-
DR-TB HIV Coordinator: General Concepts in ACSM
FullscreenAdvocacy Communication and Social Mobilisation
ContentAdvocacy refers to activities that seek to influence the influencers and decision-makers, so as to make TB more central as a public health agenda and enlist their (influencers’) support to create an enabling environment in support of the National TB Elimination Programme (NTEP) to eliminate TB. Advocacy fosters political will, increases financial and other resources on a sustainable basis, and holds authorities accountable to ensure that pledges are fulfilled and results achieved.
Communication is a process people use to exchange information about TB through media, including such channels of communication as mass media, mid-media, and Interpersonal Communication (IPC). Much of the communication effort on TB is concerned with transmitting a series of messages to the people affected by TB through mass media and mid-media, which are necessary but not sufficient. As ‘participation’ and ‘dialogue’ are necessary for effective communication, IPC occupies a place of vital importance. Communication aims to improve knowledge about TB and TB services and change attitudes and practices to encourage people to seek care and complete TB treatment.
Social mobilisation is the process of bringing together different stakeholders and building partnerships to prevent, detect, and cure TB. It targets different sections of the targeted population, say a village community, ward, or other small groupings, and raises awareness of and demand for the TB elimination program. The emphasis here is on community participation and involvement in TB case detection and cure.
Resources
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Placing TB higher on the political agenda of governments is an achievement of:
Advocacy
Coordination
IPC
None of the above
1
Advocacy is a broad set of coordinated efforts to place TB higher on the political agenda, strengthen government commitment to implement or improve TB-related policies and increase and sustain financial and other resources for TB.
Yes
Yes
What is A in ACSM
ContentIn ACSM, "A" stands for Advocacy. "Advocacy" is an activity by an individual or a group that aims to influence the decisions within political, economic and social institutions.
Advocacy focuses on influencing policy-makers, funders and international decision-making bodies through a variety of channels:
- Conferences, summits and symposia
- Celebrity spokespeople, press conferences, news coverage
- Meetings between various levels of government and civil society organizations
- Official Memoranda of Understanding (MoU), parliamentary debates and other political events
- Partnership meetings, patients’ organizations, private physicians, radio and television talk shows, and service providers.
Types of advocacy
- Policy advocacy: Mainly targets policy-setting, influencing policymakers to incorporate the latest evidence and informs senior politicians and administrators how an issue will affect the country, and outlines actions to take for improving the laws and policies.
- Programme advocacy: Targets opinion leaders at the community level on the need for local action.
- Media advocacy: Validates the relevance of a subject, puts issues on the public agenda and encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilization for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
News reports on World TB day celebrations are an example of which of the following types of advocacy?
Policy advocacy
Programme advocacy
Media advocacy
None of the above
3
Media advocacy encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Yes Yes What is C in ACSM
ContentCommunication aims to favourably change knowledge, attitudes and practices among various groups of people.
Types of communication in healthcare are:
- Oral/verbal communication- by word of mouth (speech/talk)
- Written communication- exchange of facts, ideas and opinions through the use of written materials
- Non verbal communication- through gestures, body language or posture, facial expressions, and eye contact
- Visual communication- exchange of ideas through visuals
Health communication aims to influence and empower individuals, populations and communities to make healthier choices. It frequently informs the public of the services that exist for diagnosis and treatment and relays a series of messages about the disease. It aims to inculcate behaviour change for healthy life choices.
E.g.: “Seek treatment if you have a cough for more than two weeks”, “TB hurts your lungs” or “TB is curable”.
Approaches to health communication
1. Informative communication
Provides information about a new idea and makes it familiar to people.
2.Educative communication
A new idea on health behaviour is explained, including its strengths and weaknesses.
3.Persuasive communication
Usually in the form of a message that promotes a positive change in behaviour and attitudes, and which encourages that audience to accept the new idea. This approach to message development involves finding out what most appeals to a particular audience. Persuasive approaches are more effective than coercive approaches in achieving behaviour change.
4.Prompting communication
Messages are designed so that they are not easily ignored or forgotten they can be used to remind the audience about something that reinforces earlier messages.
Behaviour Change Communication (BCC)
- Behaviour Change Communication (BCC) is an interactive process of any intervention with individuals, groups or communities to develop communication strategies to promote positive health behaviours which are appropriate to the current social conditions and thereby help the society to solve their pressing health problems.
- BCC creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
- It aims to change behaviour – such as persuading people with symptoms to seek treatment – and to foster social change, supporting processes in the community or elsewhere to spark a debate that may shift social mores and/or eliminate barriers to new behaviour.

