Tuberculosis
Content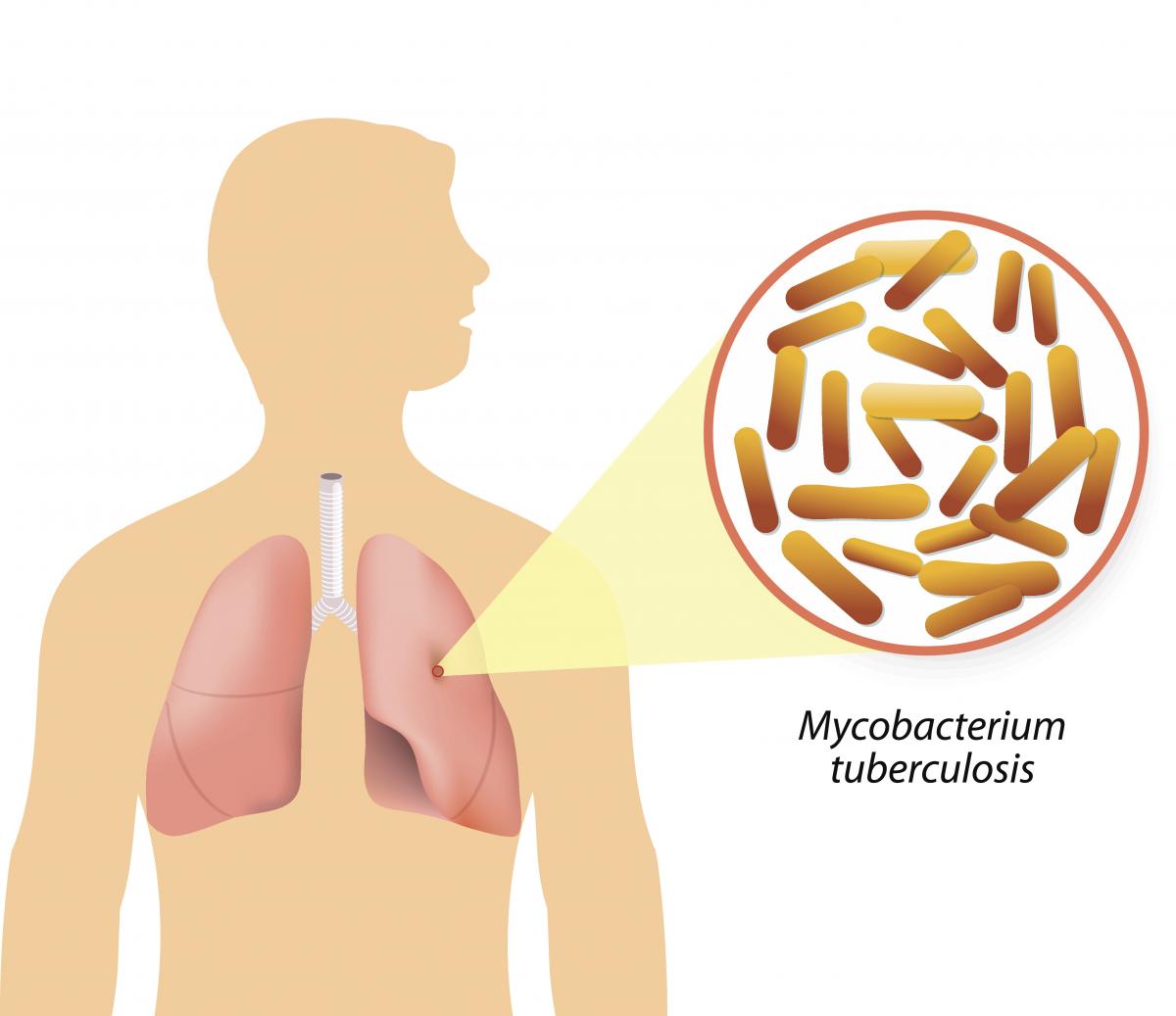
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Pathogenesis of TB
ContentTuberculosis (TB) is an infectious, chronic, granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the body.
The pathogenesis of TB in a previously unexposed immunocompetent individual is centred on the development of cell-mediated immunity. This confers resistance to the organism and results in the development of tissue hypersensitivity to tubercular antigens.
The pathologic features of TB, such as caseating granulomas and cavitation, result from the destructive tissue hypersensitivity that is part and parcel of the host immune response.
