-
STLS: Concepts in TB Treatment
FullscreenGoals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Strategies for TB Treatment
ContentUnder the National TB Elimination Programme (NTEP), strategies adopted in the treatment of TB are based on the available scientific and operational researches. These strategies are combined to ensure better treatment outcomes for the TB patients. The main strategies include:
Domiciliary Treatment
- This is a strategy that allows for the treatment of TB in a patient’s home.
- Domiciliary chemotherapy proved to be as effective as sanatoria treatment (which was the historical way of treating TB) and achieved higher cure rates.
- The patients having the social benefits of being at home.
Short Course Chemotherapy (SCC)
- Chemotherapy of TB underwent revolutionary changes in the 70s owing to the availability of two well-tolerated and highly effective drugs – rifampicin and pyrazinamide.
- These drugs allowed for SCC and made it possible to simplify treatment and reduce its duration without reducing the therapeutic effect.
- Now with SCC regimens, it is possible to treat and cure TB patients in 6 months.
- When given daily, these regimens are effective, achieve high cure rates, prevent the emergence of drug resistance and minimize relapses.
- The shorter duration also contributes to improvement in treatment adherence.
Directly Observed Treatment (DOT)
DOT is a method whereby a trained healthcare worker or another trained designated person (treatment supporter) watches a patient swallow each dose of anti-TB drugs and document it.
- DOT can reduce the development of drug resistance, treatment failure, or relapse after the end of treatment.
- Many patients who do not receive directly observed treatment stop taking drugs once they feel better.
- Hence, by providing DOT, the NTEP ensures that patients receive the right drugs, in the right doses, at the right intervals and for the right duration.
The modern treatment strategy is based on standardized short-course chemotherapy regimens largely administered on a domiciliary basis, utilising the DOTS strategy and proper case management to ensure completion of treatment and cure.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Treatment of Tuberculosis Disease, CDC, 2006.
- Guide on Tuberculosis Control for Primary Health Care Providers, WHO, 2015.
- Treatment of Tuberculosis: Guidelines for National Programmes, WHO, 2003.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these treatment strategies are adopted by NTEP?
Domiciliary treatment
Use of short-course chemotherapy
Directly observed treatment
All of the above
4
Strategies utilized by NTEP in TB treatment are domiciliary, short-course chemotherapeutic short-course regimens that are directly observed.
Pharmacological Basis of treatment
ContentTuberculosis treatment and its different regimens have scientific backgrounds for their formulations. To understand this, we need to know about the mode of action of each anti-TB drug first.
Mode of Action of Anti-TB Drugs
Anti-TB drugs have the following three actions:
- Early bactericidal activity: Killing of actively growing bacilli (in the phase of rapid multiplication and uninhibited metabolic activity).
- Sterilizing activity of persisting bacilli, i.e., metabolically inhibited organisms in a quasi-dormant state.
- Ability to prevent the emergence of drug resistance.
The ranking of first-line drugs with respect to their type of activity is indicated in Table 1 below.
Table 1: Ranking of first-line anti-TB drugs used in the treatment of drug-sensitive TB, based on the mode of action and activity
First-line Drugs Early Bactericidal Sterilizing Prevention of emergence of drug resistance Isoniazid (H) ++++ ++ ++++ Rifampicin (R) +++ ++++ +++ Pyrazinamide (Z) ++ +++ + Ethambutol (E) + Nil ++ Thus, each drug has unique characteristics and drug combinations will make the regimen more effective.
Need for Long Duration of Treatment of TB
- Anti-TB drugs mostly kill actively multiplying tubercle bacilli.
- When bacilli have low metabolic activity, i.e., when bacterial growth has almost come to a standstill and the organisms are “dormant”, they are not killed by otherwise bactericidal drugs. Such organisms are referred to as persisters*.
- Though they may survive in the presence of drugs, behaving as if they were drug-resistant, they are in fact susceptible to the drugs.
- Thus, if for some reason these organisms regain their ability to multiply freely, they would be killed by the very drugs that had not harmed them before.
- When dormant bacilli again become metabolically active and start multiplying during effective chemotherapy, they are soon killed.
- Once chemotherapy has been completed, the revived bacilli may continue to multiply and thus cause relapse.
- This explains why conventional chemotherapy needs to be of long duration.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the role of the intensive phase of anti-TB treatment? To reduce adverse drug reactions in patients To achieve rapid killing of actively multiplying bacillary population
To prevent the emergence of drug-resistance Options 2 and 3 4 The role of IP is to achieve rapid killing of actively multiplying bacillary population and eliminate naturally occurring drug-resistant mutants and prevent the further emergence of drug resistance. Yes Yes Which of the following drugs is bacteriostatic? Isoniazid Ethambutol Pyrazinamide Rifampicin 2 Ethambutol is an effective bacteriostatic drug, helpful in preventing the emergence of resistance to other companion drugs. Yes Yes Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentIt is extremely important for any type of TB patient to be initiated on the right treatment at the earliest in order to have better treatment outcomes. Therefore as soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen.
Steps in TB Treatment Initiation
Image
Figure: Flowchart-Treatment Initiation
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, India, 2021.
- Training Modules (1-4) for Programme Managers and Medical Officers, CTD, MoHFW, India.
Assessment
Question
Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. True False 1 The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. Yes Yes As soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen
True False 1 Soon after identification pre treatment counselling is given to patient and caregivers followed by pre treatment evaluation and treatment initiation. Yes Yes Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
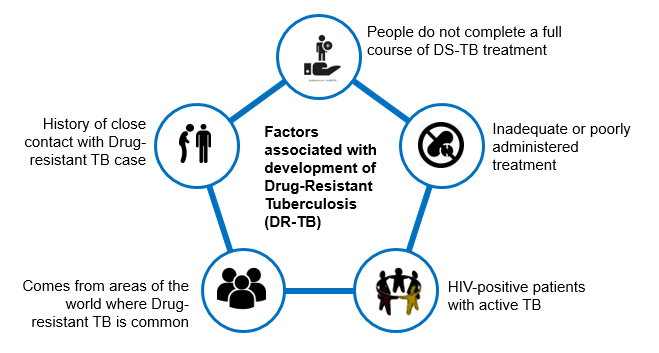
Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
-
STLS: Adverse Drug Reactions with anti-TB Drugs
FullscreenAdverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Pharmacovigilance in NTEP
ContentPharmacovigilance is defined by the World Health Organisation (WHO) as the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problem.
- It is a fundamental public health surveillance activity to ensure patient safety measures in healthcare.
- Good pharmacovigilance will identify the risks within the shortest possible time after medicines have been marketed and help establish or identify risk factors.
Importance of Pharmacovigilance
Pharmacovigilance allows for intelligent, evidence-based prescribing with the potential for preventing many Adverse Drug Reactions (ADRs). Pharmacovigilance will help in:
- Improving patient care by assessing both the harms and benefits received from drugs (anti-tubercular treatment).
- Strengthening patient safety, safeguarding the patient’s interests and ensuring adherence to prescribed drug regimens.
- Preventing antimicrobial resistance.
Pharmacovigilance ultimately helps each patient in receiving optimum therapy at a lower cost to the health system.
Conducting Pharmacovigilance under the National TB Elimination Programme (NTEP)
The Pharmacovigilance Programme of India (PvPI) was set up by the Ministry of Health and Family Welfare, Govt. of India, in July 2010. PvPI is India’s national programme for surveillance of ADR-related information.
NTEP in collaboration with PvPI, and with support from WHO India, developed the comprehensive active Drug Safety Monitoring and Management (aDSM) system for ADR monitoring. Pharmacovigilance is prioritised in Drug-resistant TB (DR-TB) centres for drug-resistant cases.
Adverse events reporting for pharmacovigilance is done as follows:
- DR-TB centres are linked with ADR Monitoring Centres (AMC) established in medical colleges to initiate reporting of ADR in a systematic manner.
- Serious adverse events are reported to AMCs and Central TB Division (CTD) within 24 hours. This is done via a standardized suspected ADR reporting form (Annexure-11) which is filled by the treating doctor.
- The data is entered in Nikshay on a regular basis by statistical assistants at the nodal DR-TB centre and senior DR-TB TB-HIV supervisors at the district DR-TB centre.
- From Nikshay, the information is directly communicated to PvPI through a connecting bridge called Vigiflow.
- The ADR data submitted to Vigifloware is analysed by PvPI and shared with CTD on a regular basis.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Ready Reckoner for Medical Officer - Adverse Drug Reactions Associated with Anti-TB Drugs Identification and Management, 2019.
- Practical Handbook on the Pharmacovigilance of Medicines used in the Treatment of Tuberculosis, WHO, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is true concerning pharmacovigilance in NTEP?
