WHO guidelines on tuberculosis infection prevention and control 2019 update (https://apps.who.int/iris/bitstream/handle/10665/311259/9789241550512-e…)
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Person-to-person transmission of drug-resistant TB is the dominant mechanism for transmission of drug-resistant TB.
True
False
1
Primary person-to-person transmission of drug-resistant TB (as opposed to acquired resistance) is the dominant mechanism for transmission of drug-resistant TB.
Yes
Yes
Standard Precautions for IPC
Content- Standard precautions are a group of infection control practices to reduce the risk of transmission of pathogens.
- These are based on the principle that all blood, body fluids, secretions, excretions except sweat, non-intact skin, and mucous membranes may contain
transmissible infectious agents. - Standard precautions are applicable to all patients in all healthcare settings and combine the major features of universal precautions, body substance isolation, and airborne precautions.
- Implementation of standard precautions is based on risk assessment in all healthcare activities.
Image
Figure: Elements of Standard Precautions; Source: Guidelines on Airborne Infection Control in Healthcare and Other Settings
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings
- Health-care facility recommendations for standard precaution
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following are features of standard precautions?
Universal precautions Body substance isolation
Airborne precautions All the above 4 Standard precautions combine the major features of universal precautions, body substance isolation, and airborne precautions. Yes Yes Hand Hygiene
ContentHand hygiene is one of the most important elements of infection control. The aim of hand washing is to remove transient micro-organisms, acquired through everyday tasks in the laboratory/ clinical setting, from the surface of the hands.
Good hand hygiene protects both patients and staff.
The World Health Organization (WHO) guidelines on “Hand Hygiene in Healthcare” describe five key situations where hand washing is required:
- Before touching a patient
- Before a clean or aseptic procedure
- After body fluid exposure/risk
- After touching a patient
- After touching patient surroundings
Hand hygiene includes hand washing using soaps or hand rubbing with 70% alcohol-based formulations.
Important Considerations for Hand Hygiene
- Perform hand washing with soap and water if hands are visibly soiled and after using the restroom.
- Availability of running water supply is important for hand washing.
- If resources permit, perform hand rubbing with an alcohol-based preparation.
- Ensure availability of hand hygiene products (clean water, soap, single-use clean towels, alcohol-based hand rub).
- Alcohol-based hand rubs should ideally be available at the point of care.
Technique of Hand Hygiene (Figure)
- Handwashing (40–60 sec): Wet hands and apply soap; rub all surfaces; rinse hands and dry thoroughly with a single-use towel.
- Hand rubbing (20–30 sec): Apply enough product to cover all areas of the hands; rub hands until dry

Figure: Handwashing Technique; Source: WHO Handwashing Poster
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Health-care facility recommendations for standard precaution.
- WHO Handwashing Poster.
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Hand hygiene includes which of the following? Hand washing using soaps Hand rubbing with 70% alcohol-based formulations Sterilising the hands with hot air 1 and 2 4 Hand hygiene includes hand washing using soaps and hand rubbing with 70% alcohol-based formulations. Yes Yes Respiratory Hygiene
ContentRespiratory hygiene is vital to prevent the spread of TB via aerosols and person-to-person transmission.
Respiratory hygiene includes:
-
Covering the nose/mouth with a tissue when coughing/sneezing and appropriate disposal of used tissues
- If tissues are not available, cough or sneeze into the inner elbow (upper sleeve) rather than into the hand
- Keeping contaminated hands away from the mucous membranes of the eyes and nose.
- Carrying out hand hygiene after contact with respiratory secretions and contaminated objects/materials
- Using appropriate Personal Protective Equipment (PPE) during aerosol generating procedures
- Use PPE including gloves, long-sleeved gowns, eye protection (goggles or face shields), and facial mask (or respirators) during aerosol-generating procedures

Figure: Respiratory hygiene (Ministry of Ayush, https://twitter.com/moayush/status/1243852404640153601)
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings
- Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care
- Ministry of Ayush, https://twitter.com/moayush/status/1243852404640153601
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following are critical elements in respiratory hygiene?
