Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
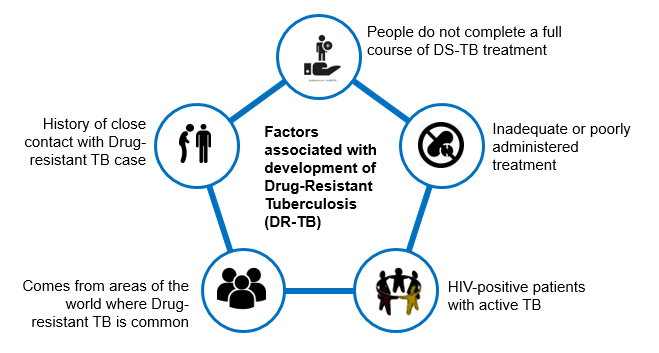
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Screening for DR-TB
ContentAll patients diagnosed with TB should have universal access to rapid DST for at least Rifampicin and further DST for at least Fluoroquinolones among all TB patients with rifampicin resistance, i.e. UDST.
UDST tests are offered preferably before treatment initiation to a maximum within 15 days from diagnosis. Based on the UDST test result, if Rifampicin resistance is detected, the patient is shifted to DR-TB Treatment Regimen. If Rifampicin resistance is not detected, then first-line anti TB treatment is continued, and the patient is screened further on their follow-ups. If tested positive in sputum examination during any patient follow up, then sputum is sent for further drug resistance testing, and the patient is referred to PHI for follow-up.
Figure: Screening of patient for initiating DRTB Treatment from DSTB Treatment
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
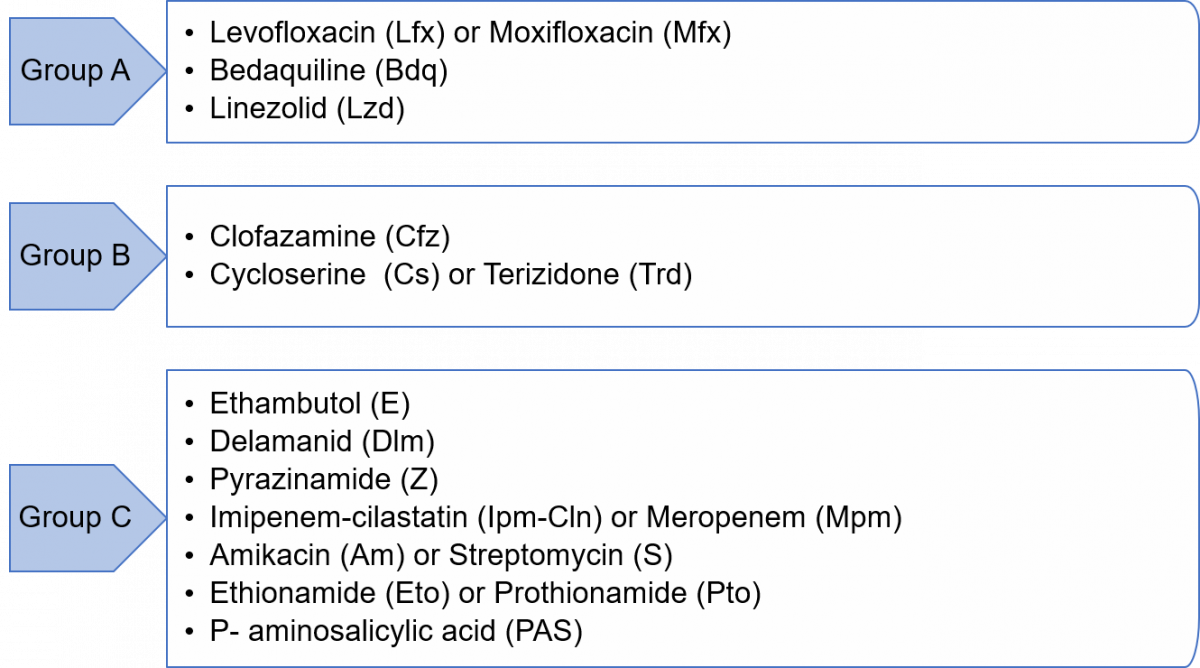
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to Second Line Treatment
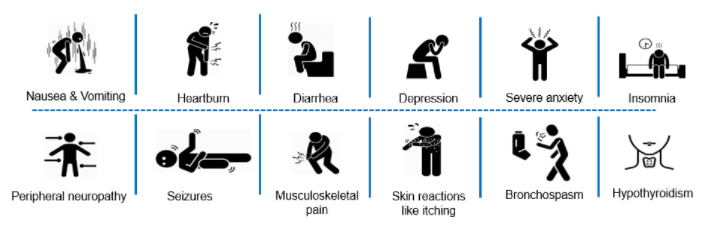
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
Fullscreen