PvPI is India’s national programme for surveillance of ADR-related information.
ADR-related information flows between Nikshay and PvPI via Vigiflow.
Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
All of the above
4
PvPI is India’s national programme for surveillance of ADR-related information, which flows between Nikshay and PvPI via Vigiflow. Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
Yes Yes
-
STLS: Documentation of Treatment
FullscreenTB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
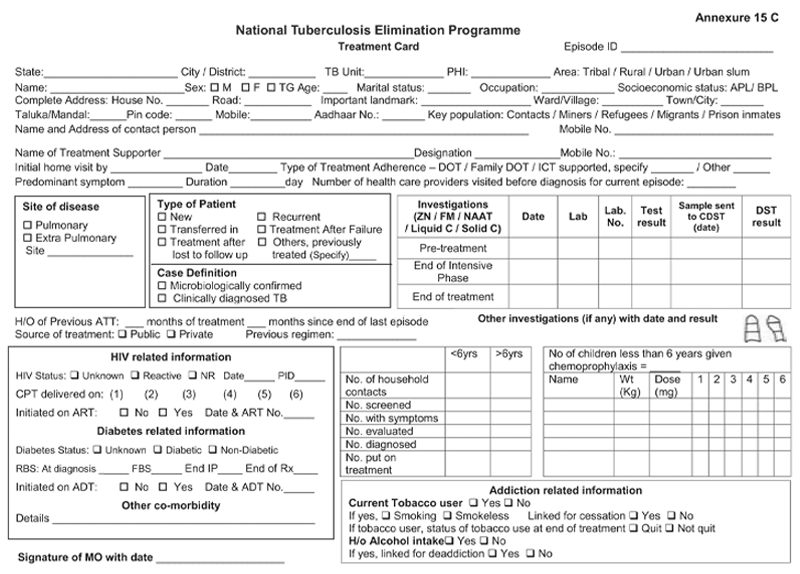
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
NTEP TB ID Card
ContentIn the National TB Elimination Programme (NTEP), the ‘NTEP TB identity card’ is provided for their identification and record of clinical follow-ups.
The identity card is completed for each patient who has a Tuberculosis (TB) Treatment Card, and it is kept with the patient. Information from the TB Treatment Card is used to complete the identity card.
There are 3 parts in the NTEP TB identity card and details in each part is delineated in Table 1.
Table 1: Parts of the NTEP TB identity card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PART
DETAILS CONTAINED IN THE SECTION
The First and Second Part
Patient information
Name and address of the TB unit/ district
Treatment details of the patient including:
- Disease classification
- Type of patient
- Treatment provider
- Case definition
- Weight bands
- Dosage
- Sputum results
- Culture results
- Results of follow-up smear examinations
- Results of follow-up cultures
- Information on the date of treatment initiation
- Treatment outcome
The Back Part
Appointment dates for visits to NTEP facilities
Contact details of NTEP staff in case of side events/queries
The information contained in this card will help to continue treatment in case the patient is transferred or admitted to any other health facility any time during the treatment period. The TB identity card is shown in Figure 1.
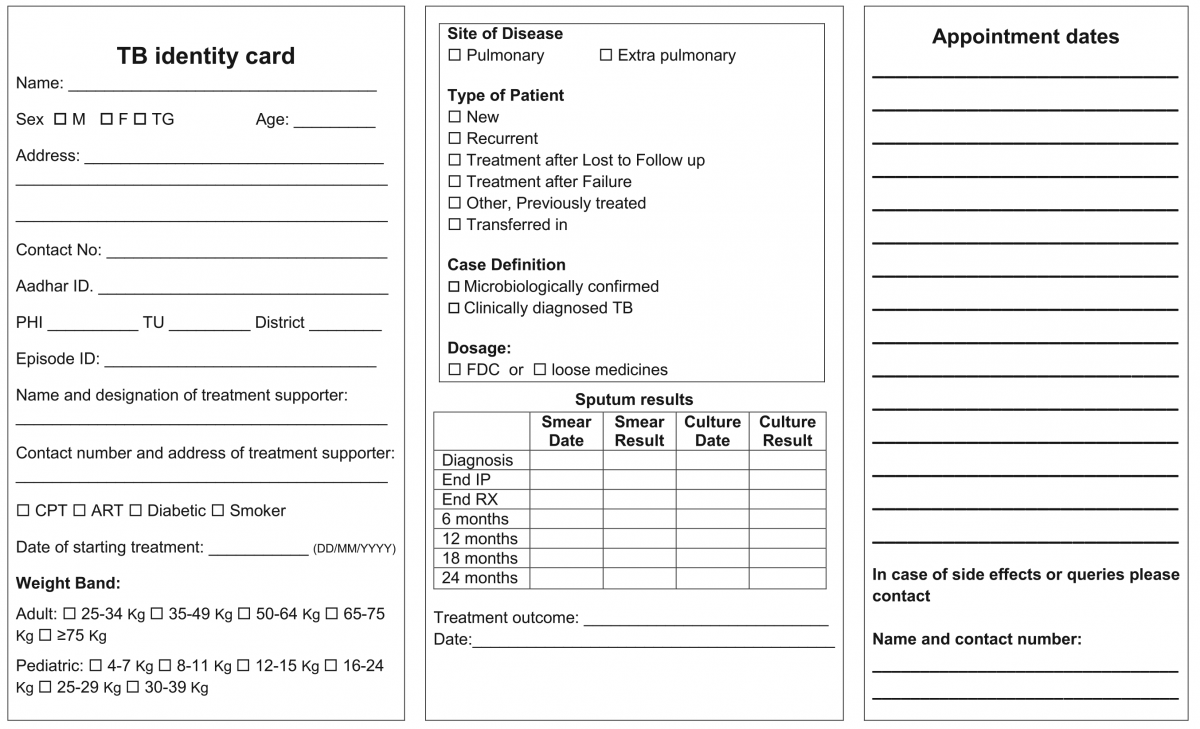
Figure 1: NTEP TB Identity Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020

Figure 2: Sample of a patient’s TB identity card


Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
-
STLS: Extra Pulmonary TB (EPTB)
FullscreenManagement of EPTB
ContentThe management principles of Extrapulmonary Tuberculosis (EPTB) are shown in the figure below.

Figure: Ten principles about what every EPTB patient in India needs as a basic standard of care
Abbr: CBNAAT:Cartridge-based Nucleic Acid AMplification Test; PTB: Pulmonary TB; NTEP: National TB Elimination Programme
Diagnosis of EP-TB
- All efforts need to be made to get a microbiological confirmation whenever a sample is available.
- Clinical diagnosis can be made by treating physician based on the clinical features, lab investigations, imaging studies and by ruling out other causes
Treatment Regimen and Duration for EPTB
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE). However, the duration of the continuation phase in EPTB may be extended in special situations such as TB Meningitis, bone and spine TB etc.
Role of Surgery in EPTB Cases
- Surgery is sometimes required for the diagnosis of EPTB. It is reserved for management of late complications of the disease.
Monitoring Treatment Response
- Response to treatment in EPTB may be best assessed clinically. Clinical follow-up is the most important criterion for the follow-up of EPTB patients. The clinician can assess the patient’s condition by checking weight gain and a decrease/ increase in presenting clinical symptoms.
- Investigations such as Acid-fast Bacilli (AFB) microscopy, chest X-ray, liver function tests, serum creatinine, and USG-abdomen can be used to monitor the treatment status.
The treatment support and other monitoring activities remain the same as for pulmonary TB.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Index TB Guidelines on Extra-pulmonary Tuberculosis for India, Central TB Division, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the standard treatment duration for most EPTB cases?
2 weeks
1 month
6 months
3 years
3
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE).
Yes Yes In which cases can the treatment duration exceed 6 months in EPTB?
TB meningitis
TB of the bone and joint
Depending on the clinician’s decision
All of the above
4
EPTB treatment duration can be extended beyond 6 months in TB meningitis, TB of bone and joint (including TB otitis media), and if recommended by the clinician.
Yes
Yes
-
STLS: Drug Sensitive TB (DS-TB)
FullscreenCategorization of DSTB Treatment Regimen
ContentDaily Regimen is prescribed for Drug Sensitive TB patients (DSTB), where the patient needs to consume the FDC formulation daily.
Daily Regimen comprises the first line Anti TB drugs based on
- Age: Adult/ Pediatric
- Weight of the patient: Weight Bands
Age: Based on age, patients are categorized into
- Adults: The patient's age should be greater than 19 years
- Paediatrics: Patient's age up to 19 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosages are based on TB patients’ weight.
