-
CDST_LT: Epidemiology and burden of TB
FullscreenTuberculosis
Content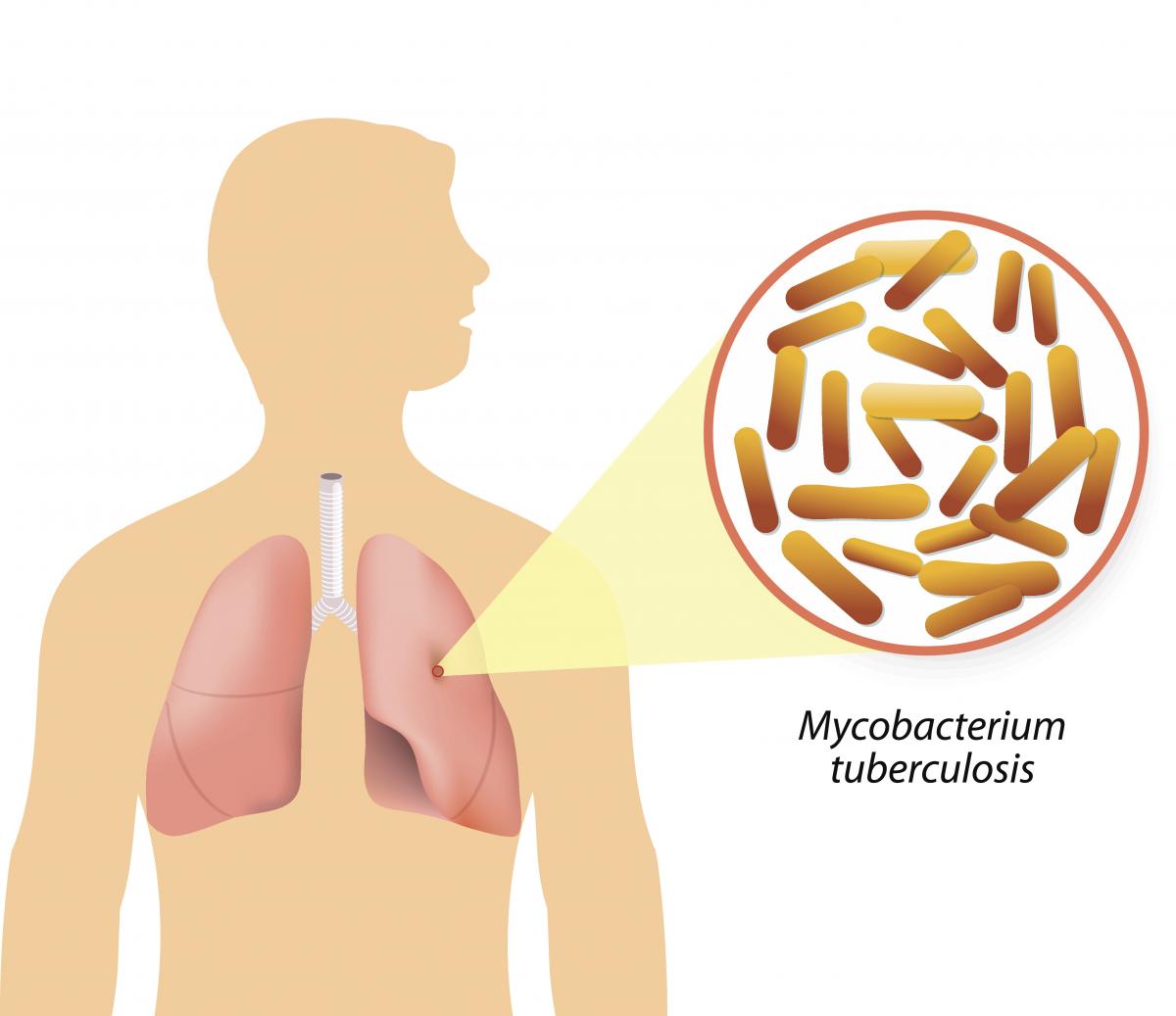
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Exposure to TB Bacilli
ContentPatients suffering from microbiologically confirmed pulmonary TB (PTB) constitutes the most important source of infection.