Figure: Behaviour Change Communication
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What does the environment created by behaviour change communication encourage the TB-affected communities to do?
Discuss, debate, organize, communicate
Discuss, organize, implement, communicate
Organize, enforce, communicate
None of the above
1
Behaviour change communication creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
What is SM in ACSM
ContentSocial Mobilisation (SM) is the process of bringing together different stakeholders and building partnerships to prevent, detect and cure TB. It generates dialogue, negotiation and consensus among a range of players that includes decision-makers, the media, Non-government Organisations (NGOs), opinion leaders, policy-makers, the private sector, professional associations, TB-patient networks and religious groups.
At the heart of social mobilisation is the need to involve people who are either living with active TB or have suffered from it at some time in the past.
Aims of Social Mobilisation
• Increase awareness of the disease (TB) and the demand for diagnosis and treatment services
• Expand service delivery through community-based approaches
• Enhance sustainability, accountability and community ownership of TB services
Activities for Social Mobilisation
- Group and community meetings - Engaging yuva/ mahila mandals, village health sanitation and nutrition committees under the National Rural Health Mission (NRHM), sensitization of local and religious leaders on TB and related stigma in the community. Regular meetings at the village level to address myths and misconceptions and help people with TB symptoms seek timely and appropriate care or referrals.
- School activities - Conducting TB awareness campaigns in schools by addressing the school assembly/ class, painting competitions, rallies, road shows, essay competitions, drawing competitions, exhibitions, dramas, pictorial presentations, quizzes, puzzles, puppet shows, leaflet distributions etc.
- Traditional media group performances - Performing entertainment-centred folk performances, street plays with scripts centred around TB awareness messages.
- Rallies and road shows - Spreading TB related messages on World TB day.
- Home visits - Encouraging interpersonal communication and empowering former TB patients and TB champions to become Directly Observed Treatment, Short-course (DOTS) providers.
Here, inter-personal communication and group communication are the main channels of communication for disseminating TB-related key messages.
In the National TB Elimination Programme (NTEP), partner NGOs play an important role in social/ community mobilisation. It generates dialogue, negotiation and consensus, engaging a range of players in interrelated and complementary efforts while taking into account people’s needs.
Resources
- Advocacy,Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
A roadshow was conducted by local PHC in a village on World TB day with message to End TB. This is an example of:
Policy making
Social mobilisation
Institutional strengthening
Diagnostics
2
Roadshow is one of the activities of social mobilisation strategy which aims at increasing awareness about the disease, involving major stakeholders.
ACSM goals for TB Elimination
ContentAdvocacy, Communication and Social Mobilization (ACSM) strategies are directed at achieving specific goals in terms of TB elimination.
They are:
- Setting and developing the policy based on the latest evidence
- Mobilizing political commitment and resources for TB
- Improving case detection and treatment adherence
- Widening the reach of services
- Combating stigma and discrimination
- Empowering people affected by TB and the community at large
It is useful to determine how ‘ideal behaviour’ in the community relates to these goals. The ‘ideal behaviour’ which is promoted through messages and ACSM strategies should be connected to the overall goal of the TB control programme. A few examples of this are:
- For the general public: Going to a healthcare provider at the first signs of possible TB infection (ideal behaviour) relates directly to the National TB Elimination Programme (NTEP) goal of increasing the case-detection rate for TB.
- For healthcare providers: Following the standards set for the treatment of TB – includes knowing what regimen, how to administer anti-tubercular therapy and what treatment path to take in case of multidrug-resistant or extensively drug-resistant TB. This relates to treatment adherence and outcomes.
The ACSM goals are planned in such a way as to achieve/ address:
• Structural or systemic issues (such as the lack of community Direct Observation Treatment, Short-course (DOTS) programmes)
• Communication interventions (such as behaviour change)
• Individual and social barriers (such as stigma, risk perception and knowledge among populations and health staff)
• Social mobilization activities that promote changes throughout a community or priority group.
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilization for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Seeking healthcare at the earliest symptom of TB directly relates to which goal of NTEP?
Mobilizing political commitment and resources for TB
Improving case detection
Widening the reach of services
Combating stigma and discrimination
2
Improving case detection is an important goal of NTEP and seeking health care early helps in the detection of more number of cases.
Yes Yes Target Audience for ACSM activities
ContentIdentifying target audience is a key step in the process of developing Advocacy, Communication and Social Mobilisation (ACSM) strategy.
