Drug-Sensitive Tuberculosis(DS-TB)
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
DSTB Treatment Phases
ContentDSTB Treatment duration is of 6–9-month course of antibiotics. The duration and drug dosage used may vary according to a patient’s age, type of TB infection, and whether s/he has been treated before.
The standard 6-month course of treatment consists of two phases.
Intensive Phase(IP)
Continuation Phase(CP)
- The first phase lasts 2 months.
- 4 drug regimen(HRZE) is given as part of IP.
- The second phase lasts 4 months
- 3 drug regimen(HRE) is given as part of CP.
*Extension of CP: Depending upon response to treatment or type of disease, physician may decide to extend the treatment by 3 months.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
FDCs used in NTEP
ContentImage
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
Drug-Resistant Tuberculosis(DR-TB)
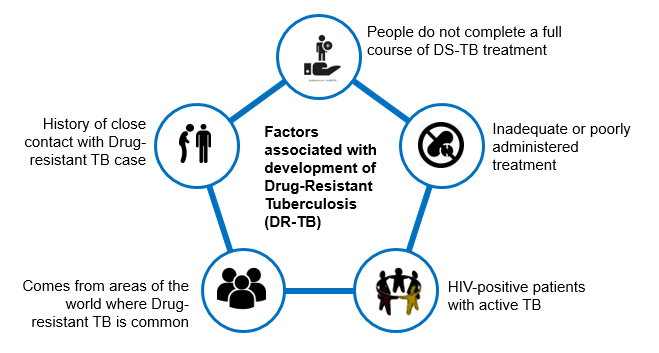
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
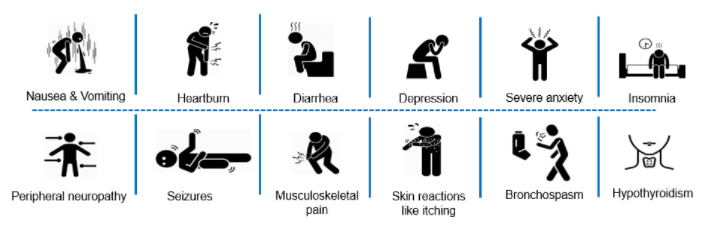
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Regimen for TPT
ContentThe following TPT treatment options are recommended under NTEP once active TB has been ruled out:
6H
3HP
Medicines
Isoniazid
Isoniazid + rifapentine
Duration (months)
6
3
Interval
Daily
Weekly
Doses
182
12
Pregnant women
Safe for use
Not Known
Post-treatment TPT for PLHIV: In patients previously treated for TB, post-treatment TPT has been considered in view of the 5-7 times higher risk of recurrence of TB among PLHIV and nearly 90% of these due to re-infection. Thus, all CLHIV/PLHIV who had successfully completed treatment for TB disease earlier should receive a course of TPT after completing treatment of TB.
Resources
-
Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
-
Latent TB Infection : Updated and Consolidated Guidelines for Programmatic Management, WHO, 2018
Kindly provide your valuable feedback on the page to the link provided HERE
-
Fullscreen