- The infection occurs most commonly through droplet nuclei generated by coughing, sneezing etc., inhaled via the respiratory route.
- M. tuberculosis spreads from the respiratory tract in small respiratory droplets or within dust particles that can travel long distances in the air.

Figure: How Exposure to TB Bacilli Happens
The chances of getting exposed and infected depend on the:
- Duration of exposure to an active TB patient
- Frequency of exposure
- Bacterial load of the TB patient
- Virulence of TB bacilli
- Immune status of the exposed individual
- Other factors (air circulation, overcrowding, temperature and humidity etc.)
Resources
- Robbin's Basic Pathology, 10th Edition, 2018.
- Training Module (1-4) for Program Managers and Medical Officer, NTEP, MoHFW, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Risk Factors for TB Disease
ContentFollowing are the risk factors that increase the chances of developing TB disease in an individual:

Figure: Risk factors for developing active TB
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
-
CDST_LT: Introduction to NTEP
FullscreenIndia's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
-
CDST_LT: General concepts in TB care in India
FullscreenMandatory Notification of TB Diagnosis
ContentTB is a notifiable disease in India, and TB notification has been made mandatory at the point of diagnosis since May 2012. This means that when a case of TB is diagnosed and/or put on treatment it is to be reported to the NTEP.
- Every healthcare provider, i.e., clinical establishments run or managed by the Government (including local authorities), private or NGO sectors and/or individual practitioners, need to notify diagnosed or treated TB patient’s.
- Reporting is to be done on the online reporting system called Nikshay and should include details of patient identification, and TB diagnosis.
- This, apart from enabling essential public health actions such as Treatment initiation, and Contact Tracing, chemoprophylaxis, but also enables provisions of Direct beneficiary transfer for Nikshay Poshan Yojana
Points to Note:
As per MCI code of ethics a registered medical practitioner giving incorrect information on his name and authority about notification amounts to misconduct and such a medical practitioner is liable for deregistration. It is the duty of the registered medical to divulge this information to the authorized notification official as regards communicable and notifiable diseases.
Resources
Nikshay
ContentNikshay is an Integrated ICT system for TB patient management and care in India. Nikshay was launched in 2012 and since then, various improvements have been made in the system.
Nikshay provides-
- A Unified interface for public and private sector health care providers
- Different types of Logins such as State, District, TU, PHI, Staff logins, Private providers, Chemist, Labs and PPSA/JEET Logins
- Integration of all adherence technologies such as 99DOTS and MERM
- Unified DSTB and DRTB data entry forms
- Mobile friendly website with mobile app
Nikshay is accessible either via web browser(https://Nikshay.in ) or mobile App called ‘Nikshay’ that can be downloaded from Google Play Store(Android).
Figure: Nikshay Login Pages
TB Case classification in NTEP
ContentTB cases are generally classified on the basis of previous history of TB treatment into New and previously treated cases.
New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated (cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up - A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Classification of TB on the basis of Drug Resistance
ContentResistant Sensitive Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistant to Isoniazid (H) Rifampicin (R) Fluroquinolones (FQ) =
Ofloxacin, Levofloxacin,
MoxifloxacinGroup A Drugs =
Bedaquiline/ LinezolidH Mono / Poly Drug Resistance Resistant Sensitive Unknown/ Sensitive Unknown/ Sensitive Rifampicin Resistance (RR) Unknown/ Sensitive Resistant Unknown/ Sensitive Unknown/ Sensitive Multi Drug Resistance TB (MDR TB Resistant Resistant Unknown/ Sensitive Unknown/ Sensitive Pre-Extensive Drug Resistance (Pre -XDR) Resistant Resistant Resistant Unknown/ Sensitive Extensive Drug Resistance (XDR) Resistant
Resistant Resistant Resistant Resources:
Development of Drug Resistance in Mtb.