The sequence of events from inhalation of the infectious droplets to the containment of the primary focus of infection is as follows:

Figure: Pathogenesis of Tuberculosis
In many individuals, the stage 5 response (from above) halts the infection before significant tissue destruction or illness occur (Latent TB Infection). In other individuals with immune deficits due to age or immunosuppression, the infection progresses to stage 5, and the ongoing immune response results in caseation necrosis (Active TB Disease). The figure above provides more details on the progression of TB disease.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Epidemiological Triad of TB
ContentThe Epidemiologic Triad is a model used in the field of epidemiology to study diseases and how they are spread. It consists of a triangle with three vertices or corners.
The three vertices for infectious diseases consist of:
1. Agent, or microbe that is the factor causing the disease.
2. Host, or organism harbouring the disease.
3. Environment, or those external factors that cause or allow disease transmission.
In the Epidemiological Triad of TB (Figure), the agent is the TB causing bacteria Mycobacterium tuberculosis; the host refers to humans that are susceptible to TB. Susceptibility or the risk factors for acquiring TB can be:
- Close contact with a person having TB disease
- Nutritional status of the host
- Existing co-morbidities
- Low immunity.
Susceptibility of the host can also vary due to age, gender, genetic composition, race, ethnicity, etc.
As TB is an airborne disease, environmental factors come into play for the transmission of TB. These include crowding, poor ventilation, bad sanitation, indoor air pollution, etc.
The understanding between the interplay of agent, host and environment is essential to understanding the epidemiology of TB and taking measures to control it. The risk of TB due to environmental factors can be reduced by practising airborne infection prevention measures like good ventilation, hand hygiene and cough etiquette.

Figure: Epidemiological Triad of TB
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The three vertices of the Epidemiological Triad are agent, host and environment.
TRUE FALSE 1 The three vertices of the Epidemiological Triad are agent, host and environment.
Yes Yes Agent in TB
ContentMycobacterium tuberculosis (M. tuberculosis) belonging to the family Mycobacteriaceae cause Tuberculosis (TB).
These are rod shaped bacilli and require oxygen to survive (aerobic bacteria).
The following characteristics of these bacilli help them to survive in human body for a long time and resist the action of drugs:
- Slow growing bacteria (replicates every 12-24 hours)
- Tough, hydrophobic cell wall rich in mycolic acid that resists action of many drugs including antibiotics.
- Ability to remain in dormant stage inside host tissues for many years in conditions with limited oxygen and nutrition (facultative anaerobes). They can revert to active state when favourable conditions (reduced host immune response, undernutrition etc.) ensue. The persistence of the bacteria in the host tissue for long duration of time is responsible for prolonged incubation period and re-activation of infection.
- The multiple mechanisms of drug resistance by the bacteria give rise to multi-drug resistant and extensively drug-resistant tuberculosis.
These characteristics make tuberculosis a chronic granulomatous disease that requires special antibiotics for treatment.
Resources
- Antimicrobial Resistance in Mycobacterium tuberculosis: Mechanistic and Evolutionary Perspectives, FEMS Microbiology Reviews, May 2017.
- The Biology of Mycobacterium tuberculosis Infection, Mediterranean Journal of Hematology and Infectious Diseases, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation PageID Part of pre-test Part of post test M. tuberculosis bacilli can survive conditions with limited oxygen. This means they are: Strict aerobes Strict anaerobes Facultative anaerobes None of the above 3 M. tuberculosis requires oxygen. However, they can survive in limited oxygen conditions also and can enter a dormant stage. They revert to active state when favourable conditions ensue. Thus, they are facultative anaerobes. Yes Yes Host factors in TB
ContentHost factors in TB disease are various factors/attributes of the host(person who is developing TB disease/infection).
The various host factors are as follows:
- Age: TB can affect people of any age. Young adults (15-30 years of age) are seen to have high rates of disease in India. Children and the elderly are also high-risk groups for the contraction of the disease.
- Gender: TB affects all genders, but males have higher disease rates, probably owing to higher levels of exposure to the bacteria in occupational settings.
- Immunity status: Individuals with compromised immunity status, like those on corticosteroid therapy/ immunosuppressants after organ transplant, HIV infection, diabetes mellitus etc., are more prone to TB infection and disease.
- Nutritional status: Undernutrition causes weakening of the immune system and hence predisposes to TB. Risk of TB increases by about 14% with each unit reduction in Body Mass Index (BMI).
- Previous TB infection: Individuals who are close/ household contacts of confirmed pulmonary TB patients; individuals residing in TB high-prevalence regions; high-risk groups like healthcare workers, homeless people, HIV infected etc., have high chances of being already infected with TB and hence, would progress to disease.