- A weight band category is defined for Adults and Pediatric patients separately, and FDC are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
DS-TB Treatment – Patient Flow
ContentCommunity Health Volunteers(CHVs) have to refer the presumptive cases identified based on the r symptom screening to the nearest NTEP health facility for further investigation. Once Diagnosed with TB, the TB patients are initiated on the first-line TB treatment. Patients are also offered NAAT within a maximum of 15 days to rule out any drug resistance. If no drug resistance is detected, then the patient continues on the first-line TB treatment. TB patients are then clinically evaluated every month to check the progress of TB treatment.
The treatment duration of TB is divided into two phases - The Intensive Phase(IP) and the Continuation Phase(CP). Post-treatment completion, patients are then evaluated at intervals of 6,12,18 and 24 Months to ensure a relapse-free TB cure for the patient.
Figure: DSTB Treatment Flow
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
-
STLS: Drug Resistant TB (DR-TB)
FullscreenDrug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Screening for DR-TB
ContentAll patients diagnosed with TB should have universal access to rapid DST for at least Rifampicin and further DST for at least Fluoroquinolones among all TB patients with rifampicin resistance, i.e. UDST.
UDST tests are offered preferably before treatment initiation to a maximum within 15 days from diagnosis. Based on the UDST test result, if Rifampicin resistance is detected, the patient is shifted to DR-TB Treatment Regimen. If Rifampicin resistance is not detected, then first-line anti TB treatment is continued, and the patient is screened further on their follow-ups. If tested positive in sputum examination during any patient follow up, then sputum is sent for further drug resistance testing, and the patient is referred to PHI for follow-up.
Figure: Screening of patient for initiating DRTB Treatment from DSTB Treatment
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
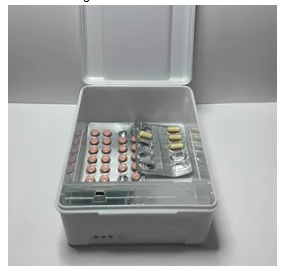
Figure: Patient wise boxes(PWB) for DRTB Treatment
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
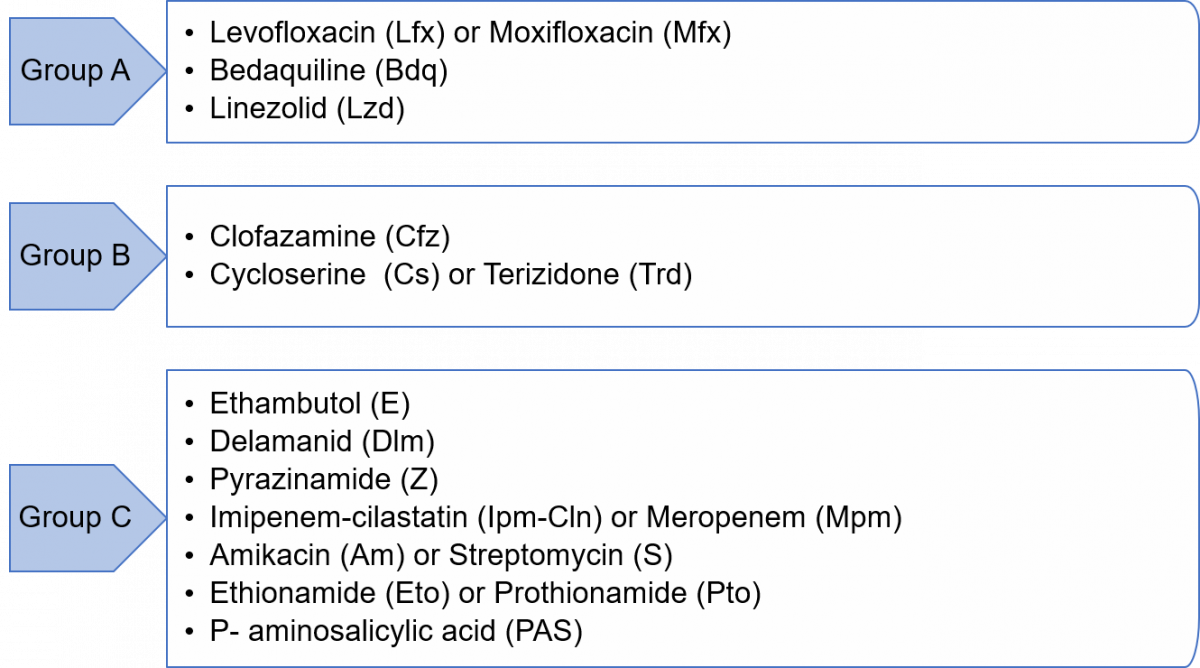
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
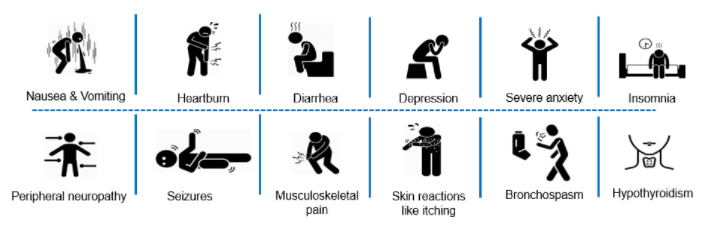
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
-
STLS: Follow up of TB patients
FullscreenFollow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
Management of Patients with Treatment Interruptions
ContentTreatment interruption is defined as a patient-initiated episode in which the patient discontinues TB treatment. All efforts must be made to ensure that TB patients do not interrupt treatment or are not lost to follow-up. Action should be taken to promptly retrieve patients who fail to come for their daily dose by the treatment supporter
The management of treatment interruptions is made based on the following criteria:
i. Type of case: Whether new, relapse or failure
ii. Duration of treatment taken: Less than one month/ more than one month. This helps in assessing the risk of the presence of drug resistance.
iii. Duration of Interruption: Less than one month/ more than a month.
If treatment interruption is more than one month, the outcome is declared as ‘lost to follow up’.
If a patient returns to the health facility after interrupting treatment for more than one month, the patient sample needs to be subjected to Drug Susceptibility Testing (DST) to determine resistance/ sensitivity status to anti-TB drugs.
In case the interruption is for less than one month, the same treatment regimen is completed to complete all doses.
Modes of Retrieval
TB treatment is supervised by a trained treatment supporter (a health worker, family member or community volunteer). The residential address is verified for all TB patients by home visits. However, in case of treatment interruption, patient retrieval action is required.
Retrieval can be done by the following modes:
1. Retrieval of patients interrupting treatment within 24 hours of discontinuation is done by the Treatment Supporter (TS) or Accredited Social Health Activist (ASHA)/ Auxilliary Nurse Midwife (ANM)/ Multipurpose Worker (MPW). The reason for interruptions should be reviewed carefully and efforts made to counsel and bring the patient back for treatment.
2. If the TS is not successful in retrieving such patients, it should be reported to the next higher level of supervisors, like Senior Treatment Supervisor (STS), and they should take all efforts to counsel and retrieve the patient.
3. If the patient interrupts treatment on more than one occasion, the Medical Officer of the Peripheral Health Institute (MO-PHI) should visit the patient’s home. The MO-PHI should give intensive counselling to the patient and may provide additional support to continue the treatment without interruption.
4. Innovative use of information and communication technologies for treatment adherence monitoring through 99 DOTS, Medication Event Reminder Monitor (MERM), etc. are also beneficial in finding missed doses and initiating retrieval action by the health staff.
Resources
1. Training Modules (1-4) for Programme Managers and Medical Officers.
2. Guidelines for PMDT in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. True False 1 If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. Yes Yes
-
STLS: Adherence monitoring
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
-
STLS: Treatment Support
FullscreenTreatment Support
ContentA person affected by TB requires support throughout the course of treatment and beyond that. The support to a TB patient is essential to ensure that s/he completes the treatment without affecting her/his quality of life (QoL). Keeping the patient as the central figure in the continuum of care, and ensuring social and personal circumstances are supportive (not only meeting immediate requirements of medical treatment) is the key to treatment support.

Figure: Key Components of Treatment Support
Resources
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, 2017.
A Patient-centred Approach to TB Care, WHO, 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
DOT is the only treatment support provided to TB patients.
True
False
2
Ensuring social and personal circumstances are supportive for treatment adherence and not just medical requirement is the key to treatment support.
Treatment Support Plan
ContentIn order to achieve TB treatment success, a good treatment support plan for the patients is essential. The National TB Elimination Programme (NTEP) recommends developing a treatment support plan for each patient at the time of treatment initiation. A holistic Treatment Support Plan (TSP) must include the following:
1) Treatment Supporter (TS) for each patient
- A Treatment Supporter (TS) who is acceptable and accessible to the patient and accountable to the health system (healthcare worker/ community volunteer/ private practitioner/ family member) identified in mutual consultation with the patient and provider during pre-treatment evaluation.