ContentDrug resistance in Mycobacterium tuberculosis occurs when there is acquisition of mutations in genes that code for anti-TB drug targets or drug-activating enzymes.
Drug resistance in Tuberculosis (TB) occurs through two main mechanisms shown in the figure below.
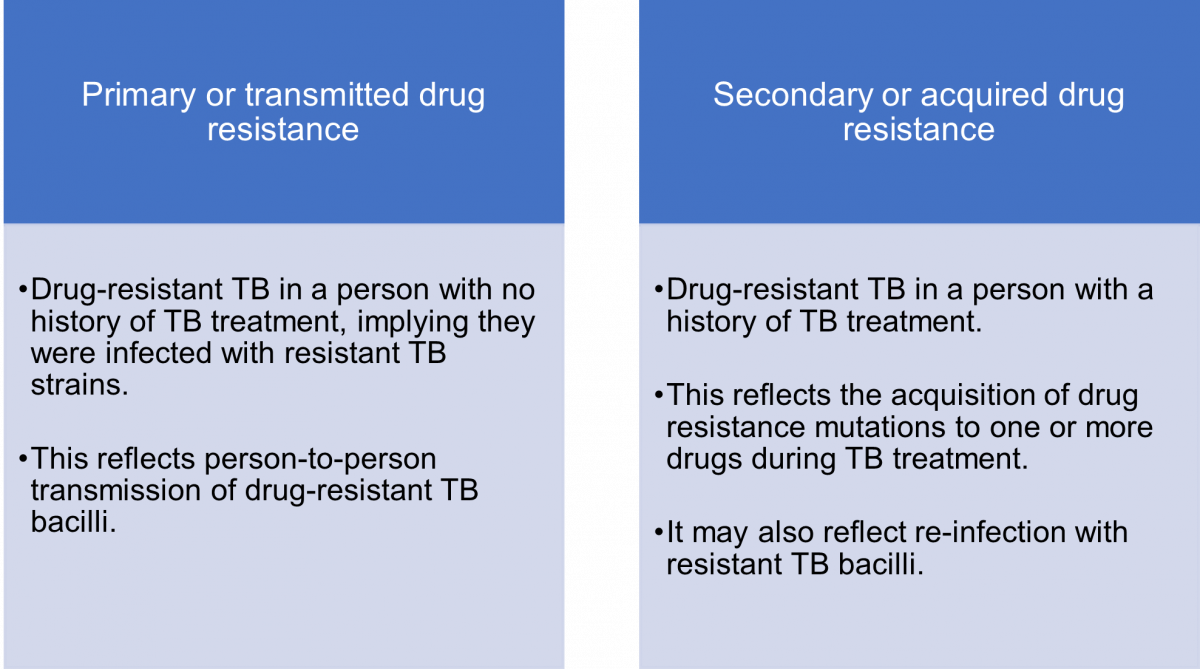
Figure: Mechanisms or Types of Drug Resistance in TB
The mechanism of transmission of drug-resistant (DR) and drug-sensitive (DS) TB is the same i.e., via infectious aerosols.
Acquired drug resistance is multi-factorial, and may be due to:
- Lack of access to quality-assured anti-TB drugs for proper treatment
- Lack of adherence to the regimen or interrupted therapy which could be due to complex dosing strategies, serious adverse drug reactions and drug–drug interactions
- Inappropriate regimens
- Sub-therapeutic dosing
- Use of expired or substandard anti-TB drugs
- Malabsorption of oral anti-TB drugs which can be seen, for example, in HIV patients.
Resources
- Navisha Dookie et al. Evolution of Drug Resistance in Mycobacterium tuberculosis: A Review on the Molecular Determinants of Resistance and Implications for Personalized Care, Journal of Antimicrobial Chemotherapy, Volume 73, Issue 5, May 2018.
- Bento J, Duarte R, Brito MC, et al. Malabsorption of Antimycobacterial Drugs as a Cause of Treatment Failure in Tuberculosis, BMJ, September 2010.