Covering the nose/ mouth with a tissue when coughing/ sneezing
Throwing tissues used to wipe nasal secretions on the road
Using appropriate Personal Protective Equipment (PPE) during aerosol-generating procedures
None of the above
Options 1 and 3
Covering the nose/ mouth with a tissue when coughing/ sneezing and appropriate disposal of used tissues, as well as appropriate PPE usage during aerosol-generating procedures, are important elements of respiratory hygiene.
Yes
Yes
-
General Cleaning and TB Lab Surface Decontamination
ContentThe cleanliness and regular disinfection of the TB lab and its surfaces play an essential role in the safety of those working in these labs.Guidelines for Laboratory Cleaning
- All personnel should don appropriate Personal Protective Equipment (PPE) prior to cleaning the facility.
- Laboratory personnel should perform all daily housekeeping routines within the TB laboratories, including trash removal. Cleaning staff should only enter the laboratories under the supervision of the laboratory staff.
- All the cleaning and decontamination procedures in the TB containment laboratory should be performed only by trained laboratory staff.
- Work surfaces are decontaminated when work is finished, at the end of every workday, and immediately after any spill of viable material.
- Large equipment, such as incubators and centrifuges, will have inner and outer surfaces damp-wiped with disinfectant on a routine basis.
- Sinks in the laboratories should be cleaned and flushed with agent appropriate disinfectants
- The floor of the TB containment laboratory should be thoroughly and routinely wiped down with a suitable chemical decontaminant, and workspaces that do not get daily attention should be disinfected
- Solid waste should be decontaminated by autoclaving prior to removal from the facility and disposed off by authorized personnel
Unidirectional Flow of Cleaning
- There should be an effective separation of various sections and activities of the lab to prevent cross-contamination.
- Unidirectional flow of cleaning should be maintained in specific areas.
- Cleaning items, such as mops, buckets and brushes, used in dirty areas of the laboratory should never be used in the cleaner areas.
Good Laboratory Practices to Keep Laboratories Clean and Clutter-free
- Floors and work surfaces should be kept as free of clutter as possible.
- Materials should be stored in closed cupboards, where possible.
- Excess reagents should be boxed, labelled and stored in the storeroom.
- Check spill kit contents on a monthly basis. The fresh disinfectant must be prepared each week.
- Record in the 'Laboratory Cleaning and Maintenance Logbook'.
Resources
IPC practices required at a DMC
ContentDirect sputum microscopy performed at Designated Microscopy Centres (DMC) is a relatively low-risk activity as long as safe work practices are implemented properly.The following work practices are recommended to ensure that microscopy laboratory technicians are not exposed to aerosols from sputum specimens.
1. Administrative Control at DMC
- The layout and design of the DMCs should include natural ventilation, mechanical ventilation (exhaust fan) and unidirectional airflow.
- The sputum collection area should be separated from the laboratory.
- Provisions for biomedical waste management in deep burial pits, sharps pits or appropriate disposal via the health facility biomedical waste management system.
2. Environment Control at DMC
- Doors and windows should be kept open for air exchanges.
- Sputum must be collected in a well-ventilated area with direct sunlight. It should not be collected inside the laboratories, toilets, waiting rooms, reception rooms, or any other enclosed space.
3. Personnel Level Control at DMC
- Laboratory technicians should wear laboratory coats, gloves and masks when handling sputum containers and during smear preparation and staining.
- Smears should be prepared in a well-ventilated environment near an open flame.
- Work benches should be cleaned daily with disinfectants.
- Sputum containers, applicator/ broomsticks, and used slides should be disinfected with 5% Phenol overnight before discarding.
Resources
Question Answer 1 Answer 2 Answer 3 All Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Sputum specimens can be collected in toilets.
True False 2 Sputum must be collected in a well-ventilated area with direct sunlight. It should not be collected inside the laboratories, toilets, waiting rooms, reception rooms, or any other enclosed space. Yes Yes Roles of various stakeholders in IPC
ContentCommitment at national, state and district level are required to support and facilitate the implementation of Infection Prevention and Control (IPC) measures.
The important stakeholders in IPC include:
National Airborne Infection Control Committee (NAICC) has been constituted to provide for a multi-lateral national level coordinating body, to develop national guidelines on IPC, and provide technical guidance for their implementation, evaluation, and revisions.