- The assigned TS should be able to receive training on drug administration, adherence monitoring, Adverse Drug Reaction (ADR) referrals etc., and perform these functions.
2) Periodic review of patient’s treatment
- Treatment Initiation counselling and monthly or need-based (in high TB burden areas) follow-up counselling to all TB patients and their family members must be included through staff who have expertise in the same, to address both bio-medical and psycho-social issues that could impact treatment.
- The TSP must also include a protocol for the field monitoring staff to capture each instance of treatment interruption and Adverse Drug Reactions, so that they can be effectively addressed before the patient turns lost to follow-up.
3) Psychosocial Support to TB patients and their families
- Counselling to the patients experiencing stigma, discrimination, marital/family discords, substance users etc. by the trained staff, and appropriate referrals for psychiatric ,de-addiction support etc. should be offered whenever required.
- The focus should be on observing, identifying and capturing above mentioned factors during treatment initiation as well as in each follow up visit.
- Home visit follow ups with consent from the patients must also be included in the TSP which may allow for better understanding and management of psycho-social issues.
- As an extension of TSP, community engagement activities which includes key persons such as politicians, religious leaders, self-help groups, TB champions etc by the TB staff is recommended to raise awareness and sensitise the communities about TB and also articulate a whole-of-society approach to ending TB.
4) Referral linkages for needy TB patients - to central and state government’s various social welfare and protection schemes and additional nutrition support services
- With the aim to eliminate catastrophic expenditure due to TB, the Government of India (GoI) has insisted on linking TB patients and households to the applicable government social welfare and protection schemes.
- The treatment supporters and the health systems staff who are in regular contact with the patients (Senior Treatment Supervisors, TB Health Visitors, District Programme Supervisors) should be trained in referral linkages so as to enable further support to the patients and their family members to avail the benefits under schemes.
- The GoI has rolled out a Direct Beneficiary Transfer (DBT) mechanism to support TB patients' nutrition (Ni-kshay Poshan Yojana) and travel during treatment whereas several state governments have also initiated certain state-specific schemes for TB patients across the country.
- Further as a part of patients treatment support, the GoI has initiated the ‘Nikshay Mitra’ campaign under the ‘Pradhan Mantri TB Mukth Bharat Abhiyan’ where in persons/companies/societies can adopt an entire block/ward to provide nutrition support to TB patients for a specific treatment period.
5) Treatment Completion Counselling
The TSP must include an end of treatment counselling for all patients, on the importance of post treatment follow ups and holistic self-care approach for leading an overall healthy life and also the ability to focus on life after TB treatment completion.
Resource- Training Modules (1-4) for Programme Managers & Medical Officers, NTEP, 2020.
- National Strategic Plan for Tuberculosis Elimination 2017-2025, RNTCP, 2017.
- Pradhan Mantri TB Mukt Bharat Abhiyaan - Guidance Document, CTD, India, 2022.
Assessment
Question Answer 1 Answer 2 Answer3 Answer 4 Correct Answer Correct explanation Only health workers can become treatment supporters for a TB patient. True False 2 Factors like acceptability, accessibility to the patient, and accountability to the health are taken into consideration when a treatment supporter is identified, and family members can also be treatment supporters and provided training by a health worker. Referral linkages for needy TB patients - to central and state government’s various social welfare and protection schemes and additional nutrition support services is part of holistic Treatment Support Plan (TSP)
True False 1 With the aim to eliminate catastrophic expenditure due to TB, the Government of India (GoI) has insisted on linking TB patients and households to the applicable government social welfare and protection schemes. Treatment supporter to TB Patient
ContentA Treatment Supporter can be any person such as a Medical Officer, MPWs, community volunteers working with the program etc. Even a patient’s relative or family member can be a Treatment Supporter.
As per NTEP guidelines, salaried NTEP/General Health System staff may also be assigned as treatment supporters for a patient. However, they will not be eligible for any honorarium.
A patient can only be linked to one treatment supporter at a time in Nikshay.
Assigning a TS
ContentAt treatment initiation a suitable Treatment Supporter has to be identified and assigned to the Patient.
How to identify a Treatment supporter for a patient
- The Treatment Supporter has to be acceptable and accessible to the patient and accountable to the health system.
- Should be identified in mutual consultation with the patient and provider, during pre-treatment evaluation.
- The Treatment Supporter can either be a healthcare worker, community worker/ volunteer, private practitioner or family member.
- Should be able to receive training on drug administration, adherence monitoring, ADR referrals etc., and perform these functions.
Assigning a Treatment Supporter to a Patient
Once the Treatment Supporter is identified, the patient records (Ni-kshay & treatment card) have to be updated by assigning the treatment supporter (prior registration in Ni-kshay is a pre-requisite) to the patient. See the steps below to assign a Treatment Supporter to the episode of a patient.
Treatment Supporters are eligible to receive the Treatment Supporters Honorarium as a Direct Benefit Transfer. However, to receive the DBT he/she should not be a salaried government employee.
NOTE:
- Only one Treatment Supporter can be assigned to an episode with status "OnTreatment" of the patient
- Treatment Supporters can be assigned by both the current PHI/ TU user.
- If required, a Treatment Supporter can be removed/ replaced by another Treatment Supporter anytime during the treatment.
Image
Figure: Steps to Assign a Treatment Supporter in Ni-kshay
Image
Figure: Screenshot Assigning a Treatment Supporter in Ni-kshay
Resources
- Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, Central TB Division, Ministry of Health & Family Welfare, India, 2021.
- Training Modules (5-9) for Programme Managers and Medical Officers, Central TB Division, Ministry of Health & Family Welfare, India, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test When should a treatment supporter be identified assigned to a patient episode ? While declaring treatment outcomes Any time while the patient is on treatment At treatment initiation When the patient is transferred 2 Treatment Supporters are to be identified and assigned to a patient at the time of treatment initiation.
Treatment Supporters can be assigned or re-assigned anytime during treatment, but this is in-case it has not been assigned before
Yes Yes A TB-HV acting as a Treatment Supporter can receive the Treatment Supporters Honorarium. TRUE FALSE 2 TB HV is a Salaried Government Employee and hence cannot receive the Treatment Supporters Honorarium. Yes Yes To assign a Treatment Supporter to a patient, which of the following are True? The Treatment Supporter needs to be registered on Ni-kshay The Treatment Supporter should be acceptable to the patient Should be able to record and monitor adherence, ADR, administer drugs, refer to the nearest Health Facility All of the above 4 Treatment Supporter needs to fulfill all the mentioned criteria. Role of TS
Treatment Support Groups
ContentTreatment Support Groups play an important role in providing treatment support to TB patients. It has been envisioned as a non-statutory body of socially responsible citizens and volunteers to provide social support to TB patients. This group goes beyond just providing treatment-related support as it also helps the community in accessing information, free and quality services and linkage to social welfare programmes without compromising confidentiality and respecting the dignity of the patient.
A good treatment support group creates a conducive environment for TB patients to access complete care without experiencing stigma and incurring out-of-pocket expenditures.

Figure: Schematic representation of the concept of treatment support groups.
Treatment Support Group (TSG): Example from Kerala
The initiative in the Pathanamthitta district of Kerala demonstrated that treatment support groups helped in minimising the loss-to-follow-up cases and better treatment outcomes. The group supported the patients in accessing information, free and quality services and social welfare programmes, thereby empowering the patients to complete the treatment successfully.
Resources
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, 2017.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation What is a treatment support group? A group of treatment supporters in the community A group of TB patients in the community A non-statutory body of citizens and volunteers to provide social support to TB patients All of the above 3 A treatment support group is a non-statutory body of citizens and volunteers to provide social support to TB patients. Nutritional Support
ContentNutrition constitutes an important part of TB Treatment. Undernutrition increases the risk of Tuberculosis (TB), and in turn, TB can lead to malnutrition. It has been demonstrated that undernutrition is a risk factor for progression from TB infection to active TB disease, and undernutrition at the time of diagnosis of active TB is a predictor of increased risk of death and TB relapse. There is, as yet, little evidence showing that additional nutrition support improves TB-specific outcomes, but low body mass index, as well as lack of adequate weight gain during TB treatment, are associated with an increased risk of TB relapse and death.
The following table illustrates the effect of undernutrition on outcomes in TB.