Resources
- India TB Report 2021, Central TB Division, MoHFW, Government of India.
- TB Risk Factors, Centers for Disease Control and Prevention.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Pick the correct statement for the causation of TB disease. Undernutrition causes TB disease. HIV infection compromises the immune system and may lead to TB disease. Children do not develop TB disease. The elderly are not at high risk for developing TB disease. 2 - HIV infection weakens the immune system of an individual and predisposes him/her to TB infection and disease.
- Undernutrition, as such, is not a causative factor for TB, but it weakens the immune system and predisposes to the infection/ disease.
- Children and the elderly are at high risk for TB.
Yes Yes Environmental influences in TB
ContentEnvironmental conditions have a huge role in the development of TB disease and are an important component of the epidemiological triad for TB disease.
The various environmental factors influencing TB are:
- Poor housing and ventilation: Damp homes, often resulting from condensation due to inadequate ventilation, allow the growth of mold, fungi, and other microorganisms. This adversely affects the respiratory health of individuals and increases the chances of the spread of TB from a patient to his/her household contacts.
- Overcrowding: More people living within a single space restricts movement, gives scope for lack of privacy and limits hygiene. The extent and persistence of contact with an infected person increases. The droplet nuclei (due to coughing) from infected individuals can stay in the air for a long time and transmit the disease easily to contacts.
- Indoor air pollution: The use of traditional biomass fuels like cow dung, wood etc. for energy generation (especially for cooking) in poorly ventilated households pose serious risks to the lung health of individuals. Damaged lungs are more susceptible to TB infection/ disease.
- Occupational environment: Healthcare workers, miners etc. are at a high risk of TB. Inadequate air change rates, negative airflow and recirculation of air have been identified as occupational hazards in hospitals with respect to TB transmission.
Resources
- Role of Environmental Factors in Transmission of Tuberculosis, Dynamics of Human Health, 2015.
- Housing and Public Health, Annual Review of Public Health, 2004.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How does poor housing contribute to TB transmission?
Poor ventilation measures
Increased dampness in the ambient air
Indoor air pollution
All of the above
4
Poor housing usually arises as a result of poverty, wherein the nutritional status and hence immunity of inhabitants are already low, which predisposes them to TB. Adding to it, structural faults like poor ventilation, the resultant increase in droplets in the air and poor smoke escape from the burning of solid fuels also contribute to TB transmission.
Yes Yes TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Natural History of TB
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
Development of Drug Resistance in Mtb.
ContentDrug resistance in Mycobacterium tuberculosis occurs when there is acquisition of mutations in genes that code for anti-TB drug targets or drug-activating enzymes.
Drug resistance in Tuberculosis (TB) occurs through two main mechanisms shown in the figure below.
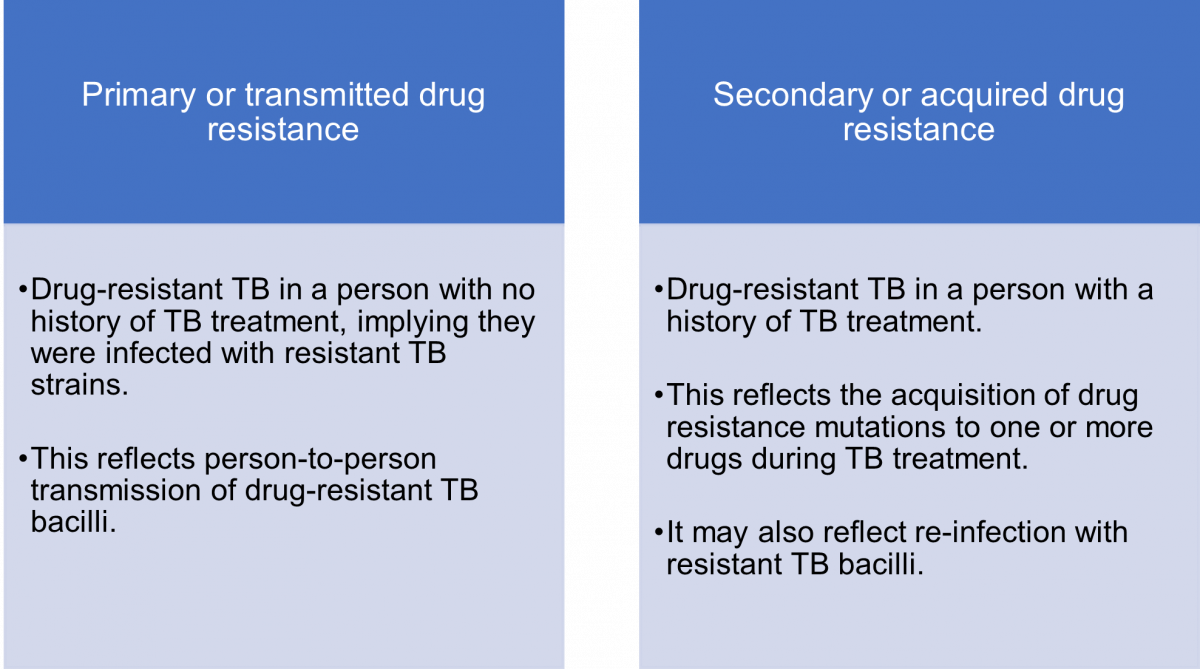
Figure: Mechanisms or Types of Drug Resistance in TB
The mechanism of transmission of drug-resistant (DR) and drug-sensitive (DS) TB is the same i.e., via infectious aerosols.
