Goals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Strategies for TB Treatment
ContentUnder the National TB Elimination Programme (NTEP), strategies adopted in the treatment of TB are based on the available scientific and operational researches. These strategies are combined to ensure better treatment outcomes for the TB patients. The main strategies include:
Domiciliary Treatment
- This is a strategy that allows for the treatment of TB in a patient’s home.
- Domiciliary chemotherapy proved to be as effective as sanatoria treatment (which was the historical way of treating TB) and achieved higher cure rates.
- The patients having the social benefits of being at home.
Short Course Chemotherapy (SCC)
- Chemotherapy of TB underwent revolutionary changes in the 70s owing to the availability of two well-tolerated and highly effective drugs – rifampicin and pyrazinamide.
- These drugs allowed for SCC and made it possible to simplify treatment and reduce its duration without reducing the therapeutic effect.
- Now with SCC regimens, it is possible to treat and cure TB patients in 6 months.
- When given daily, these regimens are effective, achieve high cure rates, prevent the emergence of drug resistance and minimize relapses.
- The shorter duration also contributes to improvement in treatment adherence.
Directly Observed Treatment (DOT)
DOT is a method whereby a trained healthcare worker or another trained designated person (treatment supporter) watches a patient swallow each dose of anti-TB drugs and document it.
- DOT can reduce the development of drug resistance, treatment failure, or relapse after the end of treatment.
- Many patients who do not receive directly observed treatment stop taking drugs once they feel better.
- Hence, by providing DOT, the NTEP ensures that patients receive the right drugs, in the right doses, at the right intervals and for the right duration.
The modern treatment strategy is based on standardized short-course chemotherapy regimens largely administered on a domiciliary basis, utilising the DOTS strategy and proper case management to ensure completion of treatment and cure.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Treatment of Tuberculosis Disease, CDC, 2006.
- Guide on Tuberculosis Control for Primary Health Care Providers, WHO, 2015.
- Treatment of Tuberculosis: Guidelines for National Programmes, WHO, 2003.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these treatment strategies are adopted by NTEP?
Domiciliary treatment
Use of short-course chemotherapy
Directly observed treatment
All of the above
4
Strategies utilized by NTEP in TB treatment are domiciliary, short-course chemotherapeutic short-course regimens that are directly observed.
Pharmacological Basis of treatment
ContentTuberculosis treatment and its different regimens have scientific backgrounds for their formulations. To understand this, we need to know about the mode of action of each anti-TB drug first.
Mode of Action of Anti-TB Drugs
Anti-TB drugs have the following three actions:
- Early bactericidal activity: Killing of actively growing bacilli (in the phase of rapid multiplication and uninhibited metabolic activity).
- Sterilizing activity of persisting bacilli, i.e., metabolically inhibited organisms in a quasi-dormant state.
- Ability to prevent the emergence of drug resistance.
The ranking of first-line drugs with respect to their type of activity is indicated in Table 1 below.
Table 1: Ranking of first-line anti-TB drugs used in the treatment of drug-sensitive TB, based on the mode of action and activity
First-line Drugs Early Bactericidal Sterilizing Prevention of emergence of drug resistance Isoniazid (H) ++++ ++ ++++ Rifampicin (R) +++ ++++ +++ Pyrazinamide (Z) ++ +++ + Ethambutol (E) + Nil ++ Thus, each drug has unique characteristics and drug combinations will make the regimen more effective.
Need for Long Duration of Treatment of TB
- Anti-TB drugs mostly kill actively multiplying tubercle bacilli.
- When bacilli have low metabolic activity, i.e., when bacterial growth has almost come to a standstill and the organisms are “dormant”, they are not killed by otherwise bactericidal drugs. Such organisms are referred to as persisters*.
- Though they may survive in the presence of drugs, behaving as if they were drug-resistant, they are in fact susceptible to the drugs.