Composition of NAICC
NAICC has representatives from Central TB Division, Medical college, State TB Programme representatives, Directorate General of Health Services, Central Design Bureau, National Institutes, Civil society representatives and other relevant agencies
A State Airborne Infection Control Committee (SAICC) should be established for adoption and integration of the national guidelines on airborne infection control in health care and other settings in the hospital infection control plans of various health care facilities in the states
Composition of SAICC
SAICC has representatives from Mission Director, National Rural Health Mission, Director Health Services (Nodal Officer), Director Medical Education and Research, State TB Officer, Project Director-SACS, State Task Force for Medical Colleges, Representative of IMA (State Body), Architects and Engineers from State PWD, Representative of State Pollution Control Board, NGO / CBO
The airborne infection control activities at the district level should be coordinated and undertaken by the Sub-Committee on Biomedical Waste Management / Infection Control (SC-BMW/IC) under the District Health Society (DHS). They should function under guidance and close coordination with the SAICC, State Health Society and with the TB Sub-Committee under DHS (NRHM).
Composition of SC-BMW/IC
SC-BMW/IC has representatives from Medical College / District Hospital, Representative of Pollution Control Board Office at the district, Director, Nursing Administration and Training or equivalent, Representative of IMA (Local Body) / NGO / CBO
The Hospital infection control committee (HICC) is an integral component of the IPC programme of the health care facility.
The main functions of HICC include:
1. Establish the IPC programme in the health care facility, develop action plan for strengthening IPC measures for the facility and individual units within the facility with priorities based on the risk assessment
2. Constitute an infection control team to oversee IPC implementation in the facility
3. Review and revise annually infection control guidelines with policies, recommendations and working protocols with standard precautions, hand hygiene, cleaning and decontamination, disinfection and sterilization as key components
4. Organize training programmes on recommendations of the guidelines and IPC practices for staff
5. Develop an antibiotic policy and antibiotic stewardship programme
6. Conduct surveillance of antimicrobial resistance, monitor trends in hospital acquired infections (HAI), investigate outbreaks of HAIs
7. Evaluate the effectiveness of interventions for IPC, analyze the surveillance data and identify at-risk patients. Take appropriate action and implement recommendations where necessary
8. Conduct audits and quality control of IPC activities, ensure compliance with recommendations
9. Help control environmental risks for infection by liaising with appropriate departments such as healthcare waste management, provision of safe water (testing of water sources), pharmacy, housekeeping services, laundry and kitchen services
Resources
Guidelines on Airborne Infection Control in Healthcare and Other Settings.
National Guidelines for Infection Prevention and Control in Healthcare Facilities (https://www.mohfw.gov.in/pdf/National%20Guidelines%20for%20IPC%20in%20H…)
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Who are the important stakeholders in Infection Prevention and Control?
National Airborne Infection Control Committee (NAICC)
State Airborne Infection Control Committee (SAICC)
Sub-Committee on Biomedical Waste Management/ Infection Control (SC-BMW/IC)
All of the above
4
Commitment at national: National Airborne Infection Control Committee (NAICC); state: State Airborne Infection Control Committee (SAICC); and district: Sub-Committee on Biomedical Waste Management / Infection Control (SC-BMW/IC) levels are required to support and facilitate the implementation of Infection Prevention and Control (IPC) measures.
Preparation of TB Lab Disinfectants
ContentDisinfectants used in lab settings include:
1% Sodium Hypochlorite
- Broad spectrum antimicrobial action
- Used to disinfect surfaces
- Used to disinfect infectious material and disposal of used Truenat consumables (reagent bottles, cartridges, tips, chips)
- Hazardous and corrosive, to be used with care
- Is highly alkaline so can corrode metal
- Waste soaked in Sodium Hypochlorite should not be discarded by autoclaving.
70% Alcohol
- Bactericidal action
- Used for surface decontamination only
- Highly inflammable; keep away from fire
- Used to disinfect biosafety cabinets, laboratory benches and surface of instruments.
5% Phenol
- Used for decontaminating Cartridge-based Nucleic Acid Amplification Testing (CBNAAT) equipment and single-use items like CBNAAT cartridges prior to disposal
- Highly irritating to the skin, eyes and mucous membranes.
Preparation of these disinfectants is described below.
Preparation of 1% Sodium Hypochlorite
- Use commercially available 4% sodium hypochlorite solution.