Effects on disease
- Increased severity of disease
- Increased risk of death
Effects on treatment
- Delayed sputum conversion
- Risk factor for drug-induced hepatotoxicity
- Malabsorption of rifampicin
- Reversion of positive cultures in Multidrug-resistant (MDR) -TB
Effects on long-term outcomes
- Increased rate of relapse
Effects on contacts
- Increased incidence in undernourished contacts
The basic recommendations to address the nutritional needs of TB patients are discussed below.
- Conducting an initial nutrition assessment of TB patients with further monitoring
- Providing ongoing counselling for patients on their nutritional status; Diet for TB patients starting treatment should include: cereals (maize, rice, sorghum, millets, etc.), pulses (peas, beans, lentils, etc.), oil, sugar, salt, animal products (canned fish, beef and cheese, dried fish), and dried skimmed milk
- Managing severe acute malnutrition according to national guidelines and WHO recommendations
- Managing moderate undernutrition for TB patients who fail to regain normal Body Mass Index (BMI) after two months of TB treatment or appear to lose weight during TB treatment and evaluating for proper treatment adherence and other comorbidities. If indicated, these patients should be provided with locally available nutrient-rich or fortified supplementary foods.
- Special categories of TB patients, such as:
- Children who are less than 5 years of age should be managed as any other children with moderate undernutrition.
- Pregnant women with active TB and patients with MDR-TB should be provided with locally available nutrient-rich or fortified supplementary foods.
6. Micronutrient supplementation for all pregnant women as well as lactating women with active TB. These women should be provided with iron and folic acid and other vitamin and minerals to complement their maternal micronutrient needs. In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
To achieve the above objectives, the guidelines for nutrition for TB patients are available and a mobile application (N-TB) is available for decision-making on nutritional support for TB patients.
Improving nutritional status at a population level is important for TB prevention which should be part of broader actions on social determinants. All efforts should be made to link TB patients for nutritional support which can be done through the existing public distribution system, local self-government or Non-governmental Organisations (NGOs)or donor agencies or through the corporate sector under Corporate Social Responsibility (CSR).
Resources
- Guideline: Nutritional Care and Support for Patients with Tuberculosis, WHO, 2013.
- Guidance Document: Nutritional Care and Support for Patients with Tuberculosis in India, MoHFW, WHO, CTD, 2017.
- Training Modules (1-4) For Programme Managers & Medical Officer NTEP, CTD, WHO, MoHFW, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, MoHFW, WHO, 2021.
Assessment
Question 1
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Page id
Part of Pre-Test
Part of Post-Test
Undernutrition doesn’t affect the outcomes of TB.
True
False
2
Undernutrition affects the outcomes of TB in terms of treatment.
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Support for deaddiction
ContentSubstance use has been one of the major reasons for non-adherence to TB treatment and therefore, the National TB Elimination Programme (NTEP) has implemented several initiatives for control and de-addiction of substance use in association with various other health programmes like the National Tobacco Control Programme (NTCP), Drug De-Addiction Programme (DDAP), etc.
NTEP has also included referral services to de-addiction facilities for TB patients as a part of the ‘Standards for TB Care in India (STCI)'.
Deaddiction Services and Linkages
- Brief substance use counselling during the pre-treatment, treatment initiation and regular follow-up counselling sessions by the trained NTEP staff.
- Referral to National Tobacco Quitline provides telephonic counselling via the toll-free number in English and Hindi languages 8 a.m. to 8 p.m. between Tuesday to Sunday.
- Referral to mCessation Programme provides evidence-based behavioural change Short Text Messages (SMSs) in English and Hindi languages on mobile phones, which include health information on tobacco use hazards, tips on quitting, and encouragement for those attempting to do so.
- Referral to nearest Tobacco cessation clinics/ centres in the government facilities.
- Referral under the Drug De-Addiction Programme (DDAP) wherein affordable, easily accessible and evidence-based treatment for all substance use disorders are provided through the government health care facilities of the Ministry of Health and Family Welfare, viz., All India Institute of Medical Sciences (AIIMS), New Delhi; Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh; National Institute of Mental Health and Neuro-Sciences (NIMHANS), Bengaluru; Dr Ram Manohar Lohia (RML) Hospital, New Delhi; AIIMS, Bhubaneswar; and Central Institute of Psychiatry (CIP), Ranchi.
Resources
- National Strategic Plan 2017-2025 for TB Elimination in India, MoHFW, India, 2017.
- National Framework for Joint TB-tobacco Collaborative Activities, MoHFW, India, 2017.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What service does the National Tobacco Quitline provide?
Telephonic counselling
Face-to-face counselling
None of the above
Both 1 & 2
1
National Tobacco Quitline: Telephonic counselling via the toll-free number in English and Hindi languages.
Yes
Yes
Support for Rehabitilation
Travel support for TB Patient
ContentEliminating the catastrophic expenditure on TB patients and their families has been an important goal of the World Health Organisation's (WHO’s) END TB strategy.
The National TB Elimination Programme (NTEP) has also attempted the same through various partnerships and one of the action plans under this strategy was to provide transport allowance to cover the TB treatment-related travel costs of the TB patients as well as their attendants.
Travel cost for Drug-resistant TB (DR-TB) patients
- Travel costs are reimbursed for DR-TB patients travelling to District or Nodal DR-TB Centre for initiation/ follow-ups/ adverse reaction management during the treatment, along with one accompanying person/ attendant.
- The reimbursement is as per actual cost per visit through public transport with a limit of up to Rs. 400 per visit within the district and up to Rs. 1000 per visit for outside district travel.
Travel cost for TB Patients in tribal/ hilly/ difficult areas
- TB Patients from tribal /hilly/difficult areas are provided with an aggregate amount of Rs. 750 as transport allowance to cover patients and the attendants' travel costs.
- Rs. 750 as a one-time payment at the time of notification.
Travel cost for Presumptive TB patients to visit District TB Centres (DTC)/ collection centres for testing
- Presumptive TB patients travelling to DTC/ collection centre are reimbursed as per actual cost with public transport.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
- Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme. Central TB Division, Ministry of Health & Family Welfare, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How much amount is provided as transport allowance to tribal/ hilly area patients and their attendants during their TB treatment
Rs.250
Rs.500
Rs.750
Rs.1000
3
Rs. 750 is provided as transport allowance to Tribal/ hilly area patients and their attendants during their TB treatment.
Yes
Yes
Linkages to Social Welfare Schemes
ContentThe government of India introduced Direct Benefit Transfer (DBT) to ensure that the benefits and subsidies are reaching the beneficiaries directly and to fasten the process. Through the process, money is directly transferred to the beneficiaries' bank account keeping the intermediary agencies and stakeholders only to manage the process of payment.
National TB Elimination Programme (NTEP) transfers all benefits to patients using the two systems:
- Nikshay
- Public Finance Management System (PFMS)
DBT Schemes available in the NTEP
Nikshay Poshan Yojana (NPY)
Objective: To provide nutritional support to TB patients at the time of notification and subsequently during the course of treatment.
Beneficiary: All unique TB patients notified on or after 1st April 2018 (including all existing TB patients under treatment for at least one month from this date).
Benefit Amount: Rs. 500 for a treatment month paid in instalments of up to Rs. 1000 as an advance.
Transport Support for TB patients in Notified Tribal Areas
Objective: To provide financial support as transport allowance for TB patients belonging to notified tribal areas (in addition to the nutritional support provided under NPY).
Beneficiary: All notified TB patients from notified tribal areas.
Benefit Amount: Rs. 750 as a one-time payment at the time of notification.
Incentives for Private Sector Providers and Informants
Objective: To provide financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by a private provider.
Beneficiary: Private providers (private practitioner, hospital, laboratory and chemist) who notify TB patients to NTEP on Nikshay.
Incentive Amount: Rs. 500 as a one-time payment on notification and Rs. 500 to a private practitioner or hospital for updating the patient’s treatment outcome.
Treatment Supporters’ Honorarium
Objective: To provide an honorarium to the treatment supporters for supporting TB patients.
Beneficiary: Community Treatment Supporters who support patients during treatment, leading to a successful outcome (cured or treatment completed).
Incentive Amount: Rs. 1,000 as a one-time payment on the update of outcome for drug-sensitive TB patients and Rs. 2,000 on completion of Intensive Phase (IP) and Rs. 3,000 on completion of Continuation Phase (CP) of treatment for drug-resistant TB patients.
Criteria/ Pre-requisites for Availing the Benefits in NTEP
- All benefits are processed for the respective beneficiary base on the rules and eligibility criteria defined above except for the treatment supporter, which needs to be manually uploaded by the TB Unit (TU) level staff.
- Beneficiary ID in Nikshay will be assigned to all patients which are unique. The benefits processed will be tracked under this ID. All beneficiaries need to register their bank details in Nikshay to enable DBT.