- Thus, if for some reason these organisms regain their ability to multiply freely, they would be killed by the very drugs that had not harmed them before.
- When dormant bacilli again become metabolically active and start multiplying during effective chemotherapy, they are soon killed.
- Once chemotherapy has been completed, the revived bacilli may continue to multiply and thus cause relapse.
- This explains why conventional chemotherapy needs to be of long duration.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the role of the intensive phase of anti-TB treatment? To reduce adverse drug reactions in patients To achieve rapid killing of actively multiplying bacillary population
To prevent the emergence of drug-resistance Options 2 and 3 4 The role of IP is to achieve rapid killing of actively multiplying bacillary population and eliminate naturally occurring drug-resistant mutants and prevent the further emergence of drug resistance. Yes Yes Which of the following drugs is bacteriostatic? Isoniazid Ethambutol Pyrazinamide Rifampicin 2 Ethambutol is an effective bacteriostatic drug, helpful in preventing the emergence of resistance to other companion drugs. Yes Yes Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentIt is extremely important for any type of TB patient to be initiated on the right treatment at the earliest in order to have better treatment outcomes. Therefore as soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen.
Steps in TB Treatment Initiation
Image
Figure: Flowchart-Treatment Initiation
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, India, 2021.
- Training Modules (1-4) for Programme Managers and Medical Officers, CTD, MoHFW, India.
Assessment
Question
Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. True False 1 The ultimate goal of the initial counselling session should be to empower the patient and their caregiver to make informed decisions regarding the treatment initiation. Yes Yes As soon as the patient is diagnosed, s/he should immediately be traced with the help of the Community Health Officer (CHO) of the Health and Wellness Centres (HWC), TB Health Visitors (TBHV) / Senior Treatment Supervisor(STS) and the health facility doctors and initiated on the appropriate treatment regimen
True False 1 Soon after identification pre treatment counselling is given to patient and caregivers followed by pre treatment evaluation and treatment initiation. Yes Yes Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Closing Cases and Assigning Treatment Outcomes
ContentVideo fileVideo:
Closing Cases and Assigning Treatment Outcomes (Web)
Video fileVideo:
Closing Cases and Assigning Treatment Outcomes (Mobile)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
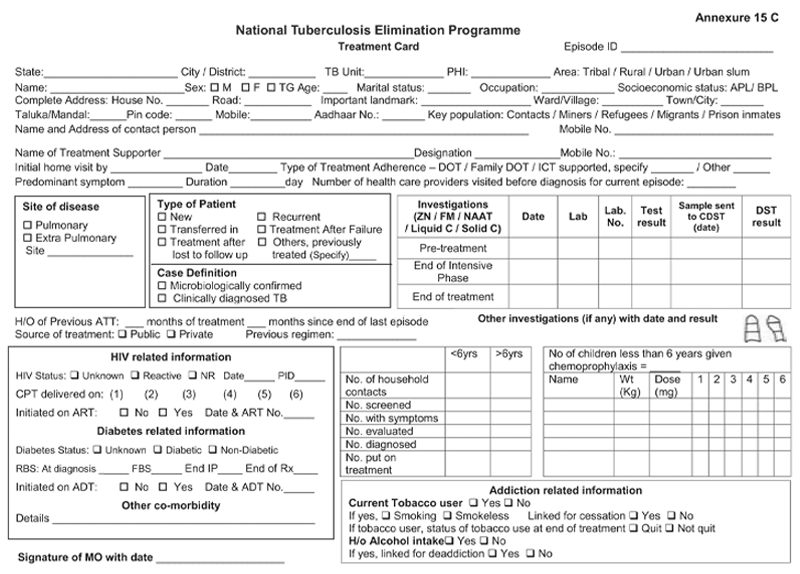
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
NTEP TB ID Card
ContentIn the National TB Elimination Programme (NTEP), the ‘NTEP TB identity card’ is provided for their identification and record of clinical follow-ups.