- Biadglegne F, Sack U, Rodloff A. Multidrug-resistant Tuberculosis in Ethiopia: Efforts to Expand Diagnostic Services, Treatment and Care. Antimicrobial Resistance Infection Control, 2014.
Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Continuum of TB Care
ContentWhat is the "continuum of TB Care"?
Tuberculosis in contrast to other infectious diseases affects humans over a long period of time. Stages such as uninfected, infected, and disease, do not have clearly demarcated time points and stages blend with each other when a person is converting or transitioning from one to the other. In addition, a person cured from TB may get re-infected and diseased, or still harbor a few dormant TB bacteria which may get reactivated at some future time; this too needs to be cared for. Hence, TB care is visualized as a continuous spectrum of care, with parts that requires varying type and intensity of services throughout a person's lifecycle, called the continuum of care.
Continuum of TB care is a concept that emphasizes that care provision/ TB related health care services exists is in a continuum for an individual's lifetime. It includes services before and after the current episode of TB including vulnerable population, TB infection, post treatment follow-up and recurrence of TB.
NOTE:
- When interacting with a person it is important to locate the person in this continuum of care. This is done by a combination of screening for TB disease, testing for TB infection, asking for the previous history of TB/ checking for existing records in Nikshay using patient identifiers.
- In alignment with the continuum of care concept, Nikshay follows a lifecycle approach. It is able to document and track a patient throughout the continuum using any of the Patient ID or Episode ID or any of the service identifiers(Test ID, Transfer ID etc).
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
- Standards for TB Care in India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Continuum of care involves a life cycle based approach toward delivering healthcare services for TB. True False 1 Continuum of care means that delivery of services under NTEP is in a continuum for an individual's lifetime and extends beyond the current episode of TB. Symptoms of TB Disease
ContentActive TB disease has 4 major symptoms (the 4 Symptom complex). Presence of any one of these symptoms without any other reason warrants evaluation for TB. These are:

Figure: Signs and Symptoms of TB
People affected with TB may experience other symptoms as well. These may be based on the site that is affected with TB or other more non-specific symptoms of an infection. The physician or doctor would evaluate these symptoms in view of diagnosis of TB.
Resources:
Screening For Tuberculosis Disease
ContentScreening for active tuberculosis (TB) a process to filter out people who are less likely to have TB, from a group. Screened positive people are likely to have TB and are confirmed subsequently using a TB diagnostic test. This will allow finite diagnostic testing resources to be used on the remaining.
Screening in TB may be performed using simple field tools (4 Symptom complex) and tests such as Chest X-ray, or a combination of both. Combination of both is the most effective, but is often not applied due to the practical difficulties in making a chest X-ray conveniently available.
Screening is an integral part of any general case finding effort. It is also applied systematically in specific situations.
- At health care facilities (intensified case finding): Here those visiting are screened using the 4 symptom complex, often at the point of entry to the facility. Those screened positive may be fast-tracked to TB Diagnostic testing.
- In vulnerable populations in active case finding efforts: Here the entire population identified for active case finding are screened using the pre-decided protocols by going door to door.
Resources
Testing for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
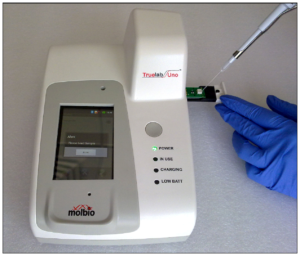
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
-
CDST_LT: Nikshay The NTEP Information System
FullscreenUser roles managing patient data in Nikshay
ContentNikshay being the final updated repository of information of TB patient services, different roles perform various actions on the patient and TB service information in Nikshay and keep it updated. These roles range from health volunteers and treatment supporters on the field to health providers and doctors at health facilities. Each role acts on or inputs information based on the services he/she provides. The information is required to updated when it is generated by the person generating it (eg by the CBNAAT LT once the results of a CBNAAT test is available).