Specific target audience need to be addressed to prevent hinderances in achieving the programme objectives.
Image
Figure: Steps in Identifying Target Audience for ACSM Activities
Target Audience for ACSM Activities
-
Advocacy
• Decision-makers at national, regional and district levels (National Health Mission officials, District Magistrate, National TB Elimination Programme leadership)
• Policy-makers
• Professional groups
• Funders
• Media
-
Communication
• General public, including different vulnerable groups, healthcare workers (i.e., primary healthcare providers, Allopathic and Ayurvedic, Yoga and Naturopathy, Unani, Siddha and Homeopathy (AYUSH) doctors, private healthcare providers, traditional healers, etc.)
• TB patients currently on treatment as well as cured TB patients
• Contacts of patients with active TB
• People at high risk of developing TB
-
Social mobilisation
• Communities
• Community groups, e.g., mahila mandals, youth groups
• National and local level leaders
• Local Non-government Organisations (NGOs), Youth organizations, Community-based Organisations (CBOs)
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Identifying target audience is crucial in the process of developing ACMS strategy.
True False 1 Specific target audiences need to be addressed to remove the causes/ reasons that are hindering programme objectives.
-
ACSM approaches
ContentOnce Advocacy, Communication and Social Mobilisation (ACSM) objectives are designed, linking them with activities strengthens the overall programme effectiveness. Several ACSM approaches can be considered for TB. Decisions on which approach or combination of approaches to use should take into account the benefits and risks, the time frame and the expertise and financial resources needed for effective implementation.
There are two parameters to determine:
(1) What ACSM activities to conduct?
(2) Which channels of communication to use?
Following are the various ACSM approaches relevant to the National TB Elimination Programme (NTEP) and the activities included in it:
NTEP Goal
ACSM Approaches
Activities & Channels
Gaining political commitment to TB elimination
- Educate national policy-makers and political leaders about the health and economic benefits of TB elimination. Aim to have TB declared a national health priority.
- Educate local and community level authorities to encourage them to contribute to TB elimination efforts.
- Solicit the support of international and national partners.
- Seminars and briefing meetings
- Print information (letters, fact sheets)
- Events around World TB Day and other occasions
Improving case detection
- Raise public awareness about TB.
- Reduce stigma against people with TB and correct misconceptions about TB infection by actively involving current and former TB patients.
- Help health workers, communities and individuals identify TB cases.
- Encourage individuals to seek care from appropriate sources.
- Target hard-to-reach populations (prisoners, urban poor, homeless).
- Formative research to determine the best messages and approaches
- Mass media including radio and television
- Distribution of print materials at community meetings or events
- Interpersonal communication and counselling training for health workers
- Community mobilisation activities
Increasing treatment success and discouraging the spread of Multidrug-resistant TB (MDR-TB)
- Give people with TB hope of complete cure.
- Encourage people with TB to seek treatment from appropriate sources.
- Provide materials to counsellors.
- Encourage people with TB to complete treatment even if they improve before treatment ends.
- Make people with TB aware of possible side effects, and where to seek care, if present.
- Encourage health workers, family and community members to directly observe people with TB taking their medicine.
- Engage people who are fully recovered to encourage people currently affected by TB to complete treatment.
- Interpersonal communication and counselling training for health workers
- Mass media, including radio and television
- Extensive distribution of print materials at healthcare facilities
- Community mobilisation activities
- Peer education at community or interest group meetings
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI. 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Factors to be considered while adopting an ACSM approach include:
Risks & benefits
Time frame
Expertise & financial resources
All of the above
4
Decisions on which ACSM approach or combination of approaches to use should take into account the benefits and risks, the time frame and the expertise and financial resources needed for effective implementation.
Yes
Yes
Communication channels
ContentThere are several communication channels for the effective dissemination of messages.
Below are various channels with their advantages and disadvantages listed.
Channels/ Tools Audiences Reached Advantages Disadvantages Mass media channels Television Households, families - Wider reach in urban and rural areas
- Maximum impact due to audiovisual elements
- Expensive production costs
- Less reach among rural and migrant populations, who are vulnerable to TB.
Radio Individuals, households, families - Radio production is simple and much less expensive than TV.
- Relatively wider reach than TV among rural and migrant populations.
- Accessible even on mobile phones
- Radio listening is no more popular; TV viewing/online portals are more popular.
Newspapers
and
magazines
Educated
individuals,
households
- Timely and fixed schedule of dissemination.
- Pictorial description of message.