The identity card is completed for each patient who has a Tuberculosis (TB) Treatment Card, and it is kept with the patient. Information from the TB Treatment Card is used to complete the identity card.
There are 3 parts in the NTEP TB identity card and details in each part is delineated in Table 1.
Table 1: Parts of the NTEP TB identity card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PART
DETAILS CONTAINED IN THE SECTION
The First and Second Part
Patient information
Name and address of the TB unit/ district
Treatment details of the patient including:
- Disease classification
- Type of patient
- Treatment provider
- Case definition
- Weight bands
- Dosage
- Sputum results
- Culture results
- Results of follow-up smear examinations
- Results of follow-up cultures
- Information on the date of treatment initiation
- Treatment outcome
The Back Part
Appointment dates for visits to NTEP facilities
Contact details of NTEP staff in case of side events/queries
The information contained in this card will help to continue treatment in case the patient is transferred or admitted to any other health facility any time during the treatment period. The TB identity card is shown in Figure 1.
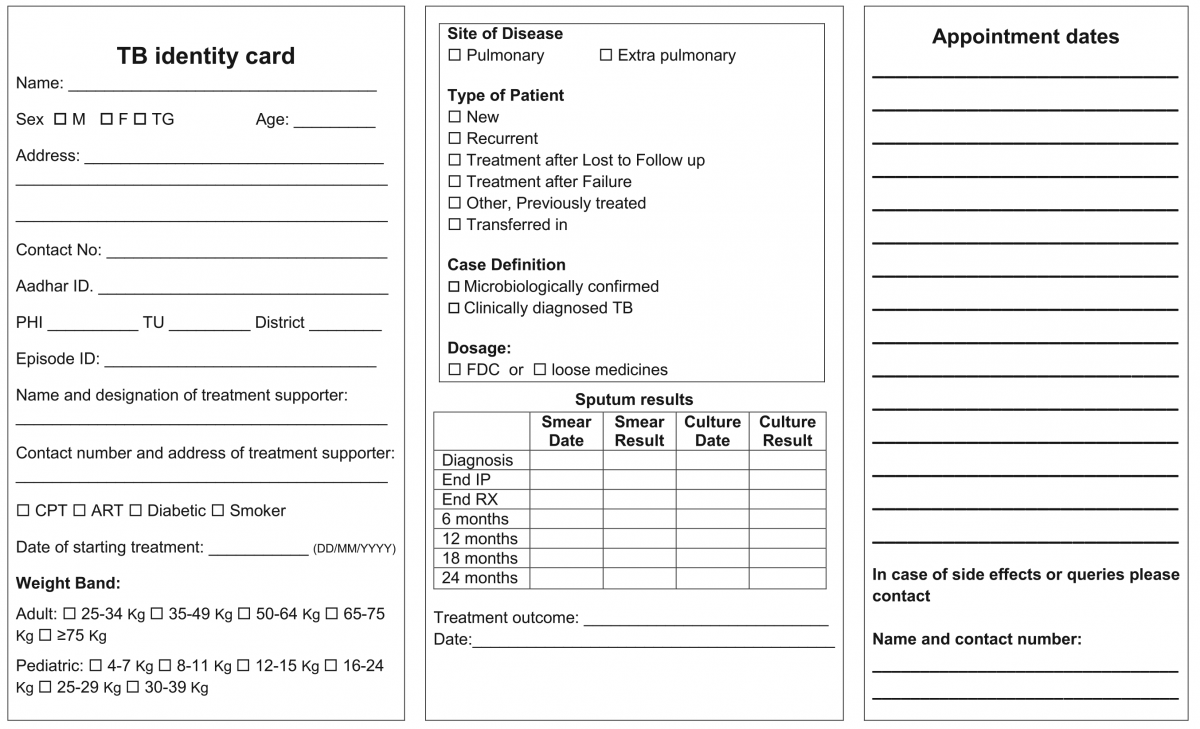
Figure 1: NTEP TB Identity Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020

Figure 2: Sample of a patient’s TB identity card


Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
Pharmacovigilance in NTEP
ContentPharmacovigilance is defined by the World Health Organisation (WHO) as the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problem.