- Laboratory Technician (LT): This role encompasses LTs at all labs performing all types of TB related tests including those at District Microscopy Centre (DMCs), Cartridge Based Nucleic Acid Amplification Test (CBNAAT) and Culture and Drug Sensitivity Test (CDST) laboratories. The LT is responsible for adding and updating test records (Test request and test result) in Nikshay that he/she performs. Nikshay in-turn provides the LT with the electronic register of tests performed at the PHI and also shares the updated information with other relevant stakeholders.
- Treatment Supporters and Health Volunteers: These field level volunteers (such as ASHAs) may enroll presumptive TB cases and refer them to the nearest PHI. Once a TB case is identified and linked to them for treatment support they can record and monitor TB patient adherence. Nikshay in-turn provides them with updated information of the patient and automatically calculates Treatment Supporters honorarium and enables its processing by the relevant authorities.
- Patients: Patients may view their updated TB health records including adherence information and status of DBT benefits processing in Nikshay through the TB Arogya Saathi Application.
- Pharmacist/ Storekeeper: These ensure drug dispensation records of patients are updated along with related supply chain information in Nikshay and Nikshay Aushadhi.
- Health Staff: This is a group of roles posted to various PHIs(Peripheral Health Institutions) and their catchment geographies, ranging from CHOs and MPHWs to Medical officers of the PHI. They are responsible for ensuring that all records related to all patients in their catchment area, encompassing all functions from enrollment to post treatment follow-up. The Medical Officer/ Doctor in-charge apart from being the final accountable authority for ensuring updated and correct information is present in Nikshay, he/she needs to review and record treatment initiation (along with treatment regimen) and clinical decision in Nikshay with support from his/he health staff.
- Senior Treatment Supervisor (STS)/ Senior TB Lab Supervisor (STLS)/ TB Health Visitor: These roles train and support the above staff in ensuring that the information in Nikshay is up-to-date. They also review reports and coordinate feedback to the other staff to ensure optimum patient services.
The overall responsibility of ensuring completion of real-time updating of information/ data in Nikshay lies with the District TB Officer (DTO). The DTO is responsible for ensuring that the relevant staff are trained in the use of Nikshay.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test When and by whom are the results of a laboratory test updated? By the LT at the end of the month By the LT at the end of the day By the LT once the test result is available By the STLS when he/she visits the lab 3 The information is required to be updated when it is generated by the person generating it. Yes Yes Patient and Process identifiers in Nikshay
ContentPatient Identifiers are key for identifying a patient in the Nikshay. Ideally, there should be only one identifier for each patient which identifies patient as well as processes for lifetime. However, during the continuum of care, one identifier may not be appropriate to represent the episodes and other processes. Hence there are various ids which are tagged to one patient in Nikshay. Knowing each ID and its purpose is therefore important. The various IDs that are present in Nikshay and their purpose are described below:
- Patient ID: In Nikshay, a TB patient can be identified by their Name, Patient ID and Nikshay ID. Since, patients might get enrolled at one primary health institute (PHI), diagnosed at another and initiated on treatment at a different PHI, the ID has been simplified to a unique number.
- Episode ID: In a life cycle approach, a person needs to be tracked across episodes of TB known as the Episode ID. In the first episode, the Patient ID = Episode ID (will be numerically equal), the patient is notified and completes one treatment cycle (Diagnosis to outcome). However, the patient may continue to have TB or have TB again at a later point in time. This is recorded as a second notification and becomes the second Episode of TB. A patient may be identified in Nikshay using a global search by both Episode ID and Patient ID.
- Test ID: When request for a laboratory test and test result for a patient is added under Nikshay, it generates a unique Test ID. For multiple tests added a new Test ID is generated for a patient.
- Transfer ID: In Nikshay, a transfer request of patients between health facilities across the country feature is enabled. Users make requests of two types - “Transfer In” and “Transfer Out”. This process generates a unique Transfer ID for the patient. The details of Transfer In and Transfer Out with Transfer ID are available in Nikshay’s Transfer Management feature.