- Dilute with distilled water to prepare required amount of 1% sodium hypochlorite
- E.g.: To prepare 100 ml of 1% sodium hypochlorite: 75 ml distilled water plus 25 ml 4% sodium hypochlorite solution.
- Sodium hypochlorite solutions (domestic bleach) contain 50 g/l available chlorine, and should therefore be diluted to 1:50 or 1:10 in water to obtain the final concentrations of 1 g/l or 5 g/l when used as a general-purpose disinfectant for TB laboratories.
- To be prepared fresh.
Preparation of 70% Alcohol
- Use commercially available absolute alcohol.
- Dilute with distilled water to prepare the required amount of 70% alcohol
- E.g.: To prepare 100 ml of 70% alcohol: 70 ml absolute alcohol plus 30 ml distilled water.
Preparation of 5% Phenol
- Melt 5 g of phenol by heating it.
- Dissolve in 100 ml distilled water.
Video fileVideo : Preparation of TB Lab Disinfectants
Resources
-
CDST_LT: Airborne infection control
FullscreenAirborne Infection Control [AIC]
ContentMycobacterium tuberculosis is transmitted in airborne particles called droplet nuclei that are expelled when a person with pulmonary TB coughs, sneezes, shouts, or sings. People nearby may breathe in these bacteria and become infected.
Airborne infection control is essential to prevent the spread of TB within a health facility and other settings.
Hierarchy of Controls to Reduce Risk of Transmission of TB (see the Figure)

Figure: Hierarchy of controls to reduce risk of transmission of TB
Environmental factors that influence transmission of M. tuberculosis are elaborated in the table below.
Table: Environmental factors that influence the transmission of M. tuberculosis; Source: Tuberculosis Infection Control Factor Description Concentration of infectious bacilli The more bacilli in the air, the more probable that M. tuberculosis will be transmitted Space Exposure in small, enclosed spaces Ventilation Inadequate local or general ventilation that results in insufficient dilution or removal of infectious droplet nuclei Air circulation Recirculation of air containing infectious droplet nuclei Specimen handling Improper specimen handling procedures that generate infectious droplet nuclei Air pressure Positive air pressure in an infectious patient's room that causes M. tuberculosis organisms to flow to other areas Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control.
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The hierarchy of controls to reduce the risk of transmission of TB includes which of the following?
Environmental controls
Administrative controls
Personal protective equipment
All of the above
4
The hierarchy of controls to reduce the risk of transmission of TB includes administrative controls, environmental controls and the use of personal protective equipment.
Ventilation as an AIC Measure
ContentVentilation is defined as the supply/ distribution/ exchange or removal of air from spaces by mechanical or natural means.
Airflow is a natural process whenever there is change in temperature or pressure. Air keeps moving displacing the room air, and the time to replace the entire in-room air depends on the size of the room, the openings, and the presence of additional/mechanical force. This air-flow, also called ventilation, will allow the entry of outside air or clean recirculated air to remove extra heat, humidity and infectious aerosols from occupied spaces to meet health and comfort requirements.
When fresh air enters a room, it dilutes the concentration of particles in room air including aerosols responsible for the transmission of TB that can otherwise remain suspended in the air for significant periods of time.
Thus, ventilation is recognized as an important factor influencing the transmission of airborne diseases.
Types of Ventilation at Designated Microscopy Centres (DMCs)
1. Natural Ventilation (Figure below)
- Natural ventilation at DMCs is achieved by designing a laboratory layout that supports the unrestricted flow of natural air.
- Doors and windows should be kept open to bring in fresh air from outside.
- Opening windows and doors on opposite walls will also allow for cross ventilation.
- The placement of furniture, equipment, supplies etc. at DMCs should not block or restrict the opening of doors and windows.

Figure: Natural ventilation achieved by opening doors and windows or using mechanical ventilation using fans and an exhaust fan for air mixing and directional flow (A); the flow of natural air should not be restricted by blocking doors and windows (B); Cross ventilation is not adequate if there is only one entry point for outside air (C); Source: Tuberculosis and HIV Co-Management and Tuberculosis And Airborne Infection Control.
2. Mechanical Ventilation: When the movement of air is driven by a mechanical device, it is called mechanical ventilation.