- It is a fundamental public health surveillance activity to ensure patient safety measures in healthcare.
- Good pharmacovigilance will identify the risks within the shortest possible time after medicines have been marketed and help establish or identify risk factors.
Importance of Pharmacovigilance
Pharmacovigilance allows for intelligent, evidence-based prescribing with the potential for preventing many Adverse Drug Reactions (ADRs). Pharmacovigilance will help in:
- Improving patient care by assessing both the harms and benefits received from drugs (anti-tubercular treatment).
- Strengthening patient safety, safeguarding the patient’s interests and ensuring adherence to prescribed drug regimens.
- Preventing antimicrobial resistance.
Pharmacovigilance ultimately helps each patient in receiving optimum therapy at a lower cost to the health system.
Conducting Pharmacovigilance under the National TB Elimination Programme (NTEP)
The Pharmacovigilance Programme of India (PvPI) was set up by the Ministry of Health and Family Welfare, Govt. of India, in July 2010. PvPI is India’s national programme for surveillance of ADR-related information.
NTEP in collaboration with PvPI, and with support from WHO India, developed the comprehensive active Drug Safety Monitoring and Management (aDSM) system for ADR monitoring. Pharmacovigilance is prioritised in Drug-resistant TB (DR-TB) centres for drug-resistant cases.
Adverse events reporting for pharmacovigilance is done as follows:
- DR-TB centres are linked with ADR Monitoring Centres (AMC) established in medical colleges to initiate reporting of ADR in a systematic manner.
- Serious adverse events are reported to AMCs and Central TB Division (CTD) within 24 hours. This is done via a standardized suspected ADR reporting form (Annexure-11) which is filled by the treating doctor.
- The data is entered in Nikshay on a regular basis by statistical assistants at the nodal DR-TB centre and senior DR-TB TB-HIV supervisors at the district DR-TB centre.
- From Nikshay, the information is directly communicated to PvPI through a connecting bridge called Vigiflow.
- The ADR data submitted to Vigifloware is analysed by PvPI and shared with CTD on a regular basis.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Ready Reckoner for Medical Officer - Adverse Drug Reactions Associated with Anti-TB Drugs Identification and Management, 2019.
- Practical Handbook on the Pharmacovigilance of Medicines used in the Treatment of Tuberculosis, WHO, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is true concerning pharmacovigilance in NTEP?
PvPI is India’s national programme for surveillance of ADR-related information.
ADR-related information flows between Nikshay and PvPI via Vigiflow.
Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
All of the above
4
PvPI is India’s national programme for surveillance of ADR-related information, which flows between Nikshay and PvPI via Vigiflow. Pharmacovigilance assesses both the harms and benefits received from anti-TB drugs.
Yes Yes Follow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
Management of EPTB
ContentThe management principles of Extrapulmonary Tuberculosis (EPTB) are shown in the figure below.

Figure: Ten principles about what every EPTB patient in India needs as a basic standard of care
Abbr: CBNAAT:Cartridge-based Nucleic Acid AMplification Test; PTB: Pulmonary TB; NTEP: National TB Elimination Programme
Diagnosis of EP-TB
- All efforts need to be made to get a microbiological confirmation whenever a sample is available.
- Clinical diagnosis can be made by treating physician based on the clinical features, lab investigations, imaging studies and by ruling out other causes
Treatment Regimen and Duration for EPTB
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE). However, the duration of the continuation phase in EPTB may be extended in special situations such as TB Meningitis, bone and spine TB etc.
Role of Surgery in EPTB Cases
- Surgery is sometimes required for the diagnosis of EPTB. It is reserved for management of late complications of the disease.