- Not useful for the illiterate population
- People read newspapers for news about political developments, crime, etc., and not for advertisements per se, unless the advertisement is attractive and eye-catching enough.
Mid-Media - Outdoor Publicity Materials and Folk Arts/ Dramas Posters Individuals - Strong pictorial description of the message.
- Useful in high-traffic areas
- Brief messages
- Short lifespan
Pamphlets Individual - Good for communicating core messages with illustration/ visual support.
- Mass distribution and a kind of take-home message.
- Not very expensive.
- Can be used for repeated exposure and to reinforce messages broadcasted through mass media.
- Useful for the literate population, but can be used by the illiterate people as well
- If the pamphlet looks attractive enough, it is taken home and contents are deciphered with the help of literates or children at home/ in the neighbourhood.
Brochures Individuals, groups - Detailed information/ instructions with illustrations/ visuals/ graphs etc.
- Production costs may be relatively high.
Flip charts Individuals - Good support in counselling sessions.
- Production costs may be relatively high.
Wall writings/ hoardings Individuals, households - Useful in high-traffic areas.
- Good for identification, pictorial description and reinforcement of message
- Only for the literate population.
- Message retention is low
Kiosks Individuals - Face-to-face communication along with audio-visual communication for better message retention.
- Useful in dispelling myths and practices.
- Expensive to scale up.
- Requires trained staff.
- Relatively small reach.
Mobile vans and videos on wheels Groups, community - Entertaining and can grab audience attention and better message retention
- Expensive to implement and scale up
- Relatively small reach
- Requires precision of timing
Folk dramas Groups, community - Entertaining and can grab audience attention and better message retention
- Can touch an emotional chord with individuals/ households; useful for sensitisation.
- Relatively small reach.
- Expensive to scale up.
- Requires precision of timing.
- Requires good artists with prior training.
Interpersonal Communication (IPC) Counselling Individuals - Credible source due to face-to-face communication.
- Allows detailed explanation of key health messages.
- Can help dispel myths and check wrong practices.
- Time-taking to build reach.
- Small reach (individual).
- Costly to scale up.
- Requires special training.
Home visits Households - Credible source due to face-to-face communication.
- Allows detailed explanation of key health messages.
- Can help dispel myths and check wrong practices.
- Useful for rapport building.
- Time-taking to build reach.
- Small reach to the target audience.
- Requires adequate capacity building.
Community Dialogue Seminars, workshops, and Parliament questions Policy-makers, implementers, urban population - Brainstorming of key stakeholders.
- Identification of key communication challenges,
- Key inputs from experts and academicians.
- Not timely.
- High cost of implementation.
- Time-taking to bring about change.
- Difficulty in mobilizing key stakeholders.
Public meetings and gatherings Key
influencers,
individuals,
households
- Emphasis on key messages by influencers/ stakeholders.
- Useful for addressing different segments of the target audience together.
- Intermittent in occurrence.
- High organising cost.
- Only verbal communication involved.
- Reach is relatively small.
Working with groups Households,
individuals
- Dissemination of key messages among communities.
- Word-of-mouth communication.
- Low frequency.
- Only verbal communication involved.
Social Media Facebook, Blogs, YouTube, SMS Individuals - Targets individuals but has a wide/ mass reach.
- An effective method of reaching a large number.
- High visibility among decision-makers.
- Only limited people have access to internet accounts on Facebook, and an even smaller number have blogs.
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Home visits for communication are an example of: Mass media Interpersonal communication Community dialogue Mid-media approach 2 A home visit is a form of Interpersonal Communication (IPC).
- Credible source due to face-to face communication
- Allows detailed explanation of key health messages
- Can help dispel myths and check wrong practices
- Useful for rapport building
Yes Yes ACSM activities at different levels
ContentAdvocacy, Communication and Social Mobilization (ACSM) activities must place the individual at the centre and bring in the family, community and society to bring about sustained changes in TB perceptions and behaviours. ACSM activities must target these 4 groups accordingly:
- Individual: Specific interventions that ensure sustained engagement of people or individuals in maintaining positive behaviours/ changing to desired behaviours. E.g., counselling, use of positive TB messages, message by TB champions, etc.
- Family: Interventions that create an enabling environment for promoting positive behaviour change and developing necessary skills for a person affected by TB. E.g., counselling of the entire family.
- Community: Mobilizes groups toward a common goal, raises local resources and fosters support and awareness for TB-related issues. E.g., conducting TB awareness campaigns in public meeting places, melas, street dramas, etc.