- DMCs are equipped with fans and exhaust fans as the simplest means of mechanical ventilation for air circulation and directional flow of air. Exhaust fans fitted in windows/ ventilators exchange air from inside the laboratory to the outdoors.
- Ceiling fans/ tabletop fans/ pedestal fans have rotating blades to circulate air inside the room. Tabletop and pedestal fans can be positioned in the room to allow the directional flow of air.
3. Hybrid/ Mixed-mode Ventilation
- In hybrid/ mixed-mode ventilation exhaust and/or fans are used in DMCs in combination with natural ventilation to obtain adequate air dilution when sufficient airflow cannot be achieved by natural ventilation alone.
The table below compares the advantages and disadvantages of the different modes of ventilation.
Table: Summary of Advantages and Disadvantages of Different Types of Ventilation; Source: Guidelines on Airborne Infection Control in Healthcare and Other Settings.
Mechanical Ventilation
Natural Ventilation
Hybrid (mixed-mode) Ventilation
Advantages
Suitable for all climates and weather
Suitable for warm and temperate climates
Suitable for most climates and weather
More controlled and comfortable environment
Lower capital, operational, maintenance costs for simple implementations
Energy-saving relative to mechanical ventilation
Occupants have limited control to affect ventilation
Capable of achieving very high ventilation rates
More flexible
Disadvantages
Expensive to install and maintain
Easily affected by outdoor climate and occupants’ behaviour
May be more costly or difficult to design
Can fail to deliver required ventilation rates through faulty design, maintenance, or operation
May be difficult to plan, design, and predict performance
Noise from equipment
Reduced comfort level of occupants in extreme weather
Cannot achieve directional control of airflow, if required
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control, CDC.
- Tuberculosis and HIV Co-Management.
- Tuberculosis and Airborne Infection Control.
Question
Answer 1
Answer 2
Answer 3
All
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In mixed-mode ventilation, exhaust and/or fans are used in combination with natural ventilation.
True
False
1
In mixed-mode ventilation, exhaust and/or fans are used in combination with natural ventilation.
Yes
Yes
Administrative measures for AIC at a Health Facility
ContentThe administrative measures at a health care facility play an important role in preventing the spread of TB in health care settings. It includes Administrative controls for outpatient and inpatient settings
Administrative measures at Outpatient(OPD) settings
1. Screen for respiratory symptoms as early as possible upon patient’s arrival at the health care facility thereby reducing the overall stay of such patients in the healthcare facility- screening at registration counter itself by asking simple questions related to chronic respiratory symptoms, and those suspected to have TB can be prioritized for further management
- screening when patients are in waiting area- by volunteers/health staff
2. Provide patient education and counseling on cough hygiene and sputum disposal
- paramedical staff or volunteers should educate and reinforce cough etiquette while the patient is in the waiting area
- educate patients on availability of bins with disinfectants for disposal of sputum
- display of posters on cough hygiene and sputum disposal in the waiting areas
3. Segregate patients with respiratory symptoms
- having separate waiting area for chest symptomatics within the overall outpatient area
- implement a patient flow control mechanism so that screened chest symptomatics are diverted to special area rather than the common waiting area
- well ventilated waiting areas to reduce overall risk of airborne transmission
4. Fast-track patients with respiratory symptoms
- fast-track patients for clinical and laboratory evaluation
- fast track chest radiography and sputum examination with priority slips/referrals
Administrative measures at Inpatient (IPD) setting
1. Minimize hospitalization of TB patients- whenever possible, manage patients entirely as outpatients thereby avoiding hospitalization and the risk of exposing other patients and staff
2. Establish separate rooms, wards, or areas within wards for TB patients
- patients with TB should be physically separated in different rooms/wards from other patients so that others are not exposed to the infectious droplet nuclei
- separation of TB patients from vulnerable and immune-compromised patients is essential
3. Educate and counsel inpatients on cough hygiene and provide adequate sputum disposal
- educate and display posters on cough hygiene and safe disposal of sputum in bins with disinfectants
- provide masks to all admitted patients and educate on proper use of masks
4. Establish safe radiology procedures for TB patients
- schedule inpatient chest radiography for non-busy times
- provide priority service to minimize the length of time spent in the department
Resources
- Guidelines on Airborne Infection Control in Healthcare and Other Settings.