Acquired drug resistance is multi-factorial, and may be due to:
- Lack of access to quality-assured anti-TB drugs for proper treatment
- Lack of adherence to the regimen or interrupted therapy which could be due to complex dosing strategies, serious adverse drug reactions and drug–drug interactions
- Inappropriate regimens
- Sub-therapeutic dosing
- Use of expired or substandard anti-TB drugs
- Malabsorption of oral anti-TB drugs which can be seen, for example, in HIV patients.
Resources
- Navisha Dookie et al. Evolution of Drug Resistance in Mycobacterium tuberculosis: A Review on the Molecular Determinants of Resistance and Implications for Personalized Care, Journal of Antimicrobial Chemotherapy, Volume 73, Issue 5, May 2018.
- Bento J, Duarte R, Brito MC, et al. Malabsorption of Antimycobacterial Drugs as a Cause of Treatment Failure in Tuberculosis, BMJ, September 2010.
- Biadglegne F, Sack U, Rodloff A. Multidrug-resistant Tuberculosis in Ethiopia: Efforts to Expand Diagnostic Services, Treatment and Care. Antimicrobial Resistance Infection Control, 2014.
Causes for Drug-resistant Tuberculosis
ContentDrug resistance is caused by a genetic mutation that makes the drug ineffective against the mutant bacilli.
The causes of drug-resistant TB can be enumerated as follows:
1. Providers/ Programme Related Causes:
- Inadequate or poorly administered TB treatment regimen
- Unavailability or poor quality of anti-TB drugs
- Poor monitoring of TB treatment
- Delay in detection and management of DR-TB
2. TB Patient/ Host Related Causes:
- Clinical characteristics of TB patients leading to suboptimal drug levels in blood (e.g. Malabsorption syndrome)
- Irregular anti-TB treatment due to any reason (e.g. socio-economic barriers, substance abuse, Adverse Drug Reactions (ADRs), psychological and other factors)
There are two principal causal pathways leading to the development of drug-resistant TB:
- Primary drug resistance: It means that a person has been infected with a drug-resistant TB strain.
-
Acquired (Secondary) drug resistance: It is the result of inadequate, incomplete or poor treatment quality that allows the selection of mutant resistant strains.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Chemotherapy and its implication in TB control
ContentChemotherapy for TB is the use of an anti-TB drugs to kill, or prevent the replication of, TB mycobacteria in the patient’s body. Effective anti-TB chemotherapy renders the patient non-contagious and cures the patient, thereby interrupting the chain of transmission. Mortality rates of TB range from 50-80% in untreated smear-positive individuals and drop to lower than 5% under chemotherapy.
Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment. TB disease must be treated for at least 6 months and in some cases even longer. The use of multi-drug therapy reduces the incidence of drug-resistant cases and increases the overall effectiveness of treatment.
If treatment is interrupted, any surviving bacteria may cause the patient to later become ill and infectious again, potentially with drug-resistant disease.
How infectious are tuberculosis patients under chemotherapy?
Under effective chemotherapy, there is a substantial decline in infectiousness in two weeks time, and may not be a major source of risk to any contacts. This decline is indicated by the rapid fall in the number of viable organisms in the sputum, and reduced frequency of coughing.
Types of Chemotherapy in TB
- Preventive Chemotherapy: Regimen for healthy but TB infected persons with a high risk of developing TB, in order to prevent them from developing TB.