- Society: Advocates for rights-based and socially inclusive approaches and seek support for the TB programme. E.g., workshops and seminars to drive change in legislation, policy, partnerships and resource allocation.
Aimed at individuals, families, communities, and the society, varied ACSM activities are undertaken at the national, state, district and community levels to:
- Create awareness and an enabling environment
- Build capacities to bring about desired changes in TB-related health behaviour
- Sustain positive behaviour
These are shown in the figure below.

Figure: ACSM Activities Spanning Across All Levels
Resources
- Operational Handbook on Advocacy, Communication, and Social Mobilization (ACSM), NTEP, 2014.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACSM activities span across which levels? Individual only. Individual, family, community, society and from central down to the village level. Individual and family levels only. ACSM activities do not span across any level. 2 ACSM activities must span across the individual, family, community, societal levels, and from the central down to the village level. Community Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
Strategies of Community Engagement in NTEP
Content- Scaling up community participation in the National TB Elimination Programme through community-led activities and working with various community groups, especially TB survivors and key populations
- Empower TB survivors and affected populations to act as mentor’s/change agents and build their capacity for engaging them in programme planning, implementation and monitoring
- Working with community stakeholders to aid in early case identification amongst the vulnerable population
- Increasing accountability of the service delivery system through community participation
District TB Forum
ContentThe district TB forum is a community-engagement modality that aims to empower and engage the TB-affected community. Constituted by TB patients (cured or on treatment), community leaders, government officials, experts and NGOs; it gives a voice to the affected community and advocates with the programme managers for the resolution of challenges faced by TB patients in accessing TB services.
District TB forum is composed of various stakeholders as shown in the table below and its meeting is to be convened at least every 6 months at the district level.
Table: Composition of the District TB Forum
Chairperson District Magistrate Co-Chairperson Chief Executive Officer, Zilla Parishad Members - District Development Officer
- Chief Medical/ Health Officer
- WHO Representative – TB Consultant
- Representative of Tuberculosis Association of India
- Pulmonologist and Professor of Community Medicine of Medical Colleges
- District President, Indian Medical Association
- Two representatives of reputed local NGOs/CSOs on a rotation basis
- Representative from NTEP partners on a rotation basis (REACH/ UNION/ CHAI/ PATH/ FIND/ WHP/ KHPT)
- Five TB patient representatives (past TB patients/ family members)
- Representative of district-level PLHIV Network
- Representative Officer from RCH who manages NGOs
- District TB Officer
- PRI member (Zilla Parishad/ BDC/ Panchayat)
- Journalist
- Advocate
- Representative of the corporate sector
Abbr: WHO: World Health Organisation; NGOs/CSOs: Non-governmental and Civil Society Organisations; NTEP: National TB Elimination Programme; WHP: World Health Partners, PLHIV: People Living with HIV; RCH: Reproductive Child Health; PRI: Panchayati Raj Institutions; BDC: Block Development Council Functions of the District TB Forum
- To advise on strategies for engaging communities affected by TB and increasing community participation in TB programs by forming a network of people affected by TB.
- To periodically review the progress of community involvement and network of people affected by TB.
- Highlight the concerns and needs of TB patients, and work with the government and a broad range of individuals/ organisations to develop better and more responsive health services.
- Advocate for greater and more equitable access to quality, accurate and independent information for patients. To focus on reducing health inequalities by campaigning for patients to have the right to be involved in decision-making.
- Enable dialogue between all stakeholders involved in a TB patient’s care such as government (including local self-government), medical and paramedical associations, industry, medical insurance companies, private healthcare providers and diagnostic centres.
- Create and manage resources to sustain and accelerate TB prevention, control, care and treatment services through community engagement and a network of people affected by TB.
- Facilitate nutritional support, linkages with social welfare schemes, and rehabilitation of TB patients.
- Perform grievance redressal.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Concerning the district TB forum, which of the following is true? It is involved in engaging communities affected by TB at the state level. It is chaired by the person affected by TB. It has only 3 stakeholders. It convenes meetings biannually. 4 The district TB forum engages communities affected by TB at the district level is chaired by district magistrates, convenes meetings biannually, and comprises of various stakeholders. Yes Yes Local Self Government [LSG]
ContentLocal Self Government is the management of local affairs by local bodies who have been elected by the local people.
-
The local self-Government includes both rural and urban government.