Treatment Supporter
A trained treatment supporter, who can be a health worker or community volunteer, will assist the patient to adhere to the drugs, provide counselling support, nutritional support, screen for adverse reactions, psycho-social support, comorbidity management and follow-up laboratory investigations.
The Treatment Support Honorarium is available as per the following eligibility:
- The treatment Supporter must be registered in Nikshay and designated as the primary Treatment Supporter.
- The linked patient must complete treatment or has to be cured.
- The treatment Supporter should not be a salaried government employee.
Resources
Direct Benefit Transfer Manual for National Tuberculosis Elimination Programme, CTD, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct Explanation
Only patients and treatment supporters seeking treatment in the public sector are eligible for DBT benefits.
True
False
2
Private providers are eligible for financial incentives for notification and subsequent follow-up until completion of treatment of TB patients who are diagnosed/ treated by them.
Free drugs and free treatment
ContentIn the National Sample Survey Office (NSSO) 68th round 2011-2012, India was reported to have the highest out-of-pocket expense on healthcare, of which over 67% was spent on drugs. Recognising the importance of essential drugs being available and accessible to the general public, the Ministry of Health & Family Welfare, Govt. of India, implemented the Free Drugs Service Initiative (FDSI) under the National Health Mission (NHM) in 2015.
Objectives
- To ensure that a set of essential drugs is made available free of cost to all those who access public health care facilities.
- To reduce the Out-of-Pocket Expenses (OOPE) of patients to support their treatment and adherence to medication.
Under this initiative, provision for obtaining free of cost essential medicines is made available through public health facilities under the National Health Mission at Primary Health Centres (PHCs), Community Health Centres (CHCs), Sub Divisional Hospitals (SDH) and District Hospitals (DHs).
Under this scheme, National TB Elimination Programme (NTEP) recommended Fixed-Dose Combination (FDC) anti-TB medicines are also available for both paediatric and adult TB patients. While most of these medicines are procured centrally, few loose drugs, especially for prophylaxis, are allowed to be procured at the state or district level at times when central supply is short.
NHM has dedicated funding for free drugs, and various levels, including Peripheral Health Institutions (PHI), are allotted preset budgets under this scheme. PHIs are supposed to procure essential drugs which are not supplied by the government-owned "General Medical Stores" from this budget. Although most of the drugs are readily provided to the PHIs, some subsidiary drugs and supplements, which are required in TB care, can be made available under this scheme. For example drugs required to treat minor adverse drug reactions, vitamins, protein supplements, expectorants, antitussives, etc.
Resources
-
Operational Guidelines - Free Drugs Service Initiative, MoHFW, GoI.
-
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, CTD, 2017.
-
Essential Medicine List for SHC & PHC Level, Ayushman Bharat - Health and Wellness Centre, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct explanation
To reduce the Out-of-Pocket Expenses (OOPE) of patients.
True
False
1
Free drug service initiative under NHM aims to reduce the Out-of-Pocket Expenses (OOPE) of patients.
PMJAY
Content
Figure: Components of Ayushman Bharat Yojana
Pradhan Mantri Jan Arogya Yojana (PM-JAY) is one of the two key components of the Ayushman Bharat Yojana launched by the Government of India as part of the National Health Policy 2017. It is one significant step toward achieving Universal Health Coverage (UHC) and Sustainable Development Goal - 3 (SDG3): Good health and well-being.
Aim
To provide health protection cover to poor and vulnerable families against financial risk arising from catastrophic health episodes.
Provisions
- Financial protection (Swasthya Suraksha) to 10.74 crore poor, deprived rural families and identified occupational categories of urban workers’ families as per the latest Socio-Economic Caste Census (SECC) data (approx. 50 crore beneficiaries). It will offer a benefit cover of Rs. 5,00,000 per family per year (on a family floater basis).
- Cover medical and hospitalisation expenses for almost all secondary care and most of the tertiary care procedures. PM-JAY has defined 1,350 medical packages covering surgery, medical and daycare treatments, including medicines, diagnostics and transport.
- To ensure that nobody is left out (especially girl child, women, children and the elderly), there will be no cap on family size and age.
- Cashless & paperless at public hospitals and empanelled private hospitals.
- Beneficiaries are not required to pay any charges for hospitalisation expenses.
- Benefit also includes pre and post-hospitalisation expenses.
- The scheme is entitlement based; the beneficiary is decided based on the family being figured in the SECC database.
Benefits for the Health Care System of the Country
- Helps to achieve UHC and SDG.
- Ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially the not-for-profit providers.
- Significantly reduces out-of-pocket expenditure for hospitalisation. Mitigates financial risk arising out of catastrophic health episodes and consequent impoverishment for poor and vulnerable families.
- Acts as a steward, align the growth of the private sector with public health goals.
- Promotes the use of evidence-based health care and cost control for improved health outcomes.
- Strengthens public health care systems through the infusion of insurance revenues.
- Enables the creation of new health infrastructure in rural, remote and under-served areas.
- Increases health expenditure by the government as a percentage of Gross Domestic Product (GDP).
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
PM-JAY benefits can be redeemed only from government hospitals.
True
False
2
PM-JAY provides cashless & paperless benefits at public hospitals and empanelled private hospitals. It ensures improved access and affordability of quality secondary and tertiary care services through a combination of public hospitals and well-measured strategic purchasing of services in health care deficit areas from private care providers, especially not-for-profit providers.
Yes
Yes
-
STLS: TB & Comorbidities and special situations
FullscreenPregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Silicosis in TB Patients
ContentSilicosis is a progressive and disabling interstitial lung disease caused by inhalation and deposition in the lungs of particles of free silica.
Mutual Risk of TB and Silicosis
- TB is a clinical complication of silicosis, called silico-tuberculosis. Silica-exposed workers with or without silicosis are at increased risk for TB. There is also an increased risk of extrapulmonary TB in individuals exposed to silica.
- The risk of a patient with silicosis developing TB is 2.8 – 3.9 times higher than a healthy individual.
- The risk of TB relapse in patients with silicosis is approximately 1.5 times higher than in patients without silicosis.
The presence of silica particles in the lung and silicosis may:
- Facilitate initiation of TB infection and progression to active TB
- Exacerbate the course and outcome of TB, including prognosis and survival
Diagnosis
The diagnosis of silicosis is made based on a history of exposure to silica accompanied by a clinical and radiological profile consistent with the disease.
Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), patients with silicosis are first screened according to the four-symptom complex to rule out/in active TB and tested for TB accordingly.
If active TB is ruled out >> Refer for Tuberculin Skin Test (TST)/ Interferon Gamma Release Assay (IGRA) >> Positive test >> Evaluate with Chest X-ray (CXR) >> Commence TB Preventive Therapy (TPT) irrespective of CXR results.
CXR often indicates TB in silicosis patients earlier than the clinical symptoms, and regular radiographic screening is required for early TB detection. Radiographic comparison of serial films is done with particular attention to:
- Rapid appearance of new opacities, symmetric nodules or consolidation and the finding of pleural effusion or excavations.
- Cavitation is the strongest indicator of probable silico-tuberculosis.
Other diagnostic tools that can help in diagnosis are:
- Chest Computed Tomography (CT) scan
- Bronchoscopy with bronchoalveolar lavage in conjunction with transbronchial biopsy
- Spirometry
Treatment and Follow-up
To keep the disease from getting worse, all silicosis patients need to eliminate any more exposure to silica. Supportive measures include the use of cough medicines, bronchodilators, oxygen therapy and pulmonary rehabilitation.
TB treatment in patients with silicosis is challenging, perhaps due to impairment of macrophage function by free silica and/or poor drug penetration into fibrotic nodules. Usual anti-TB drugs with directly observed therapy are recommended but for an extended duration of at least 8 months, to reduce the chances of relapse.
Follow-up of patients with silicosis and TB follow the same schedule as is in prevailing guidelines.
Prevention
TB prevention in silicosis patients is essential and includes:
- Active surveillance of vulnerable groups including workers
- Adoption of measures to reduce exposure to silica dust
- Patients with silicosis are eligible for TPT after ruling out active TB
NTEP is in the process of engaging with the Ministry of Labour and Mining to identify high priority districts with stone crushing units/ mining industry. Specific guidelines will be developed to support persons with an occupational risk for TB and provide access, diagnosis and treatment services from the programme.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Silico-tuberculosis, Silicosis and Other Respiratory Morbidities Among Sandstone Mine-workers in Rajasthan - A Cross-sectional Study, Saranya Rajavel et al., 2020.
- Mini-review: Silico-tuberculosis; Massimiliano Lanzafame et al, 2021.