- Standard Chemotherapy: Two-phased chemotherapy for an average of 6-8 months based on the combination of at least four major drugs (HRZE) given for 2 months during the initial intensive phase of treatment and followed by a combination of at least 2 drugs given for at least 4 months during the continuation phase of treatment.
- Chemotherapy for Drug-resistant TB: Two-phased chemotherapy varying from 9 - 24 months in patients having demonstrated resistance to drugs used in standard chemotherapy. The regimen varies with the drug to which the resistance is present, however, each regimen contains a mix of second-line anti-TB drugs including injectables.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Infectiousness and Host Susceptibility, The Journal of Infectious Diseases, Vol. 216, suppl_6, 2017.
- Tuberculosis chemotherapy: Current Drug Delivery Approaches, Respiratory Research 7, Article no. 118, 2006.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which type of chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB? First-line anti-TB drugs Preventive Chemotherapy Standard Chemotherapy Chemotherapy for Drug Resistant-TB 2 Preventive chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB. Yes Yes Incidence of TB Disease
ContentIncidence is an epidemiological measure of the occurrence of new cases of a disease in a population over a specified period of time. Tuberculosis (TB) incidence is the number of new cases of active TB disease during a certain time period (usually a year), and is better expressed as a rate, as shown in the figure below.


Figure: Deriving the Incidence of TB Disease for a Given Population
Tuberculosis incidence varies considerably in different populations and population segments.
In 2021, the Global TB incidence was 134 (125-143) per 100,000. The TB Incidence rate of India is - 210 (178-244) per 100,000 in 2021 according to WHO Global TB Report 2022.
Resources
- India TB Report, 2022.
- Epidemiologic Basis of Tuberculosis Control, Hans L. Rieder, 1999.
- Morbidity Frequency Measures, Centers for Disease Control and Prevention.
- Global Tuberculosis Report 2022.
Prevalence of TB Disease
ContentPrevalence is an epidemiological measure of the proportion of a population with a disease or a particular health condition at a specific point in time (point prevalence) or over a specified period of time (period prevalence).
Tuberculosis (TB) prevalence refers to the number of people with TB that are present in a particular population at a given time. Calculation of the TB prevalence rate is shown in the figure below.

Figure: Deriving the Prevalence of TB Disease for a Given Population
TB prevalence rate is derived by adding the number of persons that develop new TB disease (i.e., incident cases) and those who already have the disease (i.e., existing cases), and dividing the sum by the total population from which the cases arose.
TB prevalence varies widely and is affected by a number of factors such as age, gender, population density, rural/urban settings, as well as socioeconomic factors.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
TB Notification rate
ContentTB notification rate is the number of TB cases notified over a specified time period for a specified population, usually per lakh. It indicates how many cases have been diagnosed and informed to the National TB Elimination Program.
It is mostly calculated annually, and the calculation formula is as follows:

Figure: Deriving the Annualized TB Case Notification Rate
The National TB Elimination Program calculates TB notification rates based on TB cases notified using the digital surveillance system called Nikshay. Each state/district is provided with an annual target for TB case notification, the progress of which is measured periodically to understand efforts taken for the detection of TB cases.
Example
If the number of TB patients diagnosed in District X one year is 1000, and the mid-year population of District X is 10,00,000, then the annualized TB case notification rate is calculated as follows:
100 cases/100 000/year
Resources
TB deaths
ContentWhen an HIV-positive person dies from TB, the underlying cause is classified as HIV with TB as a contributory cause. However, the milestones and targets for reductions in TB deaths set at the End TB Strategy are for the combined total of deaths in HIV-positive and HIV-negative people.
Estimates of TB deaths in India:
Estimates of TB burden, 2020 Number (Rate per 100 000 population) HIV-negative TB mortality 493 000 (453 000-536 000) 36 (33-39) HIV-positive TB mortality 11 000 (9 800-12 000) 0.78 (0.71-0.84) In 2020, India accounted for 38% of global TB deaths among HIV-negative people, and for 34% of the combined total number of TB deaths in HIV-negative and HIV-positive people.
Note: The International Classification of Diseases (ICD) defines TB deaths as ‘death from TB among HIV-negative people'.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the definition of TB mortality rate?
Number of TB deaths per one thousand population per month
Number of TB deaths per 10 thousand population per year
Number of TB deaths per one lakh population per year
Number of TB deaths per one crore population per year
3
TB mortality rate is defined as the number of TB deaths per one lakh population per year.
Yes
Yes
Fullscreen