Image
Figure 1: Types of local self government
Rural Local Governments:
-
Panchayati Raj Institution (PRI) is a system of rural local self-government in India. PRI was constitutionalized through the 73rd Constitutional Amendment Act, 1992. The panchayat raj system in the entire country is not the same but, by and large, structure of LSG in most of the States have the three-tier structure:
Image
Figure 2: Structure of Panchayati Raj
Urban Local Governments:
-
An urban area is usually a compact and densely populated area. All types of urban local governments are democratically elected by the people based on electoral wards.
-
Municipal administration is necessary to provide basic civic facilities like water supply, drainage, garbage disposal, public health, primary education, construction, and maintenance.
Image
Figure 3: Types of Urban local bodies
- Other types of urban local governments in India - Notified Area Committee, Town Area Committee, Cantonment Board, township, Port trust, Special purpose agency.
Role of Local Self Government in Health.
-
The common departments in the LSGs are General Administration, Finance, Public Works, Agriculture, Health, Education, Social Welfare, Information Technology, and others. Thus, LSG could play an important role in addressing the determinants of health.
-
LSGs play an active role in preventive healthcare services like vaccination, controlling drinking water and foods, mother-child health, disease screening programs, sanitation precautions, controlling of wastes and animal diseases, controlling of environmental factors that have disease risks such as air and water pollution. They are seen as critical to the planning, implementation, and monitoring of the NHM. Implementation of the NHM in achieving its outcomes is significantly dependent on well-functioning gram, block and district level panchayats.
-
LSGs also deliver services toward health promotion.
-
The other services provided by the LSGs are: Emergency and ambulance services, rehabilitation centers, elderly care centers and home care services
-
ASHA/USHA is one of the important functionary in health care service delivery and selected by the Gram Panchayat.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
The fundamental objective of Panchayati Raj system is to ensure which among the following?
1. People’s participation in development
2. Political accountability
3. Democratic decentralisation
4. Financial mobilisation
1,2,3
2,3
1,4
1,3
4
Panchayat Raj Institution (PRI) was constitutionalised to build democracy at the grassroots level and was entrusted with the task of rural development in the country. Active participation and vigilance on the part of the rural public is a must for the sustenance of democratic de-centralisation.
-
Role of LSG in TB Elimination
ContentLocal Self Governance is the management of local affairs by local bodies who have been elected by the local people. There are 2 types of Local Self Government (LSG): panchayats in rural areas and municipalities in urban areas. Local self-government (LSG) has deep connections and linkages with local people. Role of LSG in Tuberculosis (TB) elimination includes:
Image
Fig 1: Role of Local Self Government in TB Elimination
-
Awareness generation activities
With the participation of Panchayati Raj Institution (PRI) members in rural areas and municipalities in urban areas following awareness generation activities can be carried out:
- Health education on symptoms of TB, good cough etiquettes, available services for screening, diagnosis and treatment of TB, patient support/benefit schemes, TB in vulnerable groups (children, pregnant women, diabetic patients, patients on immunosuppressants, alcoholics and smokers) with emphasis on periodic screening for TB.
- Observance of World Tuberculosis Day on March 24
- Organize health-checkup camps and talks with the TB survivors
- Sensitize Panchayat Raj Institutions (PRI) members, faith leaders etc.
- Organize anti-stigma and non-discrimination campaigns
- Advocacy interventions
Local administration or Panchayat Raj Institutions (PRI) can be engaged in advocacy interventions to promote healthy behaviours and leverage support of TB patients:
- To install spitting bins.
- To install signages on good cough etiquettes.
- Free distribution of masks/handkerchief/tissues to TB patients in the community.
- Services for case finding (Active and latent TB Infection)
With the help of LSGs outreach activity can be planned and undertaken by community/non-governmental organizations (NGO) volunteers, Accredited Social Health Activist (ASHA) and Multi-Purpose Worker (MPW-Male)/ Auxiliary Nurse Midwife (ANM) under the supervision of the Community Health Officer (CHO)/Medical Officer- Urban Primary Health Centre (MO-UPHC), for case finding. These activities include:
- Vulnerability assessment
- Screening for symptoms of TB using Community Based Assessment Checklist (CBAC)
- Periodic active case finding among identified vulnerable populations
- Prompt referral of persons with TB symptoms to health center
- Treatment support and monitoring
- Local self governments can engage in formation and conducting meetings of treatment support groups.
- Health education for TB patients and their household contacts can be conducted on TB symptoms, treatment, managing adverse drug reactions, nutrition during house visits and treatment support group meetings.
- Counselling for TB patients and caregivers can be organised by PRI members and local administration.