- Immunity to the Dual Threat of Silica Exposure and Mycobacterium tuberculosis, Petr Konečný et al., 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about silicosis and TB is/are incorrect?
TB is a clinical complication of silicosis, called silico-tuberculosis.
Silica-exposed workers with or without silicosis are at increased risk for TB and EPTB.
TB in patients with silicosis is easily diagnosed clinically as the patient coughs up silica particles.
TB treatment in patients with silicosis is often of extended duration to prevent relapse.
3
Clinical diagnosis of active TB superimposed on silicosis is often difficult, particularly in the initial phases, when clinical manifestations may not be indicative and radiological alterations can be indistinguishable from those due to the pre-existing silicosis.
Yes Yes Cancer in TB patients
ContentRelationship between Cancer and Tuberculosis (TB)
TB and malignancy may be related in the following four ways:
- TB as a marker for occult cancer: Occult cancer may lead to locally-reduced infection barriers and/or generalised immunosuppression, rendering a cancer patient susceptible to TB infection/ reactivation.
- TB as a risk factor for cancer: TB may increase the risk of cancer locally and systemically through chronic inflammation, fibrosis and production of carcinogenic molecules.
- Shared risk factors for TB and some cancers: Shared risk factors such as smoking, alcoholism, Chronic Obstructive Pulmonary Disease (COPD) and immunosuppression, including HIV, may lead to both TB and cancer, affecting both prevalent and subsequent cancer risk.
- Treatment of cancer-fueling TB: Many cancers are treated with immunosuppressants or steroids. These drugs might induce immunosuppression in the patients undergoing treatment for cancer and hence, a flare-up of TB.
Mutual Risk of Cancer and TB
- TB patients are 2-11 times more likely than non-TB patients to develop lung cancer, according to studies.
- After cancer diagnosis, the incidence of TB also increases, both in the short term and long-term.
- All types of cancer increase the risk of the development of active TB, but with varying degrees. Haematologic cancer patients had the highest rates of active TB, followed by head and neck cancers, lung cancer and breast cancer patients.
There is intrinsic immunosuppression due to the cancer itself, immunosuppressive effects of chemotherapy, or other host factors (e.g., smoking, malnutrition) that may increase the susceptibility to both cancer and TB. Thus, there is increased incidence of TB in cancer patients, and vice-versa.
Diagnosis of TB in Cancer Patients: Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), cancer patients are first screened according to the four-symptom complex to rule out/in active TB and all presumptive TB cases need to undergo testing for TB.
Co-existence of TB and cancer poses a diagnostic challenge since clinical and radiological presentations between TB and cancers are similar, hence the need for bidirectional screening. E.g., if biopsy specimens reveal infiltration by malignant cells, still send sample for microbiological confirmation of M. tuberculosis. Thus, allowing for accurate diagnosis and initiation of anti-TB treatment instead of attributing clinical deterioration to chemotherapy complications and progression of underlying malignancy.
Diagnosis of lung cancer in TB patients is usually done in consultation with a clinical specialist and can include examination of induced sputum specimens for malignant cells, as well as use of other diagnostic tools such as Computed Tomography (CT) scans, bronchoscopy, Positron Emission Tomography (PET) scans, Magnetic Resonance Imaging (MRI), histopathology and the use of biological markers.
Treatment
TB treatment in cancer patients uses the standard DS-TB/DR-TB regimens and course, except that the treating physician should assess the drug interactions between anti-TB and anti-cancer drugs. For cancer treatment, drugs may have to be modified to accommodate anti-TB treatment and to aid better prognosis of the TB outcome. However, all decisions must be taken by a competent specialist after examining the individual case.
Curative resection, chemotherapy and radiation therapy are the mainstay treatment options for cancer in TB patients. Co-existence of TB in cancer patients necessitates anti-TB treatment with extended duration, if required. Follow-up during and after treatment also follows prevailing guidelines.
Prevention
Under the NTEP, TB prevention in cancer patients is essential and includes:
- Regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-Tumour Necrosis Factor (TNF) medicines.
- Education and referral of patients who do not have TB symptoms for TB infection testing/assessment of their eligibility for TPT.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis and Risk of Cancer: A Danish Nationwide Cohort Study, D. F. Simonsen et al., International Journal of Tuberculosis and Lung Diseases, The Union, 2014.
- Increased Risk of Active Tuberculosis after Cancer Diagnosis, Dennis F. Simonsen et al., Journal of Infection, 2017.
- Pulmonary Tuberculosis as Differential Diagnosis of Lung Cancer; MLB Bhatt et al., South Asian Journal of Cancer, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about cancer and TB is/are incorrect?
Under NTEP, regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-TNF medicines is done.
TB increases the risk of developing cancer, but cancer patients do not usually get TB.
Sputum smear microscopy is important when diagnosing TB in cancer patients.
All of the above
2
There is mutual risk between cancer and TB. TB increases the risk of developing cancer, and cancer patients are more likely to develop TB.
Yes Yes COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
-
STLS: TB Preventive Treatment
FullscreenTB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes Target groups for TPT
ContentThe NTEP has prioritized the target population for TPT based on elevated risk of progression from infection to TB disease or increased likelihood of exposure to TB disease.
The target populations have been divided into two groups:
- Household contacts of bacteriologically confirmed pulmonary TB patients notified in Nikshay from public and private sector.
Target Population
Strategy
- People living with HIV (+ ART)
- Adults and children >12 months
- Infants <12 months with HIV in contact with active TB
- HHC below 5 years of pulmonary* TB patients
TPT to all after ruling out active TB disease - HHC 5 years and above of pulmonary* TB patients#
TPT among TBI positive# after ruling out TB disease #Chest X Ray (CXR) and TBI testing would be offered wherever available, but TPT must not be deferred in their absence
*Bacteriologically confirmed pulmonary TB patients to be prioritized for enumeration of the target population for TPT
- Expanded to other risk groups
Target Population
Strategy
Individuals who are:
- on immunosuppressive therapy
- having silicosis
- on anti-TNF treatment
- on dialysis
- preparing for organ or hematologic transplantation
TPT after ruling out TB disease among TBI positive Cascade of Care for TPT
ContentIn the cascade of care approach, all target populations (People Living with HIV (PLHIV), Household Contacts (HHCs) and other such groups) who are at risk of developing TB disease are systematically reached out, screened for TB disease and after ruling out active TB disease, provided TB Preventive Treatment (TPT) as a part of the continuum of care.
The cascade of care approach among TPT target populations is shown in Figure 1.
Image
Figure 1: Cascade of TB Preventive Treatment; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment, p3.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is the correct TPT cascade of care? Offer upfront CBNAAT to all at-risk populations, then offer TPT based on the results. Identify at-risk populations, then offer TPT to all the people that have been identified. Identify target populations at risk of developing TB, screen them, rule-out active TB disease, and provide TPT to eligible populations. None of the above 3 The TPT cascade of care is: Identify target populations at risk of developing TB disease, screen them for TB disease, rule-out active TB disease, and provide TPT to eligible populations. Approaches for TPT implementation
ContentThere are two programmatic approaches for Tuberculosis Preventive Therapy (TPT) implementation:
1. Test-and-treat approach – This approach aims to detect TB infection among key groups for implementing TPT.
- After ruling out active TB, the beneficiary is tested for TB infection.
- TPT is offered only to those with a positive test (Interferon Gamma Release Assay (IGRA)/ Tuberculin Skin Test (TST)/ Cutaneous TB (C-TB))
2. Treat-only approach – For certain groups, like People Living with HIV (PLHIV) and House Hold Contacts (HHC) < 5 years old, detecting TB infection is not required. Hence, this approach is given.
- After ruling out active TB, TPT is offered without testing for TB infection.
Test and treat approach*
- HHC of sputum positive Pulmonary TB >/= 5 years old
- Individuals on:
- Immunosuppressive therapy
- Having silicosis
- On anti-TumourTNF treatment
- On dialysis
- Preparing for solid organ or haematopoietic stem cell transplantation
Treat-only approach
- HHC of sputum positive Pulmonary TB (PTB) < 5 years old
- PLHIV#
*All efforts should be made to make IGRA available. However, TPT should not be withheld in case of non-availability of IGRA.
#PLHIV < 1 year old are offered TPT only if they are a household contact of an active TB case.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following category of TPT beneficiaries is offered TPT without IGRA testing?
Household contacts of sputum positive PTB >/= 5 years old
PLHIV
Patient on dialysis
Silicosis patient
2
PLHIV and HHC of sputum positive PTB < 5 years old are offered TPT without testing for IGRA. This is called Treat-only approach.
Yes
Yes
Counselling for IGRA/TST
ContentInterferon Gamma Release Assay (IGRA) and Tuberculin Skin Tests (TST) are performed on individuals who are ruled out for active TB disease.