Monitoring Treatment Response
- Response to treatment in EPTB may be best assessed clinically. Clinical follow-up is the most important criterion for the follow-up of EPTB patients. The clinician can assess the patient’s condition by checking weight gain and a decrease/ increase in presenting clinical symptoms.
- Investigations such as Acid-fast Bacilli (AFB) microscopy, chest X-ray, liver function tests, serum creatinine, and USG-abdomen can be used to monitor the treatment status.
The treatment support and other monitoring activities remain the same as for pulmonary TB.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Index TB Guidelines on Extra-pulmonary Tuberculosis for India, Central TB Division, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the standard treatment duration for most EPTB cases?
2 weeks
1 month
6 months
3 years
3
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE).
Yes Yes In which cases can the treatment duration exceed 6 months in EPTB?
TB meningitis
TB of the bone and joint
Depending on the clinician’s decision
All of the above
4
EPTB treatment duration can be extended beyond 6 months in TB meningitis, TB of bone and joint (including TB otitis media), and if recommended by the clinician.
Yes
Yes
Management of Patients with Treatment Interruptions
ContentTreatment interruption is defined as a patient-initiated episode in which the patient discontinues TB treatment. All efforts must be made to ensure that TB patients do not interrupt treatment or are not lost to follow-up. Action should be taken to promptly retrieve patients who fail to come for their daily dose by the treatment supporter
The management of treatment interruptions is made based on the following criteria:
i. Type of case: Whether new, relapse or failure
ii. Duration of treatment taken: Less than one month/ more than one month. This helps in assessing the risk of the presence of drug resistance.
iii. Duration of Interruption: Less than one month/ more than a month.
If treatment interruption is more than one month, the outcome is declared as ‘lost to follow up’.
If a patient returns to the health facility after interrupting treatment for more than one month, the patient sample needs to be subjected to Drug Susceptibility Testing (DST) to determine resistance/ sensitivity status to anti-TB drugs.
In case the interruption is for less than one month, the same treatment regimen is completed to complete all doses.
Modes of Retrieval
TB treatment is supervised by a trained treatment supporter (a health worker, family member or community volunteer). The residential address is verified for all TB patients by home visits. However, in case of treatment interruption, patient retrieval action is required.
Retrieval can be done by the following modes:
1. Retrieval of patients interrupting treatment within 24 hours of discontinuation is done by the Treatment Supporter (TS) or Accredited Social Health Activist (ASHA)/ Auxilliary Nurse Midwife (ANM)/ Multipurpose Worker (MPW). The reason for interruptions should be reviewed carefully and efforts made to counsel and bring the patient back for treatment.
2. If the TS is not successful in retrieving such patients, it should be reported to the next higher level of supervisors, like Senior Treatment Supervisor (STS), and they should take all efforts to counsel and retrieve the patient.
3. If the patient interrupts treatment on more than one occasion, the Medical Officer of the Peripheral Health Institute (MO-PHI) should visit the patient’s home. The MO-PHI should give intensive counselling to the patient and may provide additional support to continue the treatment without interruption.
4. Innovative use of information and communication technologies for treatment adherence monitoring through 99 DOTS, Medication Event Reminder Monitor (MERM), etc. are also beneficial in finding missed doses and initiating retrieval action by the health staff.
Resources
1. Training Modules (1-4) for Programme Managers and Medical Officers.
2. Guidelines for PMDT in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. True False 1 If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. Yes Yes Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Management of TB in special situations
ContentThe treatment for TB is demanding in terms of duration of treatment, adverse drug reactions, the requirement of prolonged adherence by patients and catastrophic expenditures. The presence of a special condition added on by a TB diagnosis makes it even more challenging.
To improve the outcomes for such challenging situations, the programme recommends certain modifications in the regimen, which are listed in the table below.