- LSGs can mobilise funds from philanthropists to support the TB Patients, to supplement and augment healthcare facilities, screening and testing requirements, buying diagnostics and any other resources that might be required.
- TB preventive measures
- Under supervision of LSGs screening can be conducted of household/workplace contacts and other contacts of TB patients as eligible in the local context and identified vulnerable population for TB/latent TB infection.
- LSG can promote airborne infection control at workplaces and community settings.
- Interventions to ensure community participation
- LSGs can participate in identifying and training TB Champions and facilitate their participation in Village Health Sanitation Nutrition Committees (VHSNCs), Mahila Arogya Samitis (MASs), Jan Arogya Samitis and TB forum meetings.
- VHSNCs and MASs can discuss TB related issues in their meetings, conduct awareness programmes and extend support to case finding and treatment.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India 2020
- Pradhan Mantri Khanij Kshetra Kalyan Yojana (PMKKKY), Ministry of Mines, Government of India, 2015.
- Training Modules (5-9) for Programme Managers and Medical Officers, Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Local self-government can help in identifying and mapping socially and clinically vulnerable groups using available data from Municipal/ Block/ Taluka/ Zila Panchayats' records. Periodic drives can be conducted by them to identify and trace cases and link them to services provided under National Tuberculosis Elimination Programme (NTEP) and other social schemes.
True
False
1
Media advocacy by local self-government can engage the local media to disseminate information. With strategic communication and social mobilisation through Local self-government, the community members will help in gaining awareness about the services available in NTEP as well as other social schemes.
-
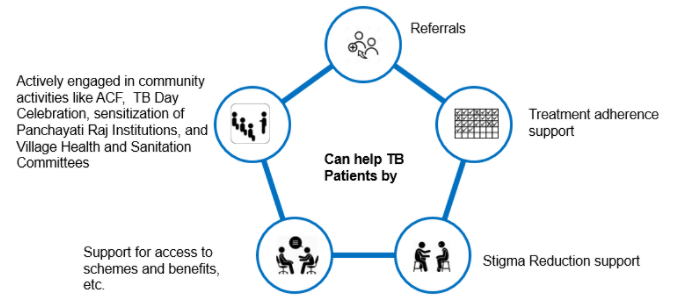
TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
Patient-provider meetings
ContentPatient-provider meetings are important to ensure patient support and improve case holding/ treatment adherence.
Objective: To orient the patients on the course of the treatment, the importance of adherence and the risk for close contact. It also provides a platform to discuss the difficulty in following treatment courses by the patients and the need for further counselling if required.
Purpose: The purpose of this meeting is to counsel patients in a group who are on treatment or who are about to begin treatment. This is an opportunity for free interaction between providers and patients and also an opportunity for patients to clarify their doubts, if any.
Facilitators: These meetings are organized by the treatment supporter/ Directly Observed Treatment (DOT) provider. The Senior Treatment Supervisor (STS)/ Medical Officer (MO) are to conduct these meetings.
Target Group: Patients on treatment or who are about to begin treatment. There could be 5-10 patients (minimum) in such meetings. (If there is a large number of patients at one centre, small groups of about 10 patients may be made so that better interaction takes place between patients and providers).
Participants: Block medical officer/ Medical Officer - TB Control (MO-TC), field staff (STS, TB Health Visitor (TBHV), Senior TB Lab Supervisor (STLS)), general health system staff, patients and their attendees.
Place: These meetings are to be organized at the health facility.
Duration and Frequency: These meetings can be organized once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility.
- Each meeting can be for half-hour to one hour.
- The patient may be provided refreshments (tea, snacks etc.)
Note: Patient-provider interaction meetings are additional to, and are different from, interpersonal communication that the provider has with the patient while administering treatment.
Messages to be Provided to Patients
- Basic information about tuberculosis, cough etiquette, etc.
- Importance of completing treatment
- Side-effects of drugs and how to manage these
- Importance of follow-up sputum examination
- Prophylaxis for children in the family
- Do’s and don’ts including protective measures, the role of a nutritious diet, etc.
Health Communication Materials: Flip book, banner, posters on TB, etc., are to be provided and used during these meetings.
Report Writing: At the end of each meeting, a report may be prepared to state the date and time of meetings, number of patients, name of facilitators, presence of MO in the meeting, topics covered/ main points discussed in the meeting, along with major concerns mentioned by the patients.
- The report is to be prepared by the STS.
- The list of patients who attended the meeting may be attached to the report.
- It may be more convenient to have a register at each centre for such meetings, and patients can write their names in the same register.
