Goals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentThe Medical Officer (MO) of the referring health facility initiates TB treatment on receipt of the diagnostic test results. All efforts are made to initiate the treatment at the earliest.
The treatment regimen is decided based on the type of patient and TB (based on drug sensitivity pattern, i.e., drug-sensitive TB or H-mono/ poly resistance, history of adverse drug reaction to anti-TB drugs).
The patient needs constant support of a health volunteer or peer, who can monitor the treatment, help him in getting a follow-up, keep him motivated, counsel the family/ contacts, etc. These health volunteers/ peers are called treatment supporters in NTEP.
The steps in treatment initiation include:
- The MO performs a clinical evaluation of the patient and assesses for comorbidities.
- Counselling of TB patients and their families should be done.
- Peripheral health worker/ treatment supporters responsible for monitoring treatment adherence and treatment providers acceptable to the patient should be assigned.
- A treatment card should be opened for each patient.
- Each patient should be given a TB Identity Card.
- Drugs should be made available at the treatment centre.
- Public health action for all notified TB patients should be initiated.
All the process related to patient treatment initiation should be documented in Nikshay.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What key activities are included during TB treatment initiation?
Clinical evaluation
Counselling
Treatment card and TB ID card opened, Nikshay updated with treatment details
All the above
4
During TB treatment initiation the key activities include clinical evaluation of the patient; counselling of patient and family members; opening of treatment card and TB ID card and updating of treatment details on Nikshay.
Yes
Yes
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Closing Cases and Assigning Treatment Outcomes
ContentVideo fileVideo:
Closing Cases and Assigning Treatment Outcomes (Web)
Video fileVideo:
Closing Cases and Assigning Treatment Outcomes (Mobile)
Adverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
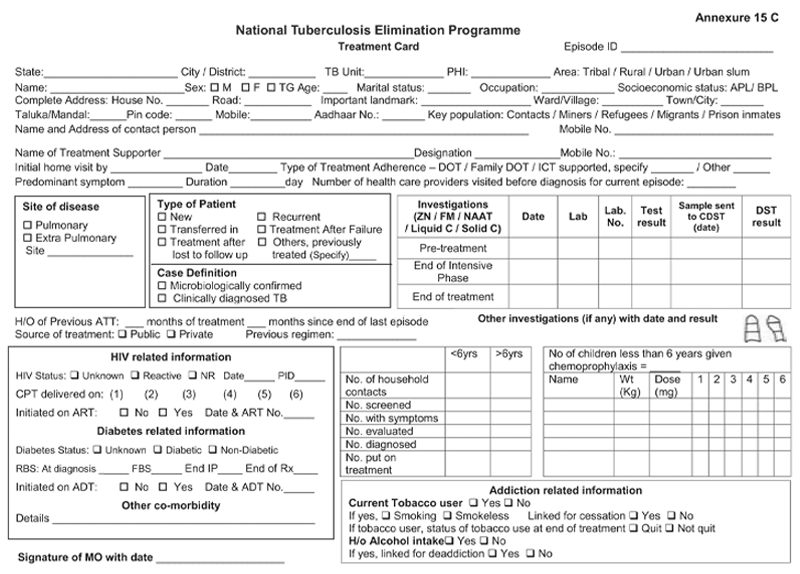
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
Follow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
Fullscreen