Table: Management of TB in Special Situations
Pregnancy and lactation Pregnant women with TB should be jointly managed by an obstetrician/ gynaecologist and pulmonologist/ physician. The shorter oral Bedaquiline-containing Multidrug-resistant (MDR)/Rifampicin-resistant (RR)-TB regimen should not be administered in pregnant women before 32 weeks due to Ethionamide (Eto) led to potential teratogenicity in first trimester and risk of hypothyroidism in the infant in second trimester. Beyond 32 weeks, the choice of regimen needs to be a consultative decision between the obstetrician and physician at the Nodal/District Drug-resistant TB Centre (N/DDR-TBC). In pregnant women diagnosed with DR-TB, if the duration of pregnancy is <20 weeks*, the patient should be advised to opt for Medical Termination of Pregnancy (MTP) in view of the potential severe risk to both mother and foetus. Bedaquiline (Bdq) and Delamanid (Dlm) both should not be recommended during the lactating period unless the mother is willing to replace breastfeeding with formula feed. Breastfeeding must be continued and after ruling out active TB, the baby should be given 6 months of isoniazid preventive therapy, The mother should be advised about cough hygiene measures such as covering the nose and mouth while coughing, sneezing or any act which can produce sputum droplets. Mothers receiving INH and their breastfed infants should be supplemented with vitamin B6 (pyridoxine), recommended dose of Pyridoxine in infants is 5 mg/day and for mother is 10mg/day. Renal impairment In the presence of mild to moderate renal impairment dosage of Ethambutol (E) and Levofloxacin (Lfx) should be adjusted. In the presence of severe renal impairment, Lfx can be replaced with a normal dose of Moxifloxacin (Mfx) (200/400 mg based on the patients’ weight). In case of patients undergoing dialysis, medicine should be given either 4-6 hours before dialysis or immediately after dialysis Pre-existing liver disease MDR/ RR-TB patients having deranged Liver Function Test (LFT) during pre-treatment evaluation should be strictly monitored as clinically indicated while on treatment. In patients with pre-existing liver disease with persistently abnormal liver function tests, a shorter oral MDR/ RR-TB regimen should be avoided due to presence of High-dose Isoniazid (H(h)), Eto and Pyrazinamide (Z). If the serum alanine aminotransferase level is more than 3 times normal before the initiation of treatment, the following regimens should be considered: –
- Containing two hepatotoxic drugs:
- 9 months of isoniazid and rifampicin, plus ethambutol (until or unless isoniazid susceptibility is documented) - 9HRE
- 2 months of isoniazid, rifampicin, streptomycin and ethambutol, followed by 7 months of isoniazid and rifampicin-2SHR/ 7HR
- 6–9 months of rifampicin, pyrazinamide and ethambutol-(6-9 RZE)
- Containing one hepatotoxic drug: 2 months of isoniazid, ethambutol and streptomycin, followed by 10 months of isoniazid and ethambutol (2SHE/10 HE)
- Containing no hepatotoxic drugs: 18–24 months of streptomycin, ethambutol and fluoroquinolone. (18-24 SLE)
Seizure disorders Patients should be evaluated to check if seizures are under control and verify if the patient is taking anti-seizure medication. Since Eto, Fluoroquinolones (FQ), and high dose Isoniazid are associated with seizures they should be used carefully/ avoided amongst MDR/RR-TB patients with a history of seizures. Though the seizure is not common with Bdq, it should also be considered while assessing the causality assessment. The prophylactic use of oral pyridoxine (vitamin B6) up to 5-25 mg/day can be used in patients with seizure disorders to protect against the neurological adverse effects of isoniazid or cycloserine. Serum levels of anti-epileptic drugs should be monitored closely to identify any drug interactions. Management of Adverse Drug Reactions (ADRs) in Special Situations
- The actual management of ADR begins during the treatment initiation counselling, where the patient should be instructed in detail about potential adverse effects due to the prescribed drug regimen and when they occur, to notify a healthcare provider.
- Treatment Supporter (TS) should be trained to closely monitor the patient for any signs of ADR (especially, since drug-drug interaction could happen) daily so that they can be recognized and managed quickly.