- These may be submitted by STS to the MO-TC on a monthly basis for onward submission to the District TB Officer (DTO) to be included in the quarterly Performance Monitoring Report (PMR).
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Technical and Operational Guidelines for Tuberculosis Control, RNTCP, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How often should patient-provider meetings be conducted? Everyday Twice a year Once every month Once a year 3 Patient-provider meetings can be organised once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility. Yes Yes
-
DR-TB HIV Coordinator: Social Inclusion and wellness activities
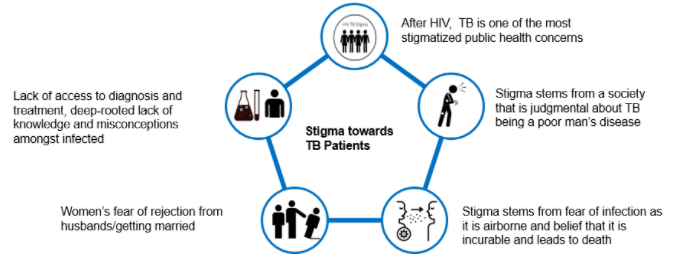
FullscreenStigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Patients' charter for TB care
ContentThe Patients’ Charter for Tuberculosis Care (the Charter) outlines the rights and responsibilities of people with TB. It empowers people affected by TB and their communities through this knowledge. Initiated and developed by persons affected by TB from around the world, the Charter makes the relationship with healthcare providers a mutually beneficial one.
The Charter sets out ways in which people affected by TB, the community, health providers (both private and public), and governments can work as partners in a positive and open relationship with a view to improve TB care and enhance the effectiveness of the healthcare process.
It allows for all parties to be held more accountable to each other, fostering mutual interaction and a positive partnership.
Principles of the Patients’ Charter for TB Care
- The charter practices the principle of Greater Involvement of People with TB (GIPT).
- This affirms that the empowerment of people with the disease is the catalyst for effective collaboration with health providers and authorities and is essential to victory in the fight to end TB.
Parts of the Patients’ Charter for TB Care
There are two main parts in the patients’ charter for TB care which cover:
- Patients’ rights
- Patients’ responsibilities
These parts are further delineated in Tables 1 and 2 below.
Table 1: Patient's Rights According to the Patient's Charter for TB Care Rights Explanation of rights: You, as the patient, have the right to: Care - Free and equitable TB quality care meeting the International Standards of Tuberculosis Care (ISTC)
- Benefit from community-care programmes
Dignity - Be treated with respect and dignity
- Social support of the family, community and national programmes
Information - Information about available care services — be informed about condition and treatment, know drug names, dosage and side-effects
- Access your medical records in the local language
- Have peer support and voluntary counselling
Choice - A second medical opinion, with access to medical records
- Refuse surgery if drug treatment is at all possible
- Refuse to participate in research studies
Confidence - Have your privacy, culture and religious beliefs respected
- Keep your health conditions confidential
- Care in facilities that practice effective infection control
Justice - File a complaint about care, and have a response
- Appeal unjust decisions to a higher authority
- Vote for accountable local and national patient representatives
Organization - Join or organise peer support groups, clubs and Non-governmental Organisations (NGOs)
- Participate in policy-making in TB programmes
Security - Job security, from diagnosis through to cure
- Food coupons or supplements, if required
- Access to quality-assured drugs and diagnostics
Table 2: Patients' Responsibilities According to the Patients' Charter for TB Care Responsibilities Explanation of responsibilities: You, the patient, have the responsibility to: Share information - Inform healthcare staff all about your condition
- Tell staff about your contacts with family, friends, etc.
- Inform family and friends and share your TB knowledge
Contribute to community health - Encourage others to be tested for TB if they show symptoms
- Be considerate of care providers and other patients
- Assist family and neighbours to complete treatment
Follow treatment - Follow the prescribed plan of treatment
- Tell staff of any difficulties with treatment
Solidarity - Show solidarity with all other patients
- Empower yourself and your community
- Join the fight against TB in your country
Resources
- The Patients’ Charter for Tuberculosis Care, The Global Plan to Stop TB 2006-2015.
- Capacity-building of Affected Communities for Accelerated Response to Drug-resistant Tuberculosis in the South-east Asia Region, WHO, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test According to the Patients' Charter for TB Care, it is not the patient’s responsibility to support other patients. True False 2 According to the Patients' Charter for TB Care, patients have a responsibility to support other patients, show solidarity and empower their communities. Yes Yes
Fullscreen