However, positive and negative tests in IGRA and TST do not necessarily mean the patient does or does not have Tuberculosis Infection (TBI) as the possibility of false positives and false negatives cannot be ruled out in these tests.
Importance of Counselling in IGRA/ TST
- All patients who undergo IGRA/ TST are already aware that they do not have an active TB disease and hence counselling is important to help them make informed decisions about undergoing IGRA/ TST for detecting TBI.
- Additionally, at the time of receiving positive IGRA/ TST results, they may be symptom-free or otherwise healthy. In such cases, resistance/denial to receive a prophylactic treatment like TB Preventive Therapy (TPT) is higher as its treatment course duration also is relatively longer.
- Counselling in IGRA/ TST is of utmost importance when the respective person belongs to the high-risk population and needs to be necessarily initiated on TPT and thus needs to be counselled for the same.
Components of Counselling in IGRA/ TST
- Information on TBI
- Need for undergoing IGRA/ TST
- Importance of initiating TPT post-IGRA/ TST tests
- If initiated on treatment, then schedule of medication
- Medication adherence support
- Follow-up
- Importance of completing the TPT course, adverse events
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India, CTD, MoHFW, India, 2021.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, CTD, MoHFW, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Counselling for IGRA/ TST should necessarily include which of the following?
Counselling on DR-TB
Counselling on TB Infection (TBI)
Counselling on DBT
None of the above
2
Counselling for IGRA/ TST should necessarily include ‘Counselling on TB infection (TBI)’.
Yes
Yes
Counselling for TPT
ContentCounselling is of paramount importance for TB Preventive Treatment (TPT) initiation and completion as most of the target population screened and found eligible would know that they do not have TB disease, would be symptom-free or otherwise healthy and would not feel the need to take any treatment, especially Household Contacts (HHC).
Stakeholders Involved in Counselling for TPT (Figure below)

Figure: Stakeholders involved in counselling for TPT
Abbr: HWCs: Health and Wellness Centres; PHC: Primary Health Centre; ICTC: Integrated Counselling and Testing Centres; ART: Anti-retroviral Therapy; PLHIV: People Living with HIV
Components of Counselling for TPT
While counselling the person and family members, the treating doctors/ staff must follow the steps outlined in the table below for an effective counselling session.
Component
Actions to be taken
Confidentiality
Ensure confidentiality when seeking a person’s commitment to complete the course before initiating TPT.
Information
Provide information on:
- TB infection
- Need for TPT and protective benefits to the individual, household and wider community
- TPT is available free of charge under National Tuberculosis Elimination Programme (NTEP)
- TPT regimen prescribed, including duration, schedule of medication collection, and directions on how to take the medications
- Potential side-effects and adverse events involved and what to do in the event of various side-effects. People treated with rifamycins should be alerted in advance about the pink discolouration of secretions due to this medicine
- Importance of completing the full course of TPT
- Reasons and schedule of regular clinical and laboratory follow-up for treatment and monitoring
- Signs and symptoms of TB and advise on steps if they develop them
Medication adherence support
Agree on the best way to support treatment adherence, including the most suitable location for drug intake and the need for a treatment supporter, if required.
Family support
Involve family members and caregivers in health education when possible.
Openness
Invite clarification questions and provide clear and simple answers.
Information, Education and Communication materials
- Provide information materials in the local language and at the appropriate literacy level of the person concerned.
- Reinforce supportive educational messages at each contact during treatment.
Call support (in case of emergencies)
Provide a telephone number of the HCW staff/ TB Health Visitors and Senior Treatment Supervisors concerned to call for other queries or a need to contact health services for advice.
The National TB Elimination Programme (NTEP) national call centre (NIKSHAY SAMPARK – Toll-free number 1800116666) may be provided to index TB patients, those initiated on TPT and family members to serve as a resource for information, counselling and troubleshooting as required to enable TPT initiation, follow-up monitoring and completion.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following people are involved when counselling for TPT?
Index TB patients
Caregivers
Family members
All of the above
4
When counselling persons eligible for TPT, it is best to involve the index TB patients, their families and caregivers.
Yes Yes Monitoring adherence to TPT
ContentTo achieve high treatment completion rates and the desired epidemiological impact of the TB Preventive Treatment (TPT), monitoring TPT treatment adherence, including management of missed doses and Adverse Drug Reactions (ADRs), is of paramount importance under the National TB Elimination Programme (NTEP).
Significance of Monitoring Adherence to TPT
Adherence to the TPT course and treatment completion are important determinants of clinical benefit, both at the individual and population levels as:
- Irregular or inadequate treatment reduces the protective efficacy of the TPT regimen.
- Poor adherence or early cessation of TPT can potentially increase the risk of the individual developing TB, including drug-resistant TB.
- Efficacy of TPT is greatest if at least 80% of the doses are taken within the duration of the regimen. The total number of doses taken is also a key determinant of the extent of TB prevention.

Figure: Strategies to Promote Adherence
Prevent TB India App and Integration with Nikshay as a Monitoring Tool
- Currently, under the NTEP, the person’s lifecycle approach and TB treatment episode level are recorded in Nikshay.
- TPT information management is integrated with this existing Nikshay approach. This includes information on screening, testing, eligibility assessment, TPT initiation, adherence monitoring and follow-up till treatment completion.
- The NTEP has adapted the World Health Organisation (WHO) Prevent TB India app and hosted it on Nikshay as an interim solution till the Nikshay TPT module is developed and fully functional.
- Health workers or treatment supporters will make entries directly into the app.
- The TPT monitoring dashboard can be accessed by various levels of supervisors using their respective Nikshay login ids using a link provided in the Nikshay Reports section on TPT Reports.
- A web-based comprehensive dashboard for Prevent TB initiative is also available at https://ltbi.nikshay.in/ltbi-generic-new/#/
Table: Roles of Stakeholders in Monitoring Adherence to TPT Role
Stakeholder
Treatment support and adherence monitoring including entry of daily doses taken in the Prevent TB India app/ Nikshay TPT module.
Community volunteers (TB survivors/ champions, Accredited Social Health Activists (ASHAs) and Anganwadi Workers)
- Regularly undertake home visits or tele/ video calls to monitor TPT adherence.
- Identify treatment interruptions at the earliest (Dashboards of Prevent TB India app/ Nikshay TPT module may be checked every week along with pill counting).
- HWCs/ sub-centre/ urban health posts (Community Health Officers (CHOs), Auxillary Nurse Midwives (ANMs), multipurpose workers and other field staff)
- Primary Health Centres (PHCs)/ Urban PHCs/ Private clinic (Medical Officers (MO), staff nurse)
- Adherence support and clinical monitoring through the concerned PHC/ sub-centre.
- Supportive supervision and handholding support to field level facilities and frontline workers, ASHAs and community volunteers on digital recording, using Prevent TB India app and monitoring TPT and follow-up examinations.
TB Unit (MO, Laboratory Technicians (LTs), staff nurse, pharmacist, counsellor (if available), Senior Treatment Supervisors (STS), Senior TB Laboroary Supervisors (STLS), TB Health Visitors (TBHV))
Ensuring adherence support for People Living with HIV (PLHIV) on TPT through mechanisms such as outreach workers, PLHIV networks, peer support groups, etc.
Anti Retroviral Therapy (ART) centre/ Link ART centre (MO, pharmacist, (institutional) staff nurse, counsellor, care coordinator)
Monitor and support adherence to TPT.
Tertiary care/ Medical colleges/ Corporate hospitals/ District hospitals/ Dialysis/ Cancer facilities (doctors, staff nurses)
Review data updating in Prevent TB India app/ Nikshay TPT module wherever available, check the quality of data regularly and provide feedback to TPT treatment supporters and for retrieval of TPT interrupters.
Supervisory staff at all health facilities including the State/ District TB cell (State TB Officers (STO), District TB Officers (DTO), State/ District Programme Coordinators)
Resources:
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment.
- Prevent TB Dashboard.
- Prevent TB India Mobile App.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which tools are used to monitor TPT adherence under the NTEP?
Video calls
Counting empty blisters
Directly asking the patient
Options 1 and 2
4
TPT adherence monitoring tools include direct observation of drug intake, 99DOTS/ MERM, counting empty blisters, tele/ video calls and refill monitoring.
Which of the following apps are currently used by NTEP to monitor TPT adherence?
TB Aarogya Sathi
Prevent TB India App
TPT app for NTEP
None of the above
2
NTEP has adapted the WHO Prevent TB India app and hosted it on Nikshay to monitor the entire TPT care cascade, including TPT adherence.
Fullscreen