- The TS should also be trained to identify ADR as major and minor.
- A symptom-based approach should be followed to manage minor ADR where the patient is usually able to tolerate anti-TB drugs and continue medication with symptomatic treatment. Appropriate referrals should be made for all major ADRs that may require hospitalization of the patient.
- If the adverse effect is mild and not serious the treatment regimen must be continued with the help of ancillary drugs, if needed.
- For most second-line drugs related ADR, reducing the dosage/ terminating the offending drug can be considered and should be decided by the Nodal/District Drug-resistant TB Centre (N/DD- TBC) committee.
- Psychosocial support, patient education and motivation through TS and other patient support groups are also effective ways to manage the ADRs.
Resources
- Guidelines on Programmatic Management of Drug Resistant TB (PMDT) in India, CTD, MoHFW, India, 2021.
- Training Modules (1-4) for Programme Managers and Medical Officers, CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The shorter oral Bdq-containing regimen should not be administered to pregnant women until how many weeks? 20 22 30 32 4 The shorter oral Bedaquiline-containing MDR/RR-TB regimen should not be administered in pregnant women before 32 weeks as it can cause Ethionamide (Eto)-led potential teratogenicity in the first trimester and risk of hypothyroidism in infants in the second trimester. Yes Yes Death Audit
ContentA death review or mortality audit is a means of documenting the causes of death and the factors that contributed to it, identifying factors that could be modified and actions that could prevent future deaths, putting the actions into place and reviewing the outcomes.
The aims of the audit or review of deaths in hospitals and health services are to:
- Ensure that all deaths are identified and discussed, and confidentiality is maintained.
- Assign a cause or causes to each death.
- Determine whether the care given was consistent with evidence-based clinical practice, standards of care or the care desired by professionals.
- Determine the social, environmental and nutritional risk factors for any death.
- Determine possible modifiable factors in the care of each person who dies.
- Change modifiable factors to improve the quality of care and avoid similar deaths in the future.
- Improve the quality and completeness of patient documentation.
- Provide an opportunity for reflection and support to HCWs.
- Let families know that their relative’s life was valued, the death is being taken seriously and HCWs are committed to learning and improving their practice.
Under the National TB Elimination Programme (NTEP), death audits provide insights into the chain of social, economic and clinical events leading to TB deaths and guide the programme in taking appropriate actions to prevent them.
Process for Undertaking Death Audits
An overview of the process for undertaking a TB death audit is shown in the figure below. Under NTEP, the following stakeholders are involved in the process:
- The medical officer should conduct an in-depth audit of all the deaths occurring amongst TB patients irrespective of initiation of treatment.
- Similarly, the District TB Officer (DTO) should conduct the death review of all Multidrug-resistant TB (MDR-TB) patients who died.

Figure: Overview of the process for undertaking a TB death audit
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- A Guide to Conducting TB Patient Mortality Audits using a Patient-centered Approach, KNCV, USAID and MSH, 2012.
- Operational Guide for Facility-based Audit and Review of Paediatric Mortality, WHO, 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is true about death audits?
A death audit is a means of documenting the causes of death and the factors that contributed to it.
It helps in identifying factors that could be modified and actions that could prevent future deaths.
It can be conducted via a community-based death review
All of the above
4
A death review or mortality audit is a means of documenting the causes of death and the factors that contributed to it, identifying factors that could be modified and actions that could prevent future deaths, putting the actions into place and reviewing the outcomes. It is conducted via two main methods: Community-based Death Review and Facility-based Mortality Audit.
Yes Yes Which of the following stakeholders are responsible for conducting death reviews under NTEP?
Treatment supporters
Medical officers
State TB officers
None of the above
2
The medical officer should conduct an in-depth audit of all the deaths occurring amongst TB patients irrespective of initiation of treatment.
Yes
Yes
Fullscreen