- Tuberculosis Infection Control.
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What of these is/are the administrative measures for airborne infection control at a health facility?
Prompt/ fast-track screening
Educating, training, and counselling
Availability of masks
All of the above
4
Administrative measures for airborne infection control at health facilities include prompt/ fast-track screening and diagnosis, education, training, and counselling, and availability of masks.
Yes
Yes
-
CDST_LT: Biomedical waste management
Fullscreencolor coding and type of container
ContentThe National TB Elimination Programme (NTEP) utilizes different coloured bags for the segregation of waste generated in TB laboratory settings as shown in the table below.
Table: Waste Segregated and Collected According to Colour-coded Bags
Yellow bag:
- Broomsticks
- Parafilm tape & plastic bag – contaminated with samples
- Löwenstein-Jensen (LJ) media without the bottle
- Microbial sample/ blood/ body fluids contaminated paper/ cotton/ swab
- Blood bags
- Microbiological cultures Truenat chips (MTB/ Rif)
- Used mask/ gowns
- Expired medicines/ drugs/ antibiotics
Red bag:
- Specimen collection tubes
- Sputum cups
- Cartridge Based Nucleic Acid Amplification Test (NAAT)/ Truenat cartridges
- Infected plastic
- Contaminated tips
- Pasteur pipettes
- Polymerase Chain Reaction (PCR) tubes
- Mycobacteria Growth Indicator Tube (MGIT) tubes
- Disposable LJ tubes
- Contaminated falcon tubes
- Used gloves
- Contaminated droppers
- Empty Cartridge-based Nucleic Acid Amplification Test (CBNAAT) reagent bottles

Blue bag:
Glass slide in Truenat machine and used microscopy slides. Slides should not be broken.
All these bags are to be labelled with the Biohazard logo (figure below) on them.
Figure: Biohazard Logo
- Waste generated in the Culture Drug Susceptibility Testing (CDST) laboratories is autoclaved prior to segregation in colour-coded bags.
- The biohazard materials are collected and handed over to handlers authorized by the pollution control board.
- Personnel handling/segregating biomedical wastes must use appropriate Personal Protective Equipment (PPE) and should be trained in spill management.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, 2021.
- Guidelines for Management of Healthcare Waste as per Biomedical Waste Management Rules, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
Disposing Off Contaminated Material Safely in DMC Laboratory Settings
ContentThe Laboratory Technician (LT) must safely discard contaminated, biohazard waste generated by tuberculosis (TB) laboratories. This waste must be discarded along with the overall waste of the health facility in which TB services are provided.