- Sample ID: It is essential that patient samples are registered in Nikshay. While “Adding Test(s)” when sample details are added, Sample IDs are auto-generated. Sample IDs help to track samples in Nikshay using this unique ID.
- Benefit ID: A “Benefit” defined in the Nikshay-PFMS (Public Finance Management System) is a payment due to a beneficiary under a particular scheme. For example, in Nikshay Poshan Yojana (TB Patient Nutritional Support Scheme), the beneficiary is a case of Tuberculosis, notified to Nikshay. This beneficiary under the scheme is eligible for Rs 500 for each treatment month. Thus Nikshay generates a Benefit ID that identifies the patient eligible for benefits @ Rs. 500 for each treatment month.
- Beneficiary ID: A beneficiary is a person/ citizen who is eligible to get benefits (financial or in kind) under any government scheme. Whenever Nikshay identifies a potential beneficiary, it issues a unique beneficiary ID to it. All the benefits processed or paid to a beneficiary are tracked using the Nikshay Beneficiary ID. For example, if a patient has multiple episodes, all the benefits of the patient across episodes are managed using the Beneficiary ID. This information is available in the Beneficiary register exported from Nikshay.
- Ayushman Bharat Health Account (ABHA) ID: The Ayushman Bharat Digital Mission (ABDM) aims to develop the backbone necessary to support the integrated digital health infrastructure of the country. Ayushman Bharat Health Account (ABHA) ID is a 14-digit number which can uniquely identify persons and authenticate them (previously known as Health ID). It can be used to access and digitally share one's health records, with consent. ABHA is integrated into Nikshay and addresses ABHA creation, capture and verification for seamless patient registration in Nikshay. Nikshay uses the Aadhaar verification services provided by NDHM (National Digital Health Mission) to generate ABHA.
Resources
- Nikshay-search for a patient, how to identify Nikshay ID/Patient ID, how to register a patient, Adding a new Episode, how to generate Test ID, Transfer Management, Sample ID generation_Diagnostics, Direct Benefit Transfer Manual, Training Video on Direct Benefit Transfer, ABHA Workflow
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is NOT a patient or process identifier on Nikshay? Ayushman Bharat Health Account (ABHA) ID Patient ID Mother’s ID Benefit ID 3 Mother’s ID is not a patient or process identifier on Nikshay. Yes Yes Nikshay interfaces- Web and Mobile application
ContentFigure: Nikshay Home Page
After login in Nikshay, using the login credential shared by NTEP Health Staff, Treatment Supporter will be able to access the following button:
- New Enrolment: Allows to enrol new cases in Nikshay
- Search Patient: Allows to search for patients that are mapped to him /her, using Patient Name, Nikshay ID and Old Nikshay ID
- Add Patient Test: Allows to add tests for all the patients.
- Diagnosis Pending: View the list of the patients that are pending for diagnosis
- Not on Treatment: View the list of the patients that are diagnosed but pending to be initiated on treatment
- On Treatment Patients: Gives the list of on treatment patients
- Outcome assigned: Gives the list of the patients that have completed their treatment
- Training Material; Access the training content available on Nikshay
- Patient Summary: Gives a brief overview on the Presumptive cases registered, Diagnosed and patients that are initiated on treatment
- Task List: Allows to view the list of pending activities pertaining to adherence, Treatment Outcome and Bank details missing for mapped patient
- Latest Updates: New updates of features that are released on Nikshay
TB Arogya Saathi Application
ContentTB Aarogya Sathi empowers Citizens (including TB Patients under NTEP) and to serve as a Direct interface with the national TB program.
Citizen: The App is aimed at increasing awareness among the citizens. It is available for all Citizens using the App (no login required to access this content)
- Information on TB (Symptoms, Side Effects)
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Nutritional Advice
Patient: Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
- Patients registered under Nikshay get access to their TB health record additional information (after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code


Figure: TB Aarogya Sathi Application snapshot
Resources:
Enrolling a patient in Nikshay
ContentVideo file
Fullscreen