There are 2 types of waste generated from DMC laboratory settings:
- Sputum containers with specimen and wooden sticks
- Stained slides
Disposal of Sputum Cups with Left-over Specimen, Lids and Wooden Sticks
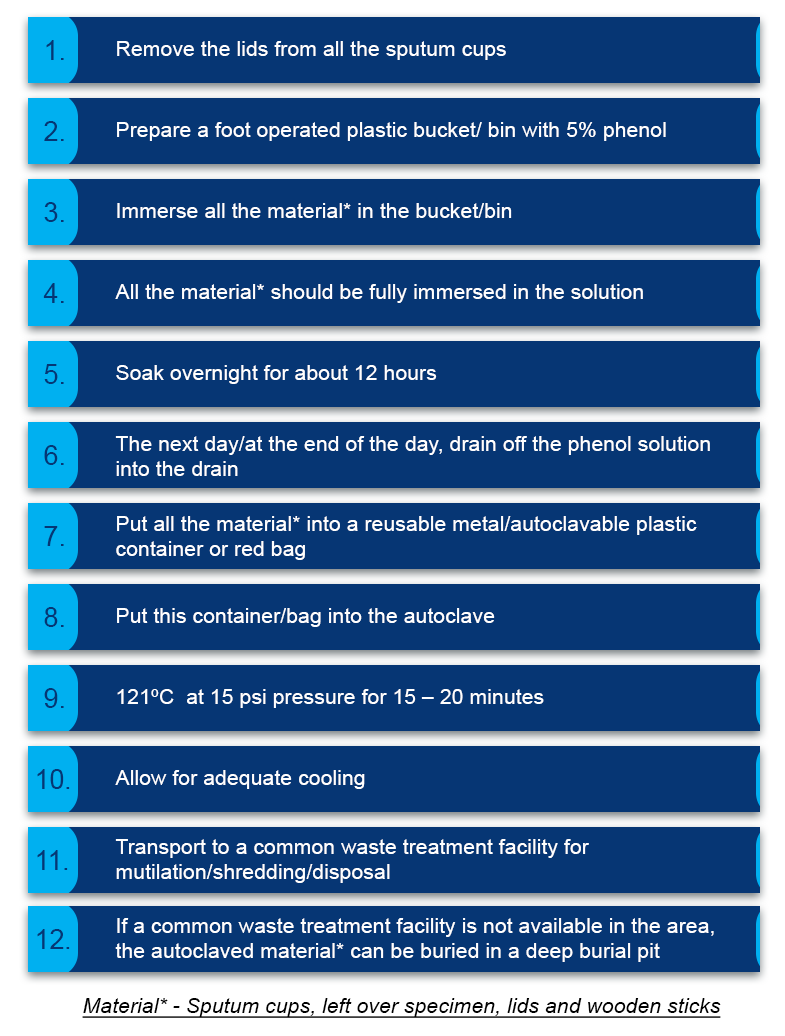
Figure 1: Steps for disposal of sputum cups with specimen, lids and wooden sticks
Important Points to Remember
- If autoclaving is not possible, boil in a pressure cooker of 7 litre capacity with water and submerge the contents for at least 20 minutes
- LTs and support staff handling biological waste need to wear gloves
- The red bag used for autoclaving must:
- Have a biohazard symbol
- Have adequate strength to withstand the load of the waste material
- Be made of non-PVC plastic material
Disposal of Stained Slides
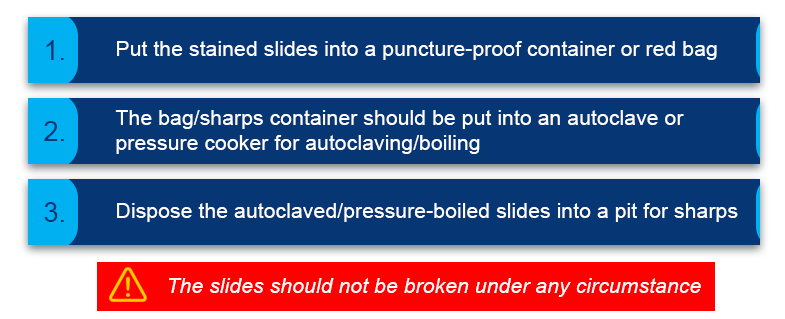
Figure 2: Steps for disposal of stained slides
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Mercury Spill in TB Lab Settings
ContentMercury is a harmful metal, and accidental spillage of mercury needs to be handled with care.
- Use of mercury thermometer should be avoided in the laboratory.
- A spill kit for mercury must be available if metallic mercury is present in the lab. The directions provided in the kit should be followed
- Spilled metallic mercury forms little spheres that roll into corners and cracks on the floor. If not completely cleaned up, mercury vapor will continue to be released into the air
- DO NOT use mercury thermometers in ovens. If the thermometer breaks, the heat will lead to dangerous concentrations of mercury in the air.
- Exercise additional caution, when placing or storing mercury thermometers to reduce the risk of breakage
- The Standard Operating Procedures (SOP) for Mercury Spill management should be displayed in TB laboratories
Handling Mercury Spill
Items needed:
- Apron
- Gloves
- Two cards/X-ray films
- Masks
- Powdered Sulphur (optional)
Cleaning the Spill
- Collect the mercury, using an index card or X-ray film, to form a pile or globule
- Mercury-absorbing powders, such as sulphur, can be used to amalgamate mercury
- Mercury waste and materials used in spill clean-up must be promptly placed in a sealed bottle
- Store metallic mercury in tightly closed, sturdy containers
- After all visible mercury has been collected, the area should be washed with a detergent solution, rinsed, and allowed to dry before use. This treatment should remove most remaining mercury residue
- Under no circumstances should mercury be swept with a broom or vacuumed with an ordinary vacuum cleaner. These procedures will disperse mercury more quickly into the air and spread the contamination
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Fullscreen
{